


Autoantibodies against at least 19 tumor suppressor proteins in response to spike protein presentation to the immune system.
(Sept '21)

Any extracts used in the following article are for non commercial research and educational purposes only and may be subject to copyright from their respective owners.
Background:
A tumor suppressor gene (TSG), or anti-oncogene, is a gene that regulates a cell during cell division and replication. If the cell grows uncontrollably, it will result in cancer. When a tumor suppressor gene is mutated, it results in a loss or reduction in its function.
https://en.wikipedia.org/wiki/Tumor_suppressor_gene
"From Anti-Severe Acute Respiratory Syndrome Coronavirus 2 Immune Response to Cancer Onset via Molecular Mimicry and Cross-Reactivity" (2021)
Abstract and Figures
Background and Objectives
Whether exposure to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) may predispose to the risk of cancer in individuals with no prior cancers is a crucial question that remains unclear. To confirm/refute possible relationships between exposure to the virus and ex novo insurgence of tumors, this study analyzed molecular mimicry and the related cross-reactive potential between SARS-CoV-2 spike glycoprotein (gp) antigen and human tumor-suppressor proteins.
Materials and Methods
Tumor-associated proteins were retrieved from UniProt database and analyzed for pentapeptide sharing with SARS-CoV-2 spike gp by using publicly available databases.
Results
An impressively high level of molecular mimicry exists between SARS-CoV-2 spike gp and tumor-associated proteins. Numerically, 294 tumor-suppressor proteins share 308 pentapeptides with the viral antigen. Crucially, the shared peptides have a relevant immunologic potential by repeatedly occurring in experimentally validated epitopes. Such immunologic potential is of further relevancy in that most of the shared peptides are also present in infectious pathogens to which, in general, human population has already been exposed, thus indicating the possibility of immunologic imprint phenomena.
Conclusion
This article described a vast peptide overlap between SARS-CoV-2 spike gp and tumor-suppressor proteins, and supports autoimmune cross-reactivity as a potential mechanism underlying prospective cancer insurgence following exposure to SARS-CoV-2. Clinically, the findings call for close surveillance of tumor sequelae that possibly could result from the current coronavirus pandemic.
…
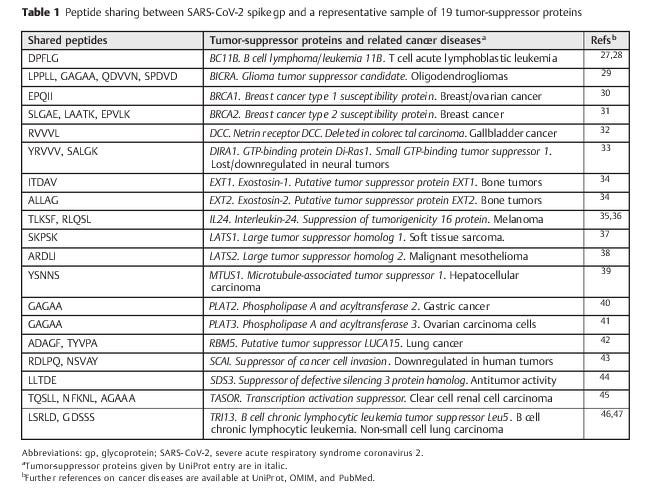
Peptide Sharing between SARS-CoV-2 Spike gp and
Tumor-Suppressor Proteins
►Table 1 shows data relative to a representative sample of 19 tumor-suppressor proteins and documents that the peptide commonality with the viral antigen amounts to 29 pentapep-tides. From a pathological perspective, ►Table 1 clearly illus-trates that even hitting only 19 out of the 294 tumor-suppressor proteins described in ►Supplementary Table S2 (available in online version only) might equate to induce or enhance carcinogenesis in almost all of the human organs, from brain and liver to lung and bones. Examples of the cancers that might be evoked/potentiated by exposure to SARS-CoV-2 in the next future are T cell acute lymphoblastic leukemia, oligodendrogliomas, breast/ovarian cancers, sarcoma, malig-nant mesothelioma, B cell chronic lymphocytic leukemia, and non-small cell lung carcinoma, among the others.
Immunologic Potential of the Peptide Sharing between SARS-CoV-2 Spike gp and Tumor-Suppressor Proteins
The gloomy outlook hinted at by the findings described in ►Table 1 becomes all the more likely in light of the high immunologic potential of the shared peptides. De facto, investigation of IEDB shows that the 29 penta peptides shared by the spike gp antigen and the 19 tumor-suppressor pro-teins (►Table 1) occur and recur in 150 epitopes derived from SARS-CoV-2 that have been experimentally validated and are cataloged as immunoreactive (►Table 2).
In essence, ►Table 2 factually supports the possibility that cross-reactions can be triggered by SARS-CoV-2 infection/active immunization and hit human proteins relat-ed to carcinogenesis. Very much this conclusion applies when considering that the extent of the potential immuno-logic cross-reactivity as well as the spectrum of potentially inducible tumors may be exponentially higher in light of the fact that ►Tables 1 and 2 refer to the peptide commonality involving only a tiny part (19 out of 294) of the human proteins that—if altered—may lead to cancer (see►Supplementary Table S2 [available in online version only] for the peptide sharing in its totality).


SARS-CoV-2 by infection or vaccination ends to divert onto available immune determinants that, in the present case, are the common determinants present in the tumor-suppressor human proteins. Pathologically, one has to consider that usually an anamnestic secondary immune response is char-acterized by high avidity and high affinity, besides being quantitatively relevant. Therefore, as a final result, exposure to SARS-CoV-2 by infection and/or vaccination can trigger immediate and violent cross-reactive attacks against the proteins that protect the human being from carcinogenesis.
Conclusion
The findings described in ►Tables 1 to 3 and ►Supplementary Table S2 (available in online version only) indicate that molec-ular mimicry and cross-reactivity between peptides common to SARS-CoV-2 and tumor-related proteins might cause/contribute to cancer epidemics worldwide in the next future. The potential cancer risk might be enhanced by immu-nologic imprinting phenomena, given the fact that the com-parative analyses shown in ►Table 3 indicate the possibility that a preexisting immune responseto previously encountered pathogens could be magnified and intensified following SARS-CoV-2 infection/active immunization. These data are disturb-ing and invite to immediately intensify clinical surveillance in oncology and to undertake rigid cancer prevention actions, including healthy lifestyle and continuous controls. It will be vital to formulate/implement actions that contemplate fast and safe procedures for clinical trials, development of specific and reliable tumor markers for diagnosis, accurate follow-up of treatments, and, administratively, medical health records, detailed registries, biobanks, health surveys, and coordinated observational studies. Never before do all the recommendations of the European plan for the fight against cancer appear current and necessary. De facto, tumors appear to be the predominant pathologies that will populate the post pandemic long COVID-19.1
Full paper:
Blood cancers can take 2-6 years to become evident, solid cancers 10+ years.