4th July ‘22: Review of the recently published paper Potential Autoimmunity Resulting from Molecular Mimicry between SARS-CoV-2 Spike and Human Proteins by Nunez-Castilla et al.
6th July ‘22: Review of From Anti-Severe Acute Respiratory Syndrome Coronavirus-2 Immune Response to Cancer Onset via Molecular Mimicry and Cross-Reactivity by Kanduc, 2021 and Molecular mimicry between SARS-CoV-2 and the female reproductive system by Dotan et al, 2021.
31st December ‘22: Review of IgG4-related diseases.
Hyperlinked contents page added. May not work on some browsers.
4th January ‘23: Soluble FAS ligand and autoimmunity.
22nd February ‘23: Abstract revised.
Any extracts used in the following article are for non commercial research and educational purposes only and may be subject to copyright from their respective owners.
This is a literature review of some of the research and articles investigating the relationship between COVID-19/spike protein and other infections, autoimmune disorders and their contribution to disease severity & long term sequalae.
It begins with warnings made by experts in their field, describes the two categories of autoimmune disorders and explains what pathogenic priming is, along with a review of the paper researching this. A selection of the autoimmune targeted proteins are described, along with pathologies associated with their dysfunction.
Subsequently published papers served to confirm the findings of Lyons-Weiler, and are discussed according to the various tissues or organs affected.
Indicative timescales from first testing positive for autoimmune antibodies to the onset of symptomatic disease for various conditions are also detailed.
The review concludes with a discussion on diagnosis and therapeutics.
Background
I was told by these officials (FDA, CDC, NIH, Moderna, & Pfizer), in confidential secret discussions, that in about 6 to 6.5 years from roll-out, in those who take the injections, they feared mass auto-immune disease and deaths, they feared viral immune escape and very problematic variants, and they anticipated constant deaths from the injections but a major number of deaths to emerge. I could not even understand exactly what they did for it was so haphazard, but these were officials. And they wanted to talk to me. To tell me ‘their truths’.
They said based on all they knew, that the COVID injections could never work, especially the mRNA platform. It never worked in the animal model and was pathological. They told me that in about 6 to 6.5 years, there will be a surge in deaths in persons who take the injections (then about 1 year ago). This was their projection. They advised me they nor their families will never (especially their children) take any of the COVID injections.1
Dr. Paul Alexander, Bachelors (Hon), MHSc, MSc, PhD, COVID-19 consultant researcher in Evidence-Based Medicine (EMB), research methodology, and clinical epidemiology, June 30th, 2022.2
Unfortunately, incoming VAERS, clinical reports, 50 year record highs in cardiovascular deaths in the UK and 9 sigma “black swan" level excess deaths from various cancers over the winter of 2022-23 appears to be confirmation that a serious, rapid decline in public health is underway. There are multiple reasons for this - part viral, part public health response.
As disease latency periods are met these figures are likely to continue to trend up from here, following a seasonal pattern of spikes followed by return to a higher baseline.
After an impassioned introduction, Dr Lyons-Weiler explains how he warned pharmaceutical companies not to use unsafe epitopes in this 14 minute speech recorded in October 20203.
Again, his reports on other safety concerns proved to be extremely prescient: 21% rate of class 3 severe AEs from the first early trial data, lack of animal safety studies, autoimmunity risk, viral protein mediated coagulation, efficacy of antivirals, and cautioned against the use of QUAT based cleaning agents around children as these are teratogenic.4
This article from 2021 by the Global Virus Network provides an excellent introduction to COVID-19 and autoimmunity5. It is important to differentiate between autoimmunity leading to inflammation and direct autoinflammatory damage. And we all experience at least low levels of autoreactivity, but this is usually asymptomatic.
COVID-19, the disease caused by SARS-CoV-2, involves at least two distinct phases. The first phase is attributed to typical progress of respiratory disease by causing fever, cough, loss of taste/smell, and other symptoms typical of respiratory infections. The second phase, which occurs less frequently, is more serious and can include a great variety of multi-organ manifestations, including lung, heart, vasculature, and central nervous system.
We will consider evidence that the latter stage of COVID-19 associates with autoimmunity. It should be pointed out that autoimmune phenomena falls into two categories: (1) the innate immune system activates adaptive B- or T-cell-mediated immune responses that lead to damaging inflammation (autoimmunity) and (2) the innate immune system causes inflammatory damage directly (autoinflammatory). In both cases, the innate immune system is intimately involved, and mostly, there is a spectrum of these patterns. It should also be noted that it can be difficult to clearly discriminate between functional and dysfunctional immune responses without an understanding of the specific correlates of protection. We will not consider situations in which autoimmunity exists prior to infection, as in the case of patients with pre-existing autoantibodies to type 1 interferons(1). Interestingly, some individuals have pre-existing stereotypic SARS-CoV-2 neutralizing antibodies, produced by naïve B cells, without any known case of viral exposure(2).
AUTOANTIBODIES
In this GVN Perspective, we will first focus on autoimmunity mediated by autoantibodies. One mechanism of autoimmunity is by molecular mimicry(3), in which a viral protein sequence resembles a cellular protein sequence. Thus, the elicited antibodies target not only the viral protein but also the related cellular proteins. The region of similarity need not be large; a stretch of a dozen or so closely related amino acid residues can result in molecular mimicry. Specifically, overlapping hexa- and heptapeptides spanning the SARS-CoV-2 spike protein were found to be homologous to a large number of peptides in the human proteome(4). This does not necessarily establish a basis for autoimmunity. However, other studies show the presence of many different autoantibodies in COVID-19 patients. We will describe these findings in detail. We acknowledge that there are many other cases. In addition, low levels of autoreactivity are common, and these did not generally manifest symptomatically.
Pathogenic priming, known as Antibody Mediated Enhanced Disease, is “a systemic inflammatory response that can result in full body skin rashes, convulsions and other serious complications when an injected individual is exposed to a wild form of the virus6.”
An epitope, also called antigenic determinant,portion of a foreign protein, or antigen, that is capable of stimulating an immune response. An epitope is the part of the antigen that binds to a specific antigen receptor on the surface of a B cell. Binding between the receptor and epitope occurs only if their structures are complementary. If they are, epitope and receptor fit together like two pieces of a puzzle, an event that is necessary to activate B-cell production of antibodies. The antibodies produced by B cells are targeted specifically to the epitopes that bind to the cells’ antigen receptors. Thus, the epitope also is the region of the antigen that is recognized by specific antibodies, which bind to and remove the antigen from the body7.”
Homologous epitopes from COVID-19 or its spike protein have a similarity to those already present in our cells, even though their function may be quite different.
In 2020, Dr Lyons-Weiler analysed SARS-CoV-2 for immunogenic epitopes, published a paper with his conclusions and, as per his speech, relayed his findings to the pharmaceutical companies8. These concerns were ignored and no changes were made to the finished products which were in development and undergoing clinical trials at the time:
Highlights
• All SARS-CoV-2 immunogenic epitopes have similarity to human proteins except one.
• Roughly one-third of the potentially targeted human proteins (putative autoantigens) are key players in the adaptive immune system.
• The list of viral/human protein matches provides clues on which epitopes or parts of epitopes might be involved in the immunopathogenesis of COVID-19 disease from SARS-CoV-2 infection.
• It also indicates which epitopes might be responsible for autoimmunological pathogenic priming due to prior infection or following exposure to SARS-CoV-2 or relatives following vaccination.
• These epitopes should be excluded from vaccines under development to minimize autoimmunity due to risk of pathogenic priming.
Abstract
Homology between human and viral proteins is an established factor in viral- or vaccine-induced autoimmunity. Failure of SARS and MERS vaccines in animal trials involved pathogenesis consistent with an immunological priming that could involve autoimmunity in lung tissues due to previous exposure to the SARS and MERS spike protein. Exposure pathogenesis to SARS-CoV-2 in COVID-19 likely will lead to similar outcomes. Immunogenic peptides in viruses or bacteria that match human proteins are good candidates for pathogenic priming peptides (similar to the more diffuse idea of “immune enhancement”). Here I provide an assessment of potential for human pathogenesis via autoimmunity via exposure, via infection or injection. SAR-CoV-2 spike proteins, and all other SARS-CoV-2 proteins, immunogenic epitopes in each SARS-CoV-2 protein were compared to human proteins in search of high local homologous matching. Only one immunogenic epitope in a SARS-CoV-2 had no homology to human proteins. If all of the parts of the epitopes that are homologous to human proteins are excluded from consideration due to risk of pathogenic priming, the remaining immunogenic parts of the epitopes may be still immunogenic and remain as potentially viable candidates for vaccine development. Mapping of the genes encoding human protein matches to pathways point to targets that could explain the observed presentation of symptoms in COVID-19 disease. It also strongly points to a large number of opportunities for expected disturbances in the immune system itself, targeting elements of MHC Class I and Class II antigen presentation, PD-1 signaling, cross-presentation of soluble exogenous antigens and the ER-Phagosome pathway. Translational consequences of these findings are explored.
“The main difference between TH1 and TH2 immune response is that TH1 immune response is a proinflammatory response, which kills intracellular parasites and perpetuates autoimmune responses, whereas TH2 immune response promotes IgE and eosinophilic responses in atopy and produces anti-inflammatory responses, which kill large, extracellular parasites such as helminths9.”
Among coronaviruses, the spike surface glycoprotein is known to play a role in neuroimmunopathology. However, the SARS-CoV-2 virus has numerous other proteins and polyproteins, each which may serve as an antigen source during infection leading to autoimmunity. the immune system presents those proteins, like all human proteins, as “normal”. T-cells are trained to recognize a normal protein shape in the thymus. Biomimicry between or among proteins from pathogens (infection or injection) can conflate the signaling by creating a population of memory B-cells, especially if the reaction switches from a Th-1 toward a Th-2 response.
In SARS, a type of “priming” of the immune system was observed during animal studies of SARS spike protein-based vaccines leading to increased morbidity and mortality in vaccinated animals who were subsequently exposed to wild SARS virus. The problem, highlighted in two studies, became obvious following post-vaccination challenge with the SARS virus [2]. found that recombinant SARS spike-protein-based vaccines not only failed to provide protection from SARS-CoV infection, but also that the mice experienced increased immunopathology with eosinophilic infiltrates in their lungs. Similarly [3], found that ferrets previously vaccinated against SARS-CoV also developed a strong inflammatory response in liver tissue (hepatitis). Both studies suspected a “cellular immune response”.
These types of unfortunate outcomes are sometimes referred to as “immune enhancement”; however, this nearly euphemistic phrase fails to convey the increased risk of illness and death due to prior exposure to the SARS spike protein. For this reason, I refer to the concept as “pathogen priming”; the peptides with pathogenic potential therefore are referred to as “putative pathogenic priming peptides”.
In this study, I present the likely human epitopic targets of biomimicry-induced autoimmunological components of morbidity and mortality caused by SARS-CoV-2 infection. This is achieved via bioinformatics analysis of the homology between highly immunogenic SARS-CoV-2 epitopes and human proteins to promote comprehension of the etiologies of pathogenesis of SARS-CoV-2 in COVID-19. Thirty-seven identified proteins in SARS-CoV-2 were evaluated.
Extract of S and spike protein epitopes from Table 1 and their roles from the genecards database, as applicable:
“Predicted to enable carbohydrate binding activity. Predicted to be involved in several processes, including animal organ morphogenesis; cell migration; and substrate adhesion-dependent cell spreading. Predicted to act upstream of or within G protein-coupled receptor signaling pathway. Predicted to be located in membrane. Predicted to be integral component of membrane. Predicted to be active in basement membrane.”
“May play a role in melanocortin signaling pathways that regulate energy homeostasis.”
“This gene encodes a protein with similarity to follistatin, an activin-binding protein. It contains an FS module, a follistatin-like sequence containing 10 conserved cysteine residues. This gene product is thought to be an autoantigen associated with rheumatoid arthritis.”
“FSTL1 (Follistatin Like 1) is a Protein Coding gene. Diseases associated with FSTL1 include Rheumatoid Arthritis and Arthritis. Among its related pathways are Signaling by BMP and Metabolism of proteins. Gene Ontology (GO) annotations related to this gene include calcium ion binding and heparin binding. An important paralog of this gene is FSTL5.”
“Secreted glycoprotein that is involved in various physiological processes, such as angiogenesis, regulation of the immune response, cell proliferation and differentiation (PubMed:29212066, PubMed:22265692). Plays a role in the development of the central nervous system, skeletal system, lungs, and ureter (By similarity). Promotes endothelial cell survival, migration and differentiation into network structures in an AKT-dependent manner. Also promotes survival of cardiac myocytes (By similarity). Initiates various signaling cascades by activating different receptors on the cell surface such as DIP2A, TLR4 or BMP receptors.”
“FSTL1 has a role in development, such as lung development, ureter development, central nervous system development, and skeletal development.”
“This gene product is thought to be an autoantigen associated with rheumatoid arthritis.”
“FSTL1 up-regulates proinflammatory mediators important in the pathology of arthritis, and serum levels of FSTL1 correlate with severity of arthritis.”
“FSTL1 protein seems to have a cardioprotective role. FSTL1 attenuated hypertrophy following pressure overload and prevented myocardial ischemia/reperfusion injury in a mouse or pig model of ischemia/reperfusion. Muscle-derived Fstl1 modulates vascular remodelling in response to injury.”
“FSTL1 has been shown to have a pronounced ability as a possible therapeutic to stimulate regeneration following myocardial infarction. Treating experimental animals (mouse and pig) with FSTL1 after myocardial infarction progressively restored heart function, at least in part by stimulating replication of normally non-dividing heart muscle cells.13”
“Predicted to enable zinc ion binding activity. Involved in cellular response to cadmium ion and cellular response to zinc ion. Located in cytoplasm and nucleus.”
“MT1E (Metallothionein 1E) is a Protein Coding gene. Diseases associated with MT1E include Frontometaphyseal Dysplasia 2 (“A form of frontometaphyseal dysplasia, a progressive sclerosing skeletal dysplasia affecting the long bones and skull. Characteristic features include supraorbital hyperostosis, cranial hyperostosis, undermodeling of the small bones, flared metaphyses, and digital anomalies. Extra-skeletal manifestations include hearing loss, cardiac malformations, and stenosis, particularly of the upper airway and urinary tract. FMD2 inheritance is autosomal dominant.”). Among its related pathways are Metal ion SLC transporters and Copper homeostasis. An important paralog of this gene is MT2A.”
“Metallothioneins have a high content of cysteine residues that bind various heavy metals; these proteins are transcriptionally regulated by both heavy metals and glucocorticoids.”
“The biosynthesis of metallothionein appeared to have increased by several-fold throughout oxidative stress to shield the cells against cytotoxicity and DNA damage. Metallothionein biosynthesis can also be induced by certain agents or conditions, for example, hormones, pharmaceuticals, alcohols, other substance treatments and many more. Metallothionein is a cytoplasmic protein, in an adult liver, it is localized mainly in the cytoplasm. In human fetus, metallothionein is localized in hepatocyte nuclei.15”
“This protein is a member of the keratin-associated protein (KAP) family. The KAP proteins form a matrix of keratin intermediate filaments which contribute to the structure of hair fibers. KAP family members appear to have unique, family-specific amino- and carboxyl-terminal regions and are subdivided into three multi-gene families according to amino acid composition: the high sulfur, the ultrahigh sulfur, and the high tyrosine/glycine KAPs. This protein is a member of the ultrahigh sulfur KAP family and the gene is localized to a cluster of KAPs at 17q12-q21.”
“KRTAP4-7 (Keratin Associated Protein 4-7) is a Protein Coding gene. Diseases associated with KRTAP4-7 include Alcohol-Related Neurodevelopmental Disorder (“A fetal alcohol spectrum disorder that results in central nervous system dysfunction and behavioral and/or cognitive deficits due to prenatal alcohol exposure”). An important paralog of this gene is KRTAP4-9.”
“In the hair cortex, hair keratin intermediate filaments are embedded in an interfilamentous matrix, consisting of hair keratin-associated proteins (KRTAP), which are essential for the formation of a rigid and resistant hair shaft through their extensive disulfide bond cross-linking with abundant cysteine residues of hair keratins. The matrix proteins include the high-sulfur and high-glycine-tyrosine keratins.”
One can speculate that congenital defects referred to above may be a consequence of autoimmune inhibition of these proteins in the developing foetus and thereafter:
“For women who have an autoimmune disease and subsequently become pregnant, pregnancy can induce amelioration of the mother’s disease, such as in rheumatoid arthritis, while exacerbating or having no effect on other autoimmune diseases like systemic lupus erythematosus. That pregnancy also leaves a long-term legacy has recently become apparent by the discovery that bi-directional cell trafficking results in persistence of fetal cells in the mother and of maternal cells in her offspring for decades after birth. The long-term persistence of a small number of cells (or DNA) from a genetically disparate individual is referred to as microchimerism. While microchimerism is common in healthy individuals and is likely to have health benefits, microchimerism has been implicated in some autoimmune diseases such as systemic sclerosis.”
“Autoimmune responses in the mother may also target the fetus when autoantibodies cross the placenta, such as neonatal lupus syndrome (NLS) and neonatal thyrotoxicosis. The heterogeneity of immune defects across autoimmune diseases is reflected in the varying response of each disease in the context of pregnancy.17”
There was a declaration of competing interest:
Dr. Lyons-Weiler has, in the past, served as expert witness in the National Vaccine Injury Compensation Program.
Further research into epitope homology
Subsequent papers served to confirm Dr Lyons-Weiler’s findings on epitope homology and pathological implications.
This study by Kanduc & Shoenfeld, also in 2020, used hexa- and heptapeptides as sequence probes to find the peptide overlaps between SARS-CoV-2 spike glycoprotein and mammalian proteomes18:
The expected value for hexapeptide sharing between two proteins was calculated by considering the number of all possible hexapeptides. Since in a hexapeptide, each residue can be any of the 20 amino acid (aa), the number of all possible hexapeptides N is given by N = 206 = 64 × 106. Then, the number of the expected occurrences is directly proportional to the number of hexapeptides in the two proteins and inversely proportional to N. Assuming that the number of hexapeptides in the two proteins is << N and neglecting the relative abundance of aa, we obtain a formula derived by approximation, where the expected number of hexapeptides is 1/N or 20−6. By applying the same calculation, the expected value for heptapeptide sharing between two proteins is equal to 20−7.
Peptide sharing between SARS-CoV-2 spike glycoprotein and mammalian and coronavirus proteomes. a Peptide sharing at the 6-mer level. b Peptide sharing at the 7-mer level
A massive heptapeptide sharing exists between SARS-CoV-2 spike glycoprotein and human proteins.Such a peptide commonality is unexpected and highly improbable from a mathematical point of view, given that, as detailed under the “Methods” section, the probability of the occurrence in two proteins of just one heptapeptide is equal to ~ 20−7 (or 1 out of 1,280,000,000). Likewise, the probability of the occurrence in two proteins of just one hexapeptide is close to zero by being equal to ~ 20−6 (or 1 out of 64,000,000).
Only the viral peptide sharing with the murine proteome and, at a lesser extent, with the rat proteome keeps up with that shown by human proteins;
Domestic animals, rabbit, and the three primates analyzed here have no or only a few peptide commonalities;
Likewise, the proteomes of the three human coronaviruses HKU1, 229E, and OC43, which were used as viral controls, have no or only a few peptides in common with the spike glycoprotein. In this regard, it seems that the SARS-CoV-2 spike glycoprotein is phenetically more similar to humans and mice than to its coronavirus “cousins”.
Gain of function work has to be implicated here.
They conclude that only aged mice appeared to be a correct animal model for testing a vaccine, and also recommended that minimal immune determinants unique to the virus and absent in the human proteome be used on the grounds of safety and efficacy. Their warnings were, again, not taken into consideration:
Conclusions
This study thoroughly quantifies the hexa- and heptapeptide sharing of SARS-CoV-2 spike glycoprotein—which is a major antigen of the virus—with mammalian proteomes. A massive peptide commonality is present with humans and mice, i.e., organisms that undergo pathologic consequences following SARS-CoV-2 infection. Instead, no or a lowest number of common peptides are present in mammals that have no major pathologic sequelae once infected by SARS-CoV-2 [10,11,12]. Hence, the data appear to be an indisputable proof in favor of molecular mimicry as a potential mechanism that can contribute to or cause the SARS-CoV-2 associated diseases.
In conclusion, in light of the data exposed in Fig. 1 and given the susceptibility parameters such as aging and health status, only aged mice appear to be a correct animal model for testing an anti-SARS-CoV-2 spike glycoprotein vaccine to be used in humans [25, 26].
Finally, this study once more reiterates the concept that only vaccines based on minimal immune determinants unique to pathogens and absent in the human proteome might offer the possibility of safe and efficacious vaccines.
Screening for autoantibodies in healthcare workers
Wang et al, in this paper from 2020, screened COVID-19 infected patients and healthcare workers for autoantibodies. These were associated with impaired antiviral responses and exacerbated disease severity in a mouse model19:
Abstract
COVID-19 manifests with a wide spectrum of clinical phenotypes that are characterized by exaggerated and misdirected host immune responses1–8. While pathological innate immune activation is well documented in severe disease1, the impact of autoantibodies on disease progression is less defined. Here, we used a high-throughput autoantibody discovery technique called Rapid Extracellular Antigen Profiling (REAP) to screen a cohort of 194 SARS-CoV-2 infected COVID-19 patients and healthcare workers for autoantibodies against 2,770 extracellular and secreted proteins (the “exoproteome”). We found that COVID-19 patients exhibit dramatic increases in autoantibody reactivities compared to uninfected controls, with a high prevalence of autoantibodies against immunomodulatory proteins including cytokines, chemokines, complement components, and cell surface proteins. We established that these autoantibodies perturb immune function and impair virological control by inhibiting immunoreceptor signaling and by altering peripheral immune cell composition, and found that murine surrogates of these autoantibodies exacerbate disease severity in a mouse model of SARS-CoV-2 infection. Analysis of autoantibodies against tissue-associated antigens revealed associations with specific clinical characteristics and disease severity. In summary, these findings implicate a pathological role for exoproteome-directed autoantibodies in COVID-19 with diverse impacts on immune functionality and associations with clinical outcomes.
BLAST analysis for whole virus epitopic homology and related pathology
This 2021 paper by Vojdani et al used BLAST analysis to look for whole virus epitopic homology20. The most striking comment is the typical timescales involved until autoimmune disorders become symptomatic, which would place us in the mid 2020’s before cases could even start to peak in a long bell curve, and of course a peak in cases can only occur provided there is a cessation of all exposure to the homologous epitopes:
The third important question to consider is whether cross-reactivity between COVID-19 and human tissue can lead to autoimmune disease development either from the infection or directly from vaccination. Determining this can be an enormous task because the development of most autoimmune diseases may take 3 to 18 years (7). Segal and Shoenfeld have raised concerns for vaccine-induced autoimmunity by citing examples of how previous vaccinations have induced cross-reactive autoimmunity in susceptible subgroups. They cite specific examples of how vaccine-induced cross-reactivity has led to the onset of systemic lupus erythematous, demyelinating autoimmune diseases, narcolepsy, and postural orthostatic tachycardia syndrome (8). In a very interesting letter, Kanduc and Shoenfeld addressed the issue of peptide sharing between SARS-CoV-2 spike glycoprotein and lung-surfactant-related proteins (9). They suggested that because the SARS-CoV-2 and lung surfactant proteins shared 13 out of 24 pentapeptides, the immune response following infection with SARS-CoV-2 may lead to cross-reactions with pulmonary surfactant proteins, followed by SARS-CoV-2–associated lung disease (9). Furthermore, very recently they presented indisputable proof of molecular mimicry as a potential mechanism for contributing to SARS-CoV-2 associated diseases (10). Based on their findings, they warned against the use of the entire SARS-CoV-2 antigens in the vaccines and cautioned that perhaps the use of only unique peptides would be the most effective way to fight the SARS-CoV-2 infection. Due to the significant red flags for the potential cross-reactivity between SARS-CoV-2 and human tissue, we have undertaken to study the interaction of antibodies made against SARS-CoV-2 spike protein, nucleoprotein, envelope protein and membrane protein with various autoimmune target proteins associated with many serious diseases. This way, we can establish the potential risk for autoimmunity and multi-system disorders with COVID-19 that may come from cross-reactivity between our own human tissues and this dreaded virus, and thus ensure that the badly-needed vaccines and treatments being developed for it are truly safe to use against this pandemic.
Results
In this study, we measured the degree of immune reactivity of human monoclonal antibody made against SARS-CoV-2 spike protein and nucleoprotein and rabbit polyclonal antibody made against SARS-CoV-2 envelope and membrane proteins with 55 different tissue proteins and peptides. Using ELISA methodology, we first found that human serum from a healthy subject and unimmunized rabbit serum did not react with spike protein, nucleoprotein, envelope protein, membrane protein, or with the 55 different tissue proteins and peptides. The ELISA ODs for all these reactions were within 3 SD above the mean of the control values, or OD < 0.25.
As was expected, the strongest reactions were between anti-SARS-Cov-2 spike protein antibody and SARS-CoV-2 spike protein (OD 3.40 or very strong), anti-SARS-Cov-2 nucleoprotein antibody and SARS-CoV-2 nucleoprotein (OD 3.76 or very strong), anti-SARS-Cov-2 envelope protein antibody and SARS-CoV-2 envelope protein (OD 3.68 or very strong), and anti-SARS-Cov-2 membrane protein antibody and SARS-CoV-2 membrane protein (OD 3.78 or very strong), which is close to the maximum detection limit of the assay (OD 4.0). These SARS-CoV-2 antibodies reacted from low to very high with 28 out of 55 tissue antigens. These 28 antigens were a diverse collection of tissue groups that included gut and barrier proteins, gastrointestinal system cells, thyroid, nervous system, heart, joint, skin, muscle, mitochondria and liver tissues, and antigens used for the screening of autoimmune diseases. The mean OD of the anti-SARS-Cov-2 spike protein antibody’s reactivity with the non-reactive 27 tissue antigens +3SD was 0.34.
Using this 0.34 OD as a cutoff, we found that human anti-SARS-Cov-2 spike protein antibody reacted strongest with neurofilament protein or NFP (OD 1.98), followed by strong reactions with M2 (OD 1.52), GAD-65 (OD 1.35), and nuclear antigen or NA (OD 1.34). The reaction of this spike protein antibody with TPO and liver microsome was moderate(ODs 0.98, 1.0). With another 19 antigens the spike antibody’s reaction was weak with ODs ranging from 0.41 to 0.85 (see Figure 1).
Antimitochondrial M2 antibodies:
“These substances are usually made by your body if you have a condition called primary biliary cirrhosis (PBC). PBC is the most common autoimmune disease that affects the liver. In autoimmune diseases, the immune system attacks organs or tissues in the body. Antimitochondrial antibody is found in nearly 19 in 20 people with PBC.
PBC causes damage to ducts in the liver that drain away fluid called bile. As a result bile builds up in the liver. This scars the liver. This scarring keeps the liver from working as it should. Over time, it causes liver failure.
PBC is especially common in middle-aged women. It often strikes along with other autoimmune diseases, especially Sjögren syndrome.
PBC is usually diagnosed and treated early in the course of the disease. This is good, because early treatment can slow down liver scarring. It delays liver failure.
What does it mean if your Mitochondrial (M2) Antibody result is too high?
Antimitochondrial antibodies (AMA) have been reported in 90% to 96% of patients with primary biliary cirrhosis. AMA are also occasionally found in sera of patients with other liver diseases, including chronic active hepatitis, cryptogenic cirrhosis, as well as in patients with clinical but no biochemical evidence of liver disease. The M2 antigen used is strongly associated with PBC, while other types (M1, M2, M5, and M6) are associated with a wide variety of conditions.21”
Autoantibodies to neurofilament proteins:
“Immune responses to neuronal proteins are a frequent occurrence in neurodegenerative diseases. This study determines the occurrence of autoantibodies to the three neurofilament subunits in phosphorylated and dephosphorylated forms and relates these measures to age, human leukocyte antigen (HLA), and severity of disease in Down syndrome (DS).22”
“We identified neurofilament protein and the prevalence of anti-bovine neurofilament light subunit (NF-L) autoantibodies in glaucomatous patients was significantly higher than in healthy controls and patients with other uveitic and optic nerve diseases (P<0.05). In addition, our immunogenetic analysis showed a possible association between HLA-DRB1*1502 allele and the patients positive for anti-NF-L autoantibodies. It suggests that the HLA class II-linked gene may be involved in development of autoimmunity in patients with glaucoma.23”
GAD65 neurological autoimmunity:
“The glutamic acid decarboxylase 65-kilodalton isoform (GAD65) antibody is a biomarker of autoimmune central nervous system (CNS) disorders and, more commonly, nonneurological autoimmune diseases. Type 1 diabetes, autoimmune thyroid disease, and pernicious anemia are the most frequent GAD65 autoimmune associations. One or more of these disorders coexists in approximately 70% of patients with GAD65 neurological autoimmunity. Neurological phenotypes have CNS localization and include limbic encephalitis, epilepsy, cerebellar ataxia, and stiff-person syndrome (SPS), among others. Classic SPS is a disorder on the spectrum of CNS hyperexcitability which also includes phenotypes that are either more restricted (stiff-limb syndrome) or more widespread (progressive encephalomyelitis with rigidity and myoclonus). GAD65 antibody is not highly predictive of a paraneoplastic cause for neurological disorders, but diverse cancer types have been occasionally reported. For all phenotypes, responses to immunotherapy are variable (approximately 50% improve). GAD65 autoimmunity is important to recognize for both coexisting nonneurological autoimmune associations and potential immunotherapy-response.24”
Anti-nuclear antibodies:
“Antinuclear antibodies (ANAs, also known as antinuclear factor or ANF)[1] are autoantibodies that bind to contents of the cell nucleus. In normal individuals, the immune system produces antibodies to foreign proteins (antigens) but not to human proteins (autoantigens). In some cases, antibodies to human antigens are produced.[2]
There are many subtypes of ANAs such as anti-Ro antibodies, anti-La antibodies, anti-Sm antibodies, anti-nRNP antibodies, anti-Scl-70 antibodies, anti-dsDNA antibodies, anti-histone antibodies, antibodies to nuclear pore complexes, anti-centromere antibodies and anti-sp100 antibodies. Each of these antibody subtypes binds to different proteins or protein complexes within the nucleus. They are found in many disorders including autoimmunity, cancer and infection, with different prevalences of antibodies depending on the condition. This allows the use of ANAs in the diagnosis of some autoimmune disorders, including systemic lupus erythematosus, Sjögren syndrome,[3] scleroderma,[4] mixed connective tissue disease,[5] polymyositis, dermatomyositis, autoimmune hepatitis[6] and drug induced lupus.25”
TPO autoimmunity:
“Autoimmunity to thyroid peroxidase (TPO), manifest as high affinity IgG class autoantibodies, is the common denominator of human thyroid autoimmunity, encompassing patients with overt hyper- or hypothyroidism as well as euthyroid individuals with subclinical disease.26”
Actin autoimmunity:
Of particular note here is that a pathogenic autoimmune response to actin can lead to food particles entering the blood stream, which in turn leads to further complicating autoimmune conditions and food sensitivities:
“What is actin and why is it important for leaky gut?
Actin is a protein that is utilized in many functions in the body. Actin plays two primary roles in intestinal anatomy.
Actin's first role in the small intestine is in the microvilli, hairlike protrusions that increase surface area in the small intestine. They increase the ability of the small intestine to absorb nutrients across the intestinal lining and into the bloodstream. More surface area means more contact with the chyme and an increased ability to absorb nutrients. In the microvilli, actin is used to make the microfilaments which provide structure to these microscopic microvilli. The extremely fine actin microfilaments provide structure to the hairlike filaments protruding into the lumen of the small intestine, reaching out to absorb nutrients from chyme.
Actin is also involved in many other functions microvilli physiology, in addition to the structure itself. Some of these roles include cell division and locomotion, transporting embryonic cells, allowing white blood cells to leak into tissue to fight infection, and assisting skin cells in wound healing. In many ways, the health of microvilli cells are dependent upon actin.
Actin also helps adhere individual microvilli to each other in order to create an impermeable intestinal membrane. When this membrane becomes permeable, also known as leaky gut, the junctions between microvilli become separated and this compromises the integrity of the gut wall. This allows partially digested food particles to enter the blood stream, which is implicated in multiple types of autoimmune conditions, as well as food sensitivities.
Because actin is so important for the structure and function of the intestinal lining it is not surprising that problems with actin can contribute to intestinal permeability. Actin autoimmunity is thought to be a contributory factor in leaky gut because a breakdown of actin leads to degradation of the intestinal wall, allowing it to become permeable.27”
…the spike protein antibody exhibited significant reactions with 25 out of 55 tested target proteins, with the strongest reactions coming from NFP and M2 antigens. The nucleoprotein antibody reacted with 24 out of 55 tissue antigens, with M2 and insulin-R showing the highest reactivity. The envelope protein antibody had weak to very strong reactions with only 8 different antigens, with the most pronounced from M2 and intestinal epithelial cell antigens. Finally, the membrane protein antibody reacted very strongly with M2 and NFP, but not as strongly with an additional 16 tissue antigens. Interestingly, M2 reacted strongly with both human monoclonal antibodies made against spike protein and nucleoprotein and with both rabbit polyclonal antibodies made against envelope and membrane proteins.
Using BLAST, we did an extensive search for the degree of identity between SARS-CoV-2 proteins and mitochondrial M2 protein (human monoclonal antibody made against spike protein reacted very strongly with M2 protein), F-actin (a major component of smooth muscle, since spike protein human monoclonal antibody had moderate reactions with this antigen).
SARS-CoV-2 proteins shared a significant number of peptide sequences with mitochondrial M2 protein, ranging from 50% to 78% identity, 58% to 63% with F-actin, and 50% to 70% with TPO. We found that some peptide sequences matched with more than one section of SARS-CoV-2; for instance, the actin sequence SIL—ASLSTF cross-reacted with the sequence SVLYNSASFSTF in the SARS-CoV-2 spike protein Chains A, B, C and E, as well as in Chain E of the SARS-CoV-2 spike receptor binding domain.
The authors tested for a wider range of antigens than in the Lyons-Weiler study and consider multisystem inflammatory syndrome (MIS):
While our own list of 55 selected human tissue antigens shares some unavoidable overlap with those used in the Lyons-Weiler study (5), we went further and based our selection on key target human tissue proteins that were known to be involved both with extra-pulmonary manifestations of COVID-19 and common autoimmune diseases. For example, the Lyons-Weiler study examined heart muscle, skeletal muscle and thyroid gland, whereas we studied alpha-myosin, actin and TPO. Lyons-Weiler studied brain, liver, GI tract and skin, whereas we examined SARS-CoV-2 cross-reactivity with brain tissue antigens (MBP, NFP, amyloid-beta, alpha-synuclein, synapsin, tTG-6), liver microsomal peptide, M2 protein, PDH peptide, and skin antigens (tTG-2, tTG-3, epithelial cell antigens). We also examined many other tissue antigens, such as barrier proteins, that were not tested in the Lyons-Weiler study. In an effort to provide further proof for this concept, we sought to determine in this study whether human monoclonal antibody that mimics natural antibodies produced by the immune system to fight the SARS-CoV-2 virus will react to various human tissue antigens. This immune reaction may be responsible for the multi-organ system disorder found in patients with severe COVID-19.
They did indeed find autoimmune reactivity against barrier proteins:
Our study found immune reactivity between SARS-CoV-2 antibodies and barrier target proteins; occludin+zonulin, beta-catenin, and S100B. These proteins are responsible for maintaining the integrity of the barriers. These cross-reactive interactions may lead to permeability of the lung barrier, gut-barrier, and the blood-brain barrier in susceptible individuals (28–31). A recent systematic review and meta-analysis has identified age, smoking, diabetes, cardiovascular disease, and respiratory diseases as significant risk factors associated with increased mortality rate and greater risk for critical illness from COVID-19 (32). Every single one of these identified risk factors is also associated with permeability of the immune barrier systems (33–37). Permeability of the immune barriers may be the essential centerpiece risk factor that is associated with COVID-19 severity, and part of this mechanism may also be associated with the combined impact of cross-reactivity of SARS-CoV-2 with immune barrier proteins. Permeability of these barriers may increase the spread of the virus throughout the body and potentially promote a systemic cytokine storm (38–40). Additionally, permeability of the immune barriers is also an independent mechanism that may promote immune dysregulation and the onset of autoimmune diseases (41). This is of great concern since autoantibodies to phospholipids have been found with COVID-19 and can lead to life-threatening complications of coagulopathy (3).
And autoantibodies against an enzyme that plays a role in celiac disease:
In addition to the reaction of the SARS-CoV-2 antibodies with tight junction proteins, the human monoclonal antibodies made against spike protein and nucleoprotein reacted with transglutaminase-2 (tTG-2), an enzyme in the intestinal mucosa that plays a role in celiac disease. Moreover, rabbit polyclonal antibody made against SARS-CoV-2 envelope protein reacted strongly with intestinal epithelial cell antigens. This cross-reaction between SARS-CoV-2 and gastrointestinal tissue antigens may be responsible for the gastrointestinal manifestations of COVID-19.
Thyroid autoimmunity (TPO):
Our study also identified several cross-reactive interactions that may lead to specific autoimmune patterns. For example, we found that SARS-CoV-2 spike protein, nucleoprotein, and membrane protein all cross-reacted with TPO. Furthermore, we found through BLAST sequence matching that many TPO peptide sequences shared homology or similarity with sequences in various SARS-CoV-2 proteins. These findings suggest that antibodies developed against SARS-CoV-2 may promote autoimmune thyroiditis. A recent case study identified sub-acute thyroiditis after SARS-CoV-2 infection (43). It is possible this may have been the first reported case of thyroid cross-reactivity from COVID-19. While data on thyroid pathophysiology is currently not available for COVID-19, patients with SARS have been found to have destruction of thyroid follicular cells, and there are highly similar genomic sequences between SARS-CoV and SARS-CoV-2 (33, 44).
Against CNS proteins. Note that either onset or increased severity of symptoms for all the highlighted conditions have since been reported as post transfection adverse events:
Several SARS-CoV-2 antibody cross-reactions were identified with central nervous system target proteins that included NFP, MBP, GAD-65, beta-amyloid, alpha-synuclein, synapsin and tTG-6. Compared to the other tissue antigens, NFP had the strongest reaction (very strong) with spike protein, and a very strong reaction with membrane protein that was second only to the reaction of membrane protein with M2 antigens. Antibodies against these neural protein targets are detected in patients with neuroautoimmune disorders such as multiple sclerosis, Alzheimer’s disease (AD), and ataxia (45, 46). A high level of neurofilament light chain proteins, which is a marker of neural injury, was detected in COVID-19 patients (47).
Against smooth and cardiac muscle:
SARS-CoV-2 cross-reactivity was also identified with target proteins to both striated and smooth muscles including actin and alpha-myosin. Actin is a major component of muscle that contributes to the tissue’s contractile property. Alpha-myosin is a heart muscle-specific constrictive protein. We did epitope mapping with BLAST and found many instances of peptide similarity and homology between F-actin and various SARS-CoV-2 proteins at identity percentages of 58% to 63%, with multiple instances and repeats of matches with sequences in different SARS-CoV-2 proteins.
Equally concerning, autoantibodies against mitochondria and a possible contributor to long COVID/long vaccine syndrome. Latent herpes virus reactivation has also been discussed in other studies28, another contributor to mitochondrial dysfunction.
“Twenty-five out of 29 known ME/CFS symptoms were reported by at least one selected long COVID study. Conclusions: Early studies into long COVID symptomatology suggest many overlaps with clinical presentation of ME/CFS.29”
“Mitochondria are the “energy factory” of our body. Mitochondrial diseases are long-term, genetic, often inherited disorders that occur when mitochondria fail to produce enough energy for the body to function properly. One in 5,000 individuals has a genetic mitochondrial disease.”
Due to the similarity between mitochondrial dysfunction and the induction of multi-organ disorder by SARS-CoC-2, we measured the reactivity of four different antibodies made against SARS-CoV-2 proteins with M2, which is part of the pyruvate dehydrogenase complex. Antibody against this mitochondrial antigen is detected in 90% to 95% of patients with primary biliary cirrhosis (PBC), and occasionally in other liver diseases and scleroderma (55). In fact, mitochondrial M2 was the only antigen out of 28 cross-reactive antigens in our study that had strong to very strong reactions with all four SARS-CoV-2 protein antibodies (Table 1). Furthermore, we found that sera negative for M2 antibody had no reactivity with the SARS-CoV-2 proteins, while sera positive for M2 antibody had moderate reactions (Table 6). These results further support mimicry between SARS-CoV-2 and M2 proteins resulting in the production of cross-reactive antibodies. Interestingly, we also tested the human monoclonal antibodies made against the viral spike and nucleoprotein with liver microsomal antigens as well as pyruvate dehydrogenase peptide E2 (PDC-E2) subunit; the modification of this subunit by xenobiotics is held to be responsible for the induction of PBC. While we do not know how mitochondrial antibodies contribute to the etiopathology of disease induced by SARS-CoV-2, cross-reaction by SARS-CoV-2 protein antibodies with M2, PDC-E2 and liver microsomal antigens gives further support to a possible role for SARS-CoV-2 in liver autoimmunity. Our own findings strengthen the recent findings by Wang et al (56). that SARS-CoV-2 infection of the liver is an important factor in hepatic impairment in patients with COVID-19. We also did epitope mapping by BLAST for mitochondria M2 against SARS-CoV-2 proteins, and found that mitochondria M2 sequences had even greater similarity and homology with SARS-CoV-2 proteins than actin, especially for spike protein, again with multiple repeats in the same peptide chains as well as sequence matches in different kinds of SARS-CoV-2 proteins.
Recently, Holder and Reddy (57) showed how interaction between SARS-CoV-2 and immune cells alters mitochondrial activities in host cells, providing a receptive intracellular environment for viral replication in infected cells that may contribute to the progression of the disease in COVID-19 patients (57). Additionally, Schreiner et al. showed that in patients with myalgic encephalomyelitis/chronic fatigue syndrome, mitochondria were strongly fragmented by human herpesvirus 6 (HHV-6) and HHV-7; this is believed to be the trigger of the disease (58). Whether such fragmentation of mitochondria that results in the production of mitochondrial antibody occurs with SARS-CoV-2 certainly deserves future investigation.
“Polymyositis and dermatomyositis. These are two related diseases in which there is inflammation of the muscles (polymyositis) and skin (dermatomyositis). Symptoms of both diseases can include:
People with dermatomyositis may also have a skin involvement around the eyes and the hands.
Rheumatoid arthritis (RA). Rheumatoid arthritis is a disease in which the immune system attacks the thin membrane (called the synovium) lining the joints, causing pain, stiffness, warmth and swelling of the joints, and inflammation throughout the body. Other symptoms may include:
RA can lead to permanent joint damage and deformity.
Scleroderma. Scleroderma is a term for a group of disorders that causes thick, tight skin, buildup of scar tissue, and organ damage. These disorders fall into two general categories: localized scleroderma and systemic sclerosis.
Localized scleroderma is confined to the skin and, sometimes, the muscle beneath it. Systemic sclerosis also involves the blood vessels and major organs.
Sjögren's syndrome. Sjögren's syndrome is a chronic disease in which the immune system attacks the moisture-producing glands, such as those of the eyes and mouth. The effects can range from mildly uncomfortable to debilitating. Although dry eyes and mouth are the main symptoms of Sjögren's, many people also experience extreme fatigue and joint pain. The condition also increases the risk of lymphoma and may cause problems with the kidneys, lungs, blood vessels, and digestive system as well as nerve problems.
Systemic lupus erythematosus. Systemic lupus erythematosus (SLE or simply lupus) is a disease characterized by inflammation of the joints, skin, and internal organs. Symptoms may include:
A butterfly-shaped rash on the cheeks and bridge of the nose
Problems with memory and concentration or other nervous system disorders
Vasculitis. Vasculitis is a general term for more than 20 different conditions characterized by inflammation of the blood vessels. These can affect blood flow to the organs and other body tissues. Vasculitis can involve any of the blood vessels.
Mixed connective tissue disease. People with MCTD have some features characteristic of several diseases, including lupus, scleroderma, polymyositis or dermatomyositis, and rheumatoid arthritis. When this occurs, doctors often make the diagnosis of mixed connective tissue disease.
While many people with mixed connective tissue disease have mild symptoms, others may experience life-threatening complications.31”
Lastly, we identified cross-reactivity with autoimmune target proteins involved in mixed connective tissue diseases (MCTD) that included nuclear antigen (NA), extractable nuclear antigen (ENA), histone and collagen. SARS-CoV-2 spike protein antibody reacted with ENA, NA and histone, nucleoprotein antibody reacted with NA, histone and collagen, and membrane protein antibody reacted with histone and collagen.
The authors emphasize the limited scope of their studies and recommended further research:
As Lyons-Weiler said, any of these sequence or epitope matches could potentially lead to autoimmunity by cross-reacting with SARS-CoV-2 antibodies (5). The plethora of these matches between SARS-CoV-2 sequences and human tissues may explain why monoclonal antibodies made against SARS-CoV-2 proteins reacted with so many tissue antigens out of the 55 in our study. It should be noted that our study was limited to the identification of general cross-reactive antibody responses, and our BLAST search was just limited to three human tissues.
Other antigens among our list that had moderate reactions or greater with SARS-CoV-2 may also have sequences here and there in their structure that could potentially be triggers of autoimmunity, and likewise deserve additional attention and study. Further investigation to identify the specific cross-reactive epitopes will require specific peptide fragment inhibition studies as well as computational modeling. More precise identification of conformational autoepitopes is needed to clarify the role of SARS-CoV-2 in autoimmunity.
To conclude their paper they also considered vaccine safety, with a stark warning:
Another concern from molecular mimicry is the potential role it may play in vaccine safety. Several incidences of viral infection and vaccine-induced autoimmunity specific to cross-reactivity have been reported in the literature (8). In 2009, the vaccines developed to treat the H1N1 pandemic lead to narcolepsy specifically due to cross-reactivity. The inactivated split-viron particles (ASO3) shared cross-reactive homology with hypocrites found in the hypothalamus, leading to selective destruction of that substance after vaccination in a subgroup of susceptible individuals (13). Vaccination with ASO3 lead to a three-fold increase in the onset of narcolepsy compared to individuals who were not vaccinated (61).
During the swine flu outbreak in the late 1970s in the United States, the use of influenza vaccination was found to induce a four- to eight-fold increased risk of developing Guillain-Barré syndrome due to cross-reactivity (14). Cross-reactive relationships between viral infections and vaccinations have also been found with hepatitis B and myelin proteins leading to multiple sclerosis, human papillomavirus and nuclear proteins leading to systemic lupus erythematosus (SLE), coxsackievirus and islet cells proteins leading to type 1 diabetes, etc (15–18). Razim et al (62)., in designing a vaccine against Clostridium difficile, concluded that before considering a protein as a vaccine antigen, special care should be taken to analyze and remove the sequences of tissue cross-reactive epitopes in order to avoid possible future side effects.
In a very recent publication in JAMA, Trogen et al. said, “What cannot and must not be allowed is for desperation to result in the suspension of scientific principles and ethical research values (63).” We ourselves would apply these principles and ethical values towards investigating whether SARS-CoV-2 peptides contained in a future vaccine may cross-react with human tissue antigens and possibly result in autoimmunity. But while the possibility of future autoimmune disease is daunting and very real, it must be remembered that without vaccinations the SARS-CoV-2 pandemic will spread unchecked, bringing with it a slew of multiple system disorders including autoimmunities both in the present and the future. We hope that the recently approved human monoclonal antibodies and vaccines can prevent the many extra-pulmonary manifestations and other disorders brought about by COVID-19, and eventually help bring an end to this pandemic.
Conflict of Interest
AV is the co-owner, CEO and employee of Immunosciences Lab., Inc. EV is the owner and employee of Regenera Medical, a private medical practice.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Their last concerns have not borne out as feared. In contrast to post vaccinal high levels of spike protein antibodies, natural viral infection instead produces relatively lower levels of different antibodies against the whole virus rather than a component, and generally at a lower viral & antigenic load due to upper respiratory tract IgA mucosal antibodies. There are always exceptions to this and some individuals will experience high viral loads and autoimmune disorders, but these are the minority.
In addition, as viral reinfections generally diminish with severity due to immune adaption (possibly even low or asymptomatic throughout, especially in children) exposure risk is diminished vs repeated vaccinal boosters that can easily reach 4-5 or more strong doses of spike protein antigens, going into general circulation via the lymphatic system after the deltoid muscle and bypassing the URT entirely32.
Risk of autoimmune disorders from the virus is generally a one off, but risk from vaccination is recurring and possibly cumulative. There is no correlation between antibody counts and immunity to a particular infection, particularly as these can be non-neutralising due to antigenic drift before the product has even come to market.
More is not necessarily better, especially if efficacy is as short as a few weeks and original antigenic sin is induced in the process, along with many many other pathologies. Mucosal antibodies and long term memory B & T-cells aren’t even considered as part of the approval process, let alone the risk of expressing homologous epitopes.
Moderna’s new study tested people who’d had three prior vaccinations, giving 377 of them a fourth dose of the original vaccine and another 437 the combo shot.
The study wasn’t designed to track how well the updated booster prevented COVID-19 cases and it was tested only against omicron, not the variants dominant now. Butthe bivalent vaccine sparked a nearly eight-fold rise in levels of antibodies capable of fighting omicron. Importantly, that was 1.75 times better than the antibody jump from simply giving a fourth dose of the original vaccine, Moderna said.33
Indicative timescales from first testing positive to the onset of symptomatic disease
It is important at this point to expand on typical timescales before autoimmune antibodies may lead to disease, as referred to in the above paper. An excellent paper by Ma et al (2017):
Abstract
The etiology of autoimmune diseases is due to a combination of genetic predisposition and environmental factors that alter the expression of immune regulatory genes through various mechanisms including epigenetics. Both humoral and cellular elements of the adaptive immune system play a role in the pathogenesis of autoimmune diseases and the presence of autoantibodies have been detected in most but not all autoimmune diseases before the appearance of clinical symptoms. In some cases, the presence or levels of these autoantibodies portends not only the risk of developing a corresponding autoimmune disease, but occasionally the severity as well. This observation is intriguing because it suggests that we can, to some degree, predict who may or may not develop autoimmune diseases. However, the role of autoantibodies in the pathogenesis of autoimmune diseases, whether they actually affect disease progression or are merely an epiphenomenon is still not completely clear in many autoimmune diseases. Because of these gaps in our knowledge, the ability to accurately predict a future autoimmune disease can only be considered a relative risk factor. Importantly, it raises the critical question of defining other events that may drive a patient from a preclinical to a clinical phase of disease.
The whole paper is worth a read, but rheumatoid arthritis (RA) is representative of the possible timescales involved, but most conditions present symptoms within a few years and as briefly as 1 year in the case of MS & lupus (SLE). Genetic makeup and epigenetics (“environment”) are also key factors in susceptibility:
The presence of autoantibodies is a hallmark of many autoimmune diseases, including systemic lupus erythematosus, rheumatoid arthritis, primary biliary cirrhosis, multiple sclerosis, autoimmune hepatitis, drug-induced lupus, autoimmune thyroid disease and type 1 diabetes. Clearly genetics and the environment play significant roles in loss of tolerance [1], [2], [3], [4], [5], [6], [7], [8], [9]. In this review, we will present the evidence for preclinical disease in several autoimmune diseases and we will speculate on mechanisms that drive the patient from a preclinical to a clinical phase. Because there has not been any reports concerning the appearance of autoantibodies before clinical symptoms of myasthenia gravis and antiphospholipid syndrome, and genetic factors accounting for these two autoimmune diseases are obscure, these two diseases are not discussed in the present article. The appearance of autoantibodies in specific autoimmune diseases before disease onset is presented below and is summarized in Table 1.
In 2003, Rantapää and coworkers found that once people became seropositive for ACPAs, almost all of them retained this positivity, and the antibody titers increased significantly over time before the first clinical manifestation of RA [46]. Moreover, they found that titers of RF isotypes also increased significantly over time.Jan and coworkers measured serum antibody titers in serially obtained samples, and were able to detect ACPAs up to 14 years before symptom appearance[54]. ACPAs of both IgG and IgA isotypes demonstrate seropositivity several years before RA onset, with the strongest predictive value for IgG ACPAs [55]. When Aase et al. conducted a large scale investigation based on cohorts reflective of the general population, they also found that ACPA testing had high specificity for prevalent RA and offered improved diagnostic reliability [56]. In addition to ACPAs, the presence of anti-CarP antibodies can also predict the development of RA, with a median risk time of 12 months.
Fine tuning the analysis: homologous sequences and protein folding
Beaudoin et al (2021) improved the analysis techniques a step further by taking into account not just any homologous sequences but protein folding too, a structural comparison34. The receptor-binding domain (RBD) of the spike protein is critical for RBD-ACE2 receptor interaction.
Highlights
•Potential coronavirus spike protein mimicry revealed by structural comparison.
•Human and non-human protein potential interactions with virus identified.
•Predicted structural mimicry corroborated by protein–protein docking.
•Epitope-based alignments may help guide vaccine efforts.
Abstract
Viruses often encode proteins that mimic host proteins in order to facilitate infection. Little work has been done to understand the potential mimicry of the SARS-CoV-2, SARS-CoV, and MERS-CoV spike proteins, particularly the receptor-binding motifs, which could be important in determining tropism and druggability of the virus. Peptide and epitope motifs have been detected on coronavirus spike proteins using sequence homology approaches; however, comparing the three-dimensional shape of the protein has been shown as more informative in predicting mimicry than sequence-based comparisons. Here, we use structural bioinformatics software to characterize potential mimicry of the three coronavirus spike protein receptor-binding motifs. We utilize sequence-independent alignment tools to compare structurally known protein models with the receptor-binding motifs and verify potential mimicked interactions with protein docking simulations. Both human and non-human proteins were returned for all three receptor-binding motifs. For example, all three were similar to several proteins containing EGF-like domains: some of which are endogenous to humans, such as thrombomodulin, and others exogenous, such as Plasmodium falciparum MSP-1. Similarity to human proteins may reveal which pathways the spike protein is co-opting, while analogous non-human proteins may indicate shared host interaction partners and overlapping antibody cross-reactivity. These findings can help guide experimental efforts to further understand potential interactions between human and coronavirus proteins.
Their conclusions are very interesting. Note that later modelling of 4 HIV inserts on the spike glycoprotein trimer has them outward facing in reactive locations (ie binding energy)35. Of interest here was their finding of the sequences.
Structural mimicry of chemokine and cytokine signaling has been reported for several viruses [1]. Viral proteins can mimic the chemokine, as in the case of HIV gp120 and CCL5, or they can mimic the receptor and bind directly to the cytokine (inhibiting its function), such as the vaccinia virus B15R protein that mimics the IL-1B receptor and binds to IL-1B [62], [63].
The coronavirus RBMs were found to structurally mimic several motifs on the HIV and Influenza spike proteins; however, they were found either facing inwards or buried inside the mimicked protein and were, therefore, discarded. PDBeFold and TM-align indicated that the SARS-CoV-2 and SARS-CoV RBMs structurally mimic several hepatitis C virus (HCV) antibody epitopes. The SARS-CoV-2 and SARS-CoV RBMs were found to be similar to 10 and 6 PDB HCV E2 protein epitopes structures, respectively (Supplementary Table 2). The HCV E2 protein is implicated in host entry, which has been explored as an inhibitory target with neutralizing antibodies.
They concluded that structure and folding wasn’t as critical as hypothesised:
The flexibility of the cystinedisulfide loop in the SARS-related RBMs was found to permit large global changes in RBM structure; however, since most of the predicted mimicry was mapped to the RBM central beta-strands, which are quite rigid, the models of different conformations did not return significantly different proteins from the structural alignment tools.
“Thrombomodulin (TM), CD141 or BDCA-3 isan integral membrane protein expressed on the surface of endothelial cells and serves as a cofactor for thrombin. It reduces blood coagulation by converting thrombin to an anticoagulant enzyme from a procoagulant enzyme.37”
The predicted endogenous mimicry comprised of proteins in cell signaling, adhesion, and complement pathways. Potential mimicry of several microbial antigenic proteins and exogenous toxins was also discovered. The EGF-like domains of both endogenous and exogenous proteins structurally resemble all three RBMs. Predicted mimicked endogenous interactions include the EGF-like domain of thrombomodulin binding to thrombin, NOTCH1 binding to DLL4, and coagulation factor VIIa binding to tissue factor. Interference in these pathways may partially explain coagulopathies in coronavirus infections[126]. Exogenous EGF-like domains of MSP1 from different Plasmodium species, on the other hand, may provide a structural epitope scaffold for cross-reactivity between coronavirus and Plasmodium infections [106]. Epitope similarity was further explored among the several antibody-bound hepatitis C virus E2 protein motifs that were structurally analogous to the SARS-related RBMs. Structural similarity to antigenic proteins from other microbes may confer cross-immunity and, thus, also potentially guide vaccine design [127]. Cell signaling pathway proteins, such as TNF-related and ephrin ligands, were also found as potential mimics of the coronavirus RBMs, which may lead to use of alternative co-receptors for viral entry or modulation of signaling cascades. Complement factor H was returned for all three RBMs and has also been implicated in coronavirus infections [90]. The mimicry of complement proteins is widespread among viruses, and the spike RBM may have secondary roles interfering in these pathways [128]. Many snake and spider toxins were also found similar to the coronavirus RBMs, which implies the potential usage of receptors involved in pain, muscle contraction, cell adhesion, and coagulation pathways[129], [130], [131]. The prediction of evolutionarily unrelated, yet structurally similar, potential protein mimics reveals that previously unidentified pathways could be altered by the spike RBMs. The structural variation between coronavirus RBMs and their resulting molecular mimics can possibly be connected to differences in tropism, infection severity, and immune system reactivity between coronaviruses.
No declarations of competing interest were declared.
The importance of also analysing sequence similarity and localisation
In this 2021 paper by Moody et al they also took a different approach38:
Assessment of potential for cross-reactivity between SARS-CoV-2 and self-proteins with capacity to perpetuate autoimmune pathology was based on a combination of immunologically relevant sequence similarity (not just identity) (Angileri et al., 2020a; Kanduc, 2020; Lucchese and Flöel, 2020; Marino Gammazza et al., 2020) and the localization of the protein itself, with a focus on extracellular targets. 11 human proteins, containing amino acid sequences similar to nine predicted SARS-CoV-2 B cell epitopes, were identified based on these selection criteria. These findings indicate that antibodies induced by SARS-CoV-2 could directly interfere with cell function, including that of immune cells, and could help explain some of the additional pathologies identified in COVID-19 patients (Cheng et al., 2020; Cheung et al., 2020; Han et al., 2020; Hundt et al., 2020; Nalleballe et al., 2020; Oxley et al., 2020; Poyiadji et al., 2020; Xie et al., 2020; Zheng et al., 2020). Finally, comparing the sequences of both predicted spike epitopes and full length spike protein to various human proteins implicated in immune thrombocytopenia purpura (ITP) and thrombocytopenia syndrome (TTS), our results indicate that molecular mimicry is unlikely to be the cause of TTS, or vaccine induced prothrombotic immune thrombocytopenia (VIPIT) following vaccination with the COVID-19 adenovirus vector vaccines. To our knowledge, this is the first study to compare immune epitopes across the circulating VOCs and VOIs; highlight multiple similarities between the selected Orf proteins and human proteins; identify proteins with reported associations to autoimmunity as sharing sequences with SARS-CoV-2 epitopes; and to highlight novel extracellular human proteins which may have antibody cross-reactivity with SARS-CoV-2 immunogenic regions.
Additionally, 144 of the self-proteins are reported to be associated with a range of other diseases (Supplementary Table S8). Among the identified diseases, we observed similarities for different forms of the same disease, for example types of retinitis pigmentosa or types of epilepsy. Some of these diseases share similarities with symptoms reported within COVID-19 patients such as cardiovascular diseases (atherosclerosis, cardiomyopathy, hypertension etc.) (Zhou et al., 2020b; Madjid et al., 2020); respiratory issues (airway hyper-responsiveness, inflammation) (Huang et al., 2020); neurological diseases (cerebellar ataxia, epilepsy) (Mithani et al., 2021; Povlow and Auerbach, 2021; Werner et al., 2021); and myopathy (Manzano et al., 2020; Versace et al., 2021). We also found that 42 of these 144 proteins had an association with various types of cancer.
Serving to confirm the findings of previous papers reviewed:
To identify whether there were any similarities or common location associations between the proteins, we grouped each of the proteins based on the body system/s they were found to be associated with (Supplementary Table S9). In doing so, we identified a range of overlap between proteins and systems (Figure 9). 52 proteins were found to be associated with the nervous system, six of which overlapped with the cardiovascular system, which is just under half of the cardiovascular-related proteins identified. Overlap could additionally be found with the respiratory system and gastrointestinal tract (GIT), systems associated with known COVID-19 complications. Additional locations/systems found to have protein associations included excretory system, facial region, skin, bone/muscle, thyroid, mitochondria/metabolic diseases and the immune system. Among the proteins associated with these, some showed overlap with other regions. This suggests that potential interruptions in some of these proteins could have multi-organ consequences, which may be associated with COVID-19.
FIGURE 9. Overlap of proteins between body systems. Proteins found to be associated with diseases were grouped based on body system location of the diseases. Key systems with known complications in COVID-19 disease were found to have overlapping protein associations
There is an Association Between Human Proteins, With Shared SARS-CoV-2 Sequences, and Autoimmunity
As reports of autoimmunity in COVID-19 continue to emerge (Bordet et al., 2020; Korem et al., 2020; Unsworth et al., 2020; Lui et al., 2021), of key interest was the association between the identified human proteins and whether they have a role in autoimmune diseases or are known autoantigens. Of the 223 human proteins, 50 were associated with autoimmune diseases, in both human and animal model settings (Supplementary Table S10). Among these 50 proteins, we found that some overlapped with multiple autoimmune diseases (Figure 10; Supplementary Table S11). Systemic lupus erythematosus (SLE) was found to have the most protein association, followed by multiple sclerosis (combined human and animal model, experimental autoimmune encephalomyelitis (EAE)). SLE shared the most overlap with other autoimmune diseases and some targets were shared across more than two autoimmune diseases. Many of the associations identified were due to gene single nucleotide polymorphisms (SNPs) and altered expression levels. However, eight of the proteins are known targets of autoantibodies and include key antibodies for assessing or diagnosing the associated diseases such as the myasthenia gravis autoantigen A-kinase anchor protein 12 (gravin), and histone 3, a nuclear target in SLE (Table 1). This suggests that the presence of some of these autoantibodies in COVID-19 patients without a history of autoimmune disease could be due to immune cross-reactivity.
Discussion
Using in silico immunoinformatic tools, potential B cell immunogenic epitopes in the SARS-CoV-2 proteome were predicted and further used to compare to global variants as well as explore the similarity to human proteins. In doing so, we identified eight structural epitopes containing mutations in at least one strain within these immunogenic regions.When comparing the epitopes to the human proteome, a variety of human proteins were identified to share sequences similar to SARS-CoV-2 proteins. Many of the identified human proteins were found to be associated with diseases, some of have which been reported to be related to COVID-19 symptoms and complications. Additionally, we show associations of these proteins to autoimmune diseases, such as SLE and MS. We further identified sequence similarities between SARS-CoV-2 immunogenic regions and human proteins which are localized in the extracellular region. These similarities and potential ease of access to circulating antibodies suggests the potential damaging cross-reactivity that can perpetuate a pathological condition. Finally, we analyzed and found that molecular mimicry may not be the mechanism for the thrombosis and thrombocytopenia syndrome occurring following vaccination with the AstraZeneca and Johnson & Johnson COVID-19 vaccines.
Presence of autoimmune antibodies can put you at increased risk of disease, or increasing the severity of existing conditions:
COVID-19 is associated with a series of multi-organ complications (Huang et al., 2020; Zaim et al., 2020). Many of the human proteins identified in this study, that share amino acid sequence similarities with the SARS-CoV-2 virus, play key roles in cellular functions, which if interrupted may result in altered cell function and therefore pathology. We found that clusters of proteins could be grouped based on their relationship to similar diseases and overlap to multiple body systems, some of which have been implicated in COVID-19 pathology, including respiratory, cardiovascular, gastrointestinal tract and nervous systems. Some of the broad examples of such diseases include epilepsy, cardiomyopathy and cerebellar ataxia, all of which have been reported in COVID-19 patients (Siripanthong et al., 2020; Mithani et al., 2021; Povlow and Auerbach, 2021; Werner et al., 2021). However, some of the diseases associated with the similar proteins may not result in a complication but instead confer a higher risk.Alzheimer’s Disease, macular degeneration and cardiovascular diseases were all diseases identified with proteins that shared sequence similarities to SARS-CoV-2 capable of making them the targets of autoantibodies. Pre-existing diagnosis for each of these have been found to predict higher risk of infection and greater severity and risks in COVID-19 (Chen et al., 2020; Huang et al., 2020; Ramlall et al., 2020; Yu et al., 2021). Many of the proteins identified to be associated with disease are intracellular and are therefore less likely to be immune targets. However, as the SARS-CoV-2 virus is an intracellular pathogen, the sequence similarities could alternatively have an impact on cellular functions which may result in the observed pathologies, independently of having the potential to be recognized by antibodies.
Interesting comment on how infection may break your autoimmune tolerance. And the autoantigenic sequences appear to be conserved between variants, so antigenic drift of the virus may not reduce your risk as was considered previously:
During COVID-19 infection, the release of intracellular proteins may be playing a role in breaking immune tolerance, allowing for the potential cross-reactivity of SARS-CoV-2 antibodies to self, or the increase of AAbs. This may be perpetuated through the recognition of the regions that are extracellular and therefore more likely to be visible to circulating antibodies. Interestingly, the SARS-CoV-2 spike and nucleoprotein alignments with human protein matches conforming to our criteria, are ones that do not contain mutations across different global variants, suggesting the potential for cross-reactivity to these proteins irrespective of the virus variant. Furthermore, according to the IEDB, there are several confirmed discontinuous B cell epitopes within the spike protein, which may also further expand the number of cross-reactive epitope targets to human proteins to be explored in future studies.
The authors concluded by discussing the need for further research and vaccine induced thrombosis thrombocytopenia syndrome. No conflicts of interest were declared:
The mechanism behind the thrombotic events occurring in some people following vaccination with the AstraZeneca and Johnson & Johnson adenovirus vectored vaccines is not known (Scully et al., 2021). Our findings suggest that molecular mimicry between the SARS-CoV-2 spike protein and proteins implicated in TTS and ITP, including PF4 and ADAMTS13, is unlikely to be the cause of these events. The vaccine induced thrombosis thrombocytopenia syndrome has been reported to be similar to autoimmune heparin-induced thrombocytopenia (aHIT) (Schultz et al., 2021), and therefore similar mechanisms may be involved. In aHIT, it has been suggested that structural changes in PF4 may be involved (Greinacher et al., 2017). Anti-PF4 antibodies are part of the diagnostic criteria for TTS (Greinacher et al., 2021). It has been hypothesized that free DNA in the vaccines may be a possible trigger of the anti-PF4 antibodies (Greinacher et al., 2021). However, further research into the formation of these anti-PF4 autoantibodies and the causes behind TTS following COVID-19 vaccination is required to identify potential interventions to prevent these events.
Autoimmune antibodies and specific conditions
Multiple sclerosis
Multiple sclerosis considered in this 2021 paper by Valéry Salle39:
Common human coronaviruses and multiple sclerosis
Seven types of coronavirus are known to infect humans (Table 1 ). The most common human coronaviruses circulating worldwide are OC43, HKU1, NL63, and 229E [18]. Multiple sclerosis is an immune-mediated demyelinating disease in which infectious pathogens could play a role in the pathogenesis of the disease. The possible involvement of human coronaviruses as an environmental trigger of multiple sclerosis (MS) is supported by several studies. Antibodies to coronaviruses OC43 and 229E were found in the cerebrospinal fluid of MS patients more frequently and in higher titers than that of matched controls [19]. Moreover, intrathecal antibody synthesis to OC43 and 229E coronaviruses has been found in 41% and 26% of MS patients, respectively [19]. Human coronavirus HCV-229E can replicate in cultures of various human neuronal and glial cell lines [20]. Human coronavirus 229E viral RNA has been detected in the brain tissue of MS patients [21]. Molecular mimicry has been proposed as a putative mechanism in the pathogenesis of MS. T-cell lines isolated from MS patients show cross-reactivity between myelin basic protein and viral antigens from the human respiratory coronavirus 229E [22].
Long-COVID
Long-COVID and autoantibodies targeting G-protein coupled receptors, an investigation by Wallukat et al (2021)40.
“G protein-coupled receptors (GPCRs) comprise the largest and most diverse family of integral membrane proteins that participate in different physiological processes such as the regulation of the nervous and immune systems. Besides the endogenous ligands of GPCRs, functional autoantibodies are also able to bind GPCRs to trigger or block intracellular signalling pathways, resulting in agonistic or antagonistic effects, respectively.”
“Autoantibodies targeting β1 and β2 adrenergic receptors, which are expressed by cardiac and airway smooth muscle cells, respectively, have an important role in the development of asthma and cardiovascular diseases. In addition, high levels of autoantibodies against the muscarinic acetylcholine receptor M3 as well as those targeting endothelin receptor type A and type 1 angiotensin II receptor have several implications in the pathogenesis of rheumatic diseases such as Sjögren syndrome and systemic sclerosis.41”
Highlights
•Sera from Long-COVID syndrome patients contained functionally active autoantibodies targeting G-protein coupled receptors.
•Autoantibodies target β2- and α1-adrenoceptors, angiotensin II AT1-, muscarinic M2-, MAS-, nociceptin- and ETA-receptors.
•Included syndromes were of neurological and cardiological origin, or a combination of both.
•Such autoantibody patterns have previously been seen in COVID independent neurological deficits and cardiovascular disease.
Abstract
Impairment of health after overcoming the acute phase of COVID-19 is being observed more and more frequently. Here different symptoms of neurological and/or cardiological origin have been reported. With symptoms, which are very similar to the ones reported but are not caused by SARS-CoV-2, the occurrence of functionally active autoantibodies (fAABs) targeting G-protein coupled receptors (GPCR-fAABs) has been discussed to be involved.
We, therefore investigated, whether GPCR-fAABs are detectable in 31 patients suffering from different Long-COVID-19 symptoms after recovery from the acute phase of the disease.
The spectrum of symptoms was mostly of neurological origin (29/31 patients), including post-COVID-19 fatigue, alopecia, attention deficit, tremor and others.Combined neurological and cardiovascular disorders were reported in 17 of the 31 patients. Two recovered COVID-19 patients were free of follow-up symptoms. All 31 former COVID-19 patients had between 2 and 7 different GPCR-fAABs that acted as receptor agonists. Some of those GPCR-fAABs activate their target receptors which cause a positive chronotropic effect in neonatal rat cardiomyocytes, the read-out in the test system for their detection (bioassay for GPCR-fAAB detection). Other GPCR-fAABs, in opposite, cause a negative chronotropic effect on those cells. The positive chronotropic GPCR-fAABs identified in the blood of Long-COVID patients targeted the β2-adrenoceptor (β2-fAAB), the α1-adrenoceptor (α1-fAAB), the angiotensin II AT1-receptor (AT1-fAAB), and the nociceptin—like opioid receptor (NOC-fAAB). The negative chronotropic GPCR-fAABs identified targeted the muscarinic M2-receptor (M2-fAAB), the MAS-receptor (MAS-fAAB), and the ETA-receptor (ETA-fAAB). It was analysed which of the extracellular receptor loops was targeted by the autoantibodies.
In their Italian study, Carfi et al. [1] indicated that only 12.6% of investigated patients did not develop any persistent symptoms after recovering from COVID-19. Most of the symptomatic post-infection COVID-19 patients suffered from neurological disorders, such as chronic fatigue syndrome, postural orthostatic tachycardia syndrome (PoTS) and dysautonomia [1]. However, other neurological diseases, such as transverse myelitis, acute necrotising myelitis, Guillain-Barré syndrome and others, have also been reported in several recent case reports on patients following SARS-CoV-2 infection [[2], [3], [4], [5], [6], [7], [8], [9]]. Similar results concerning the extent of post-COVID-19 symptoms were also obtained in a German study that showed only 22% of their investigated COVID-19 patients stayed free of post-disease symptoms [10].
Besides neurological manifestations, patients who recovered from COVID-19 also often developed cardiovascular implications [11]. The most prevalent abnormalities observed included myocardial inflammation, arrhythmia, tachycardia, bradycardia, and atrioventricular (AV) block [10,[12], [13], [14], [15], [16], [17], [18]]. In a large multi-centre study, including the intensive care units of 68 geographically diverse hospitals across the United States, Hayek and co-workers investigated 5019 critically ill COVID-19 patients. They observed that of these 5019 patients, 14% (701/5019) had an in-hospital cardiac arrest which was associated with poor survival, particularly among older patients.
It is a proven fact that autoimmune processes and the formation of functional autoantibodies (fAABs) directed against G-protein coupled receptors (GPCR) play a role in the development of neurological [[28], [29], [30]] and cardiovascular symptoms [31]. Therefore, in this present study, it was tested if such GPCR-fAABs might also be associated with the development of corresponding post-COVID-19 symptoms. We investigated virus-free sera from 31 recovered COVID-19 patients with respect to the occurrence of GPCR-fAABs.
These results correlate with the findings of precious studies eg M2 receptors and keratin synthesis. As they point out, autoantibodies against ANGII may be beneficial (through the inhibition of hypertension and fibrosis), but against ANG1-7 may be pathogenic (anti-inflammatory effects in models of cardiovascular disease and arthritis42), the net effect being cardiovascular symptoms in over half of the long-Covid patients tested.
3. Results
Several different GPCR-fAABs were identified in the 31 sera of recovered COVID-19 patients. All 31 investigated patients had between 2 and 7 different GPCR-fAAB (Table 1). This was a surprising unexpected effect. In healthy controls, which are included in many studies, these autoantibodies are only found in a small percentage [37,38]”.
Two functionally active autoantibodies, that were seen in almost all investigated former COVID-19 patients, were directed against the β2-adrenoceptor (β2-fAAB) and the muscarinic M2 receptor (M2-fAAB). These fAABs induced a positive and a negative chronotropic response on their targeted receptors, respectively.
Two other fAABs that were also present in 29 (90%) of the 31 investigated post-COVID-19 patients were directed against the angiotensin II AT1 receptor (fAT1-AAB) and the angiotensin 1-7 MAS receptor (MAS-AAB). These receptors belong to the renin angiotensin system (RAS) and cause a positive and negative chronotropic effect, respectively, when targeted by the respective fAABs.
Post-infection hair loss (alopecia) was experienced by 8 of the recovered patients. In sera of these patients, three additional GPCR-fAABs were discovered: the negative chronotropic ETA-fAAB (4/8), the positive chronotropic NOC-fAAB (5/8), and the positive chronotropic α1-AAB (3/8). Not every alopecia patient showed all three of these GPCR-fAABs. Instead, their occurrence varied, and a pattern is not yet detectable. As shown in (Table 1), 2 of the 31 investigated post COVID-19 patients developed fAABs without showing any symptoms.
A healthy gut biome and S2 antibody response
Another interesting finding by Geanes et al (2022) in that a healthy gut biome correlates to a stronger S2 antibody response43. The corollary to this is alarming, in that vaccination may promote antibodies to an otherwise potentially healthy gut biome:
There are two preliminary reports that found that antibodies elicited to SARS-CoV-2 could cross-react with proteins in the commensal gut microbiome51,52. One of these epitopes overlapped with the S2-78 peptide sequence we used for our immunization study. We also found high sequence similarity between S2-78 peptide and proteins found in bacteria. Moreover, we found that individuals with higher levels of pre-existing S2 antibodies before COVID-19 vaccination had significantly higher levels after immunization. Prior studies with influenza vaccines have shown that treatment with antibiotics and disruption of the microbiome may result in impairment of immunoglobulin neutralization49. These observations raised the hypothesis that the composition of the microbiome could influence antibody levels. Our findings identified high sequence conservation of SARS-like coronavirus spike proteins in viruses and bacteria and ascertained the possibility of the Pfizer-BioNTech BNT162b2 vaccine to boost immunity against more than just SARS-CoV-2. Future studies of components of both commensal gut bacteria and the virome should be carried out to determine how exposure to other bacteria and viruses impact the SARS-CoV-2 antibody response. A limitation of these findings is whether a neutralizing response occurs from gut bacteria exposure or if these antibodies recognize intact microbiome or if bacterial lysis must occur. Lastly, in the pursuit of generating cross-reactive antibody responses that could react with the microbiome, determinization of deleterious effects towards the microbiome or host proteins should be measured.
In summary, our data demonstrated that SARS-CoV-2 infection or vaccination elicited cross-reactive antibodies that target not only SARS-CoV-2, but related coronaviruses. Moreover, we showed that immunization with conserved peptide regions of SARS-CoV-2 induce cross-reactive antibodies in mice. Lastly, we provided evidence that suggested that the makeup of the gut microbiome could influence SARS-CoV-2 antibody levels. These data lay the groundwork for developing a pan-coronavirus vaccine that could elicit cross-reactive immunity to a broad range of coronavirus species. Further research will be needed to optimize this process in order to identify epitopes and vaccine platforms that induce protective immunity.
Risk to foetus
Extreme risk to the foetus by pathogenic autoimmune antibodies is discussed in this alarming 2021 paper by Wang et al44:
Abstract
This study, using a virus-free mouse model, explores the pathogenic roles of certain antibodies specific to the spike proteins of highly pathogenic coronaviruses such as the COVID-19 and the SARS-CoV viruses. Our data showed that these pathogenic antibodies, through a mechanism of Antibody Dependent Auto-Attack (ADAA), target and bind to host vulnerable cells or tissues such as damaged lung epithelium cells, initiate a self-attack immune response, and lead to serious conditions including ARDS, cytokine release, and death. Moreover, the pathogenic antibodies also induced inflammation and hemorrhage of the kidneys, brain, and heart. Furthermore, the pathogenic antibodies can bind to unmatured fetal tissues and cause abortions, postpartum labors, still births, and neonatal deaths of pregnant mice. Novel clinical interventions, through disrupting the host-binding of these pathogenic antibodies, can be developed to fight the COVID-19 pandemic. In addition, the new concept of ADAA explored by this study may be applicable to other infectious diseases, such as the highly pathogenic influenza infections. It should be noted that the majority of anti-spike antibodies are non-pathogenic, as only 2 of 7 monoclonal antibodies tested showed significant pathogenic effects.
Note that 45% of the pups exposed to anti-COVID-19 S1 spike protein antibodies became sick or died:
It was surprising that when the pathogenic polyclonal anti-COVID-19 S1 antibody was mixed with an equal amount of the non-pathogenic anti-COVID-19 N (50 μg + 50 μg), the sickness and death rate induced by the antibody mixture was significantly lower than that induced by the anti-COVID-19 S1 alone (Table 2). Moreover, the sickness and death rate induced by the highly pathogenic REGN10987 antibody also decreased significantly when a mixture of the antibody and other two non-pathogenic antibodies, CR3022-b6 and CC12.3, were injected (Table 2). The mixture consisted of 40 μg of REGN10987, 20 μg of CR3022-b6, and 20 μg of CC12.3. The data suggested that co-existing of non-pathogenic antibodies can reduce the pathogenicity of pathogenic antibodies.
Antibodies to spike protein induced antibody-dependent enhancement (ADE) and antibody dependent auto-attack (ADAA) were indicated in this mouse model. Previously it was concluded that aged mice were close animal models to humans:
Discussion
The current study revealed the pathogenic roles and the new mechanism of action (ADAA) of certain antibodies specific to the spike proteins of coronaviruses such as the COVID-19 virus and the SARS-CoV virus (Figure 8). We had discovered that in a mouse model, pre-injection of anti-influenza immune sera induced more severe infections than the mice infected with an influenza virus alone14 . Wang and co-workers reported that anti-SARS-CoV spike antisera promoted SARS infection through antibody-dependent enhancement (ADE) in vitro 22. Liu and co-workers reported that anti-SARS-CoV spike immune sera induced by a SARS-CoV vaccine caused acute lung injury by promoting MCP1 and IL-8 production and monocyte or macrophage recruitment and accumulation in SARS-CoV infected macaque models 23 . The previously reported mechanism of action (MOA) of these anti-spike antibodies is ADE-based, in that the antibodies enhance viral infectivity24The current study, revealed for the first time, the self-cell targeting MOA of pathogenic antibodies, in which the antibodies bind to host vulnerable cells or tissues and mislead immune responses to attack host-self (ADAA). Our study also explored a new mechanism of pathogenisis (MOP) of highly pathogenic viral infections. The MOP is caused by the pathogenic antibodies inducible by highly pathogenic viruses such as the COVID-19 virus and SARS-CoV virus. Moreover, the pathogenic antibodies may be related to the cause of infection-related autoimmune diseases, including those in COVID-19 long haulers, through ADAA.
As discussed earlier, exposure to the virus may be less pathogenic than repeated exposure to vaccinal epitopes, especially during or before pregnancy:
Better vaccines
It was surprising that when the pathogenic anti-COVID-19 S1 antibodies was mixed with an equal amount of the non-pathogenic anti-COVID-19 N antibodies, the sickness and death rates caused by the antibody mixture was significantly decreased compared to the results of the injected anti-COVID-19 S1 antibody alone (Table 2 and Figure 1C). A similar result was observed with the highly pathogenic REGN10987 as well with an antibody mixture of the REGN10987 and the two non-pathogenic monoclonal antibodies of CR3022-b6 and CC12.3 (Table 2 and Figure 1C). The data suggested that co-existence of non-pathogenic antibodies can reduce the ADAA of pathogenic antibodies. Thus, a vaccine capable of inducing multivalent antibodies may be safer, in which at least one kind of antibody is of the non-pathogenic kind that induces fewer adverse reactions. One example of such a vaccine is the traditional inactivated viral vaccine (e.g. inactivated COVID-19 vaccine) which induces multivalent antibodies specific for multiple antigens of a virus.As another example, a recombinant or mRNA COVID-19 vaccine capable of inducing the antibodies specific to not only the spike protein but also to the nucleocapsid proteins, or a non-spike protein of the SARS-CoV-2 virus may be safer (patent pending). Despite the mechanism of action being unclear, it is not likely that the non-pathogenic antibodies affected the ADA actions of the pathogenic antibodies through competitive binding since neither the anti-COVID-19 S1 nor the anti-COVID-19 N bind to the same antigens. Neither the REGN10987 nor the other two non-pathogenic antibodies bind to the same epitope of the S1 protein of the COVID-19 virus. We hypothesize that non-pathogenic antibodies affect the ADAA of pathogenic antibodies through diluting and space obstructing or interrupting the attachment of pathogenic antibodies to vulnerable cells or tissues.
Novel clinical interventions for diagnosis and treatment, including improved vaccines based on the ADAA of pathogenic antibodies, can be developed. In addition, the new concept and the mechanism of ADAA explored by this study may also be applicable to other infectious diseases, such as highly pathogenic influenza infections (study ongoing).
Case reports
Chen et al published this at the end of 2021 as confirmatory case reports were presenting45:
Abstract
Coronavirus disease 2019 (COVID-19) pandemic caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has led to an unprecedented setback for global economy and health. Vaccination is one of the most effective interventions to substantially reduce severe disease and death due to SARS-CoV-2 infection. Vaccination programmes are being rolled out globally, but most of these vaccines have been approved without extensive studies on their side-effects and efficacy. Recently, new-onset autoimmune phenomena after COVID-19 vaccination have been reported increasingly (e.g. immune thrombotic thrombocytopenia, autoimmune liver diseases, Guillain-Barré syndrome, IgA nephropathy, rheumatoid arthritis and systemic lupus erythematosus). Molecular mimicry, the production of particular autoantibodies and the role of certain vaccine adjuvants seem to be substantial contributors to autoimmune phenomena. However, whether the association between COVID-19 vaccine and autoimmune manifestations is coincidental or causal remains to be elucidated. Here, we summarize the emerging evidence about autoimmune manifestations occurring in response to certain COVID-19 vaccines. Although information pertaining to the risk of autoimmune disease as a consequence of vaccination is controversial, we merely propose our current understanding of autoimmune manifestations associated with COVID-19 vaccine. In fact, we do not aim to disavow the overwhelming benefits of mass COVID-19 vaccination in preventing COVID-19 morbidity and mortality. These reports could help guide clinical assessment and management of autoimmune manifestations after COVID-19 vaccination.
Potential mechanisms inducing autoimmunity through vaccine adjuvants.
Schematic depiction of mechanisms inducing vaccine-induced immune thrombotic thrombocytopenia following COVID-19 vaccination.
CONCLUSION
In the light of the information discussed above, emerging evidence has indicated that new onset of autoimmune manifestations including VITT, autoimmune liver diseases, GBS and IgA nephropathy appears to be associated with COVID-19 vaccines (Table 2). The plausible mechanisms by which COVID-19 vaccines lead to autoimmune manifestations include molecular mimicry, the production of particular autoantibodies and the role of certain vaccine adjuvants. Further studies are warranted to elucidate the underlying biological mechanisms and identify the exact causality.
No conflicts of interest were declared.
Thrombocytopenia
A recently published paper by Nunez-Castilla et al (28th June ‘22)46 hypothesises that COVID-19 infection may induce the production of TQLPP-specific antibodies against its epitope that can cross-react with human thrombopoietin (hTPO), a glycoprotein hormone produced by the liver and kidney which regulates the production of platelets.
The current research has indicated a high possibility of cross-reactivity between the Spike protein of SARS-CoV-2 and hTPO involving the TQLPP epitope. This event affects the production of platelets leading to thrombocytopenia. Additionally, the cross-reactivity with other TQLPP-containing proteins, e.g., NEK10, also supports the hypothesis. Also, researchers reported that the presence of neutralizing antibodies against peptides with TQLPP in the plasma of the COVID-19 recovered patients, especially in severe cases. Which further adds credence to the research hypothesis. Notably, the COVID-19 vaccines that are developed based on Spike protein of SARS-CoV-2 can cause thrombocytopenia.
The authors of the current study propose that scientists should consider avoiding potential predictable autoimmune interference for the future development of the COVID-19 vaccines. Another interesting point to note is the evolutionary trend in the TQLPP motif, i.e., it might not remain in the Spike region. Such an occurrence has been observed in the SARS-CoV-2 Gamma variant. The neutralizing antibodies targeting the NTD supersite may become ineffective against the SARS-CoV-2 variant due to rapid mutation. However, for future COVID-19 vaccines, protein engineering of the TQLPP motif may reduce the possibility of thrombocytopenia and provide long-term protection against future SARS-CoV-2 variants.47
Thrombocytopenia is a condition associated with low platelet counts. The cytokine thrombopoietin regulates platelet count. Previous studies have reported that thrombocytopenia can increase the COVID-19 mortality rate by about five times.
In contrast to some older studies, they made both sequence and structural in silico comparisons of human and spike protein against the Immune Epitope Database (IEBD):
Abstract
Molecular mimicry between viral antigens and host proteins can produce cross-reacting antibodies leading to autoimmunity. The coronavirus SARS-CoV-2 causes COVID-19, a disease curiously resulting in varied symptoms and outcomes, ranging from asymptomatic to fatal. Autoimmunity due to cross-reacting antibodies resulting from molecular mimicry between viral antigens and host proteins may provide an explanation. Thus, we computationally investigated molecular mimicry between SARS-CoV-2 Spike and known epitopes. We discovered molecular mimicry hotspots in Spike and highlight two examples with tentative high autoimmune potential and implications for understanding COVID-19 complications. We show that a TQLPP motif in Spike and thrombopoietin shares similar antibody binding properties. Antibodies cross-reacting with thrombopoietin may induce thrombocytopenia, a condition observed in COVID-19 patients. Another motif, ELDKY, is shared in multiple human proteins, such as PRKG1 involved in platelet activation and calcium regulation, and tropomyosin, which is linked to cardiac disease. Antibodies cross-reacting with PRKG1 and tropomyosin may cause known COVID-19 complications such as blood-clotting disorders and cardiac disease, respectively. Our findings illuminate COVID-19 pathogenesis and highlight the importance of considering autoimmune potential when developing therapeutic interventions to reduce adverse reactions.
Figure 1. Molecular mimicry with autoimmune potential across SARS-CoV-2 Spike. (a) Overview of molecular mimics (solid arrow: 3D-mimic, dashed arrow: AF-3D-mimic) for Spike in the linear sequence showing Spike domains (NTD: N-terminus domain of S1 subunit (green), RBD: receptor binding domain of S1 subunit (orange), CTD: C-terminus domain of S1 subunit (cyan), S2: S2 domain (purple)) as predicted by Pfam [51] based on the NCBI reference sequence (YP:009724390.1). The boundary between the S1 and S2 subunits is indicated at S1/S2. (b) Surface representation of Spike (PDB id: 6XR8 [23]) colored by subunit (pink, beige, light blue) with residues colored by number of occurrences in a molecular mimic (blue: 1, green: 2, purple: 3, orange: 4 or more). Structural visualization generated with PyMOL 2.5.0 [30]. (c) The number of occurrences of the sequence motif in human RefSeq Select isoforms arranged in order from the N-terminus to the C-terminus and colored by predominant secondary structure element (magenta: α-helix, yellow: β-sheet, blue: coil) based on Spike PDB id 6XR8 chain A.
In all instances, the ELDKY motif is found in an α-helix, resulting in the high degree of structural similarity found for this motif across proteins and bolstering the possibility for molecular mimicry. The ELDKY occurrence with the largest RMSD (0.46 Å) is found in the leucine-zipper dimerization domain of cGMP-dependent protein kinase 1 (PRKG1) (Figure S6) whose phosphorylation targets have roles in the regulation of platelet activation and adhesion [72], smooth muscle contraction [73], and cardiac function [74]. Additionally, PRKG1 regulates intracellular calcium levels via a multitude of signaling pathways [75]. The ELDKY motif is also found in tropomyosin alpha-1 (TPM1), a homolog of the AF-3D-mimic tropomyosin alpha-3 (TPM3). Tropomyosins (TPMs) are involved in the regulation of the calcium-dependent contraction of striated muscle.
To recap, the motif ELDKY is shared in multiple human proteins such as PRKG1 which is involved in platelet activation and calcium regulation, and tropomyosin, which is linked to cardiac disease (iehypertrophic cardiomyopathy HCM or abnormally thick heart muscle, dilated cardiomyopathy DCM where the heart cannot pump blood effectively because the left ventricle, the main pumping chamber, is enlarged and weakened and left ventricular noncompaction LVCN, a congenital condition)48
This is, again extremely concerning as autoimmunity is not something you can just switch off once started. There is no magic pill to reset the immune system.
A typical report, from a Doctor of Nursing Practice:
As these motifs are shared in so many different human proteins antigenic stimulation may continue indefinitely, with both coagulation disorders, coronary heart disease and cardiomyopathies a progressive risk to health that may take some time to present symptoms and any pre-existing cardiovascular conditions being rendered more severe.
For PRKG1, cross-reactive Spike antibodies targeting ELDKY may react with the motif, affecting PRKG1′s role in the regulation of platelet activation and adhesion and thus providing another avenue for thrombocytopenia or other blood clotting disorders. Antibodies that cross-react with PRKG1 may also alter calcium levels, thus affecting TPM function. For TPM1, cross-reactive Spike antibodies targeting the ELDKY motif may result in coronary heart disease, as low-level autoantibodies against this protein have been associated with increased risk for this condition [78] and TPM1 and TPM3 are cardiac disease-linked antigens [77]. Cardiac disease, including myocardial injury and arrhythmia, can be induced by SARS-CoV-2 infection [79] and myocarditis has been found to develop in some individuals following vaccination against SARS-CoV-2 [80]. Furthermore, COVID-19 has been found to increase the risk and long-term burden of several cardiovascular diseases, with COVID-19 severity being proportionate to increased risk and incidence [81].
4. Conclusions
We find that molecular mimics with high autoimmune potential are often found in clusters within Spike. Some clusters have several molecular mimics whose motifs are also found multiple times in the human proteome. Molecular mimics located in α-helices tend to have high structural similarity as can be expected based on the regular conformation of the helix, but also some molecular mimics in coil regions are remarkably similar. Our results on the TQLPP motif, located in a coil region, suggest a worrisome potential for cross-reactivity due to molecular mimicry between Spike and hTPO involving the TQLPP epitope that may affect platelet production and lead to thrombocytopenia. Further, cross-reactivity with other TQLPP-containing proteins such as NEK10 cannot be dismissed based on our in-silico results, but in-vivo validation is required. The presence of neutralizing antibodies against peptides with TQLPP in COVID-19 patients’ convalescent plasma [82], particularly in severe and fatal cases [16] adds credence to our result. It is also interesting to note that antibodies against a TQLPP-containing peptide were found in the serum of pre-pandemic, unexposed individuals [83]. Prior infection with a different human coronavirus cannot explain the cross-reactivity observed in the unexposed group because TQLPP is situated in a region with low amino acid conservation [83]. Rather, this suggests the presence of an antibody for an unknown epitope with an affinity for the TQLPP region in Spike. The COVID-19 vaccines designed to deliver the Spike protein from SARS-CoV-2, like COVID-19 infection itself, can cause thrombocytopenia [53,84,85,86] and it is plausible that cross-reactivity can titrate the serum concentration of free hTPO. The TQLPP motif is changing in the SARS-CoV-2 variants and evolutionary trends of the motif suggest it may not remain in Spike. RMSD values between wild-type TQLPP and TQLPP in five variants of concern range from 0.21–1.78 Å (Table S3). In the Gamma variant, a P26S mutation has changed TQLPP to TQLPS and two additional mutations are located just before the motif at L18F and T20N in the NTD supersite, while the Delta variant is mutated at T19R [87]. The first Omicron variant (21K or BA.1), however, has no amino acid substitutions near the TQLPP motif, while a closely related Omicron variant (21L or BA.2) contains a 9 nucleotide deletion that results in the loss of 60% of the TQLPP motif (L24-, P25-, P26-) [87]. Neutralizing antibodies targeting the NTD supersite may rapidly lose efficacy against the evolving SARS-CoV-2. While the current COVID-19 vaccines remain safe and efficacious, we postulate that protein engineering of the TQLPP motif and possibly the NTD supersite for future COVID-19 vaccines may reduce the risk for thrombocytopenia and improve long-term vaccine protection against evolving variants.
We highlight two epitopes of particular interest in our investigation of molecular mimicry in SARS-CoV-2. For one epitope, we find the TQLPP motif and an interacting antibody with which we perform a computational investigation into antibody binding properties of the tentative molecular mimic. The results show that the same antibody may be able to bind TQLPP-containing epitopes in different proteins and that the TQLPP motif tends to be found in similar conformations despite being in a loop or coil. For the other epitope, we find the ELDKY motif with potential for protective immunity and with high structural similarity. High structural similarity can be expected for α-helical structures, and, if the sequence is identical, molecular mimicry results. Altogether, these are examples of molecular mimicry that may play a role in the autoimmune or cross-reactive potential of antibodies generated by the immune system against SARS-CoV-2 Spike, but it must be noted that these results have not been experimentally verified. Still, computational investigations into the autoimmune potential of pathogens like SARS-CoV-2 are important for therapeutic intervention and when designing vaccines to avoid potential predictable autoimmune interference.
The authors declared no conflict of interest.
IgG4-Related Disease (IgG4-RD)
Relates to a peer reviewed paper published in December 2022 by Irrgang et al that found abnormally high levels of IgG4 antibodies 2010 days after the 3rd dose of mRNA transfection agents, which were even more elevated upon re-infection: Class switch towards non-inflammatory, spike-specific IgG4 antibodies after repeated SARS-CoV-2 mRNA vaccination49.
Fig. 1. Longitudinal analyses of vaccine induced antibody response.
(A) Schematic representation of the human immunoglobulin heavy chain gene locus. 5′ of each functional C-region (except Cδ) switch (S) regions are positioned directing class-switch recombination. Gene segments denoted by ψ resemble pseudogenes (B) 29 volunteers received three doses of the mRNA vaccine Comirnaty as detailed in Table 1. Serum samples were collected at a median of ten days after each vaccination (post first, post second, post third) as well as during follow-up visits at 210 days after the second vaccination (FU second) and 180 days after the third vaccination (FU third). Ten individuals experienced a breakthrough infection in the time frame between post third and FU third (indicated by grey circles). The different IgG subclasses were quantified by flow cytometry using recombinant monoclonal receptor binding domain (RBD)-antibodies as a standard. The median MFI of three negative sera were used to set the background for each subclass. For visualization purposes, all sera with MFI values below the background were set to 0.1 μg/ml. The lowest limit of quantification (LLoQ) is indicated in each graph by a dotted line and represents the lowest amount of the respective standard mAbs, which was detected (1.56 μg/ml for IgG2, IgG3 and IgG4; 5.6 μg/ml for IgG1). Depicted are individual donors and the respective median. n.a. = not analyzed. For the sake of clarity only statistical comparisons between post second, FU post second, and post third are shown irrespective of statistical significance. (C) The proportion of the different IgG subclasses of the total anti-S IgG response is shown for the four last time points. Depicted are the means of each IgG subclass. Over-time comparison within one group was done by Kruskal-Wallis test followed by Dunn’s multiple comparisons test. *p < 0.05, **p < 0.01, ***p < 0.001, ****p < 0.0001, and n.s. indicates not significant.
IgG4 related diseases can affect many organs and promote cancers or cancer-like neoplasms. The rheumatology.org website is an excellent resource50.
Early diagnosis is important to prevent serious organ damage, but this can be challenging:
Fast Facts
The condition tends to affect middle-aged to elderly individuals but can also affect children. Unlike many autoimmune diseases, IgG4-RD tends to affect males more often than females.
IgG4-RD, a multi-organ disease, has a tendency for the following organs: pancreas, bile ducts, lacrimal glands, major salivary glands (parotid, submandibular, sublingual), lungs, kidneys, aorta, meninges, thyroid gland.
Some patients have levels of IgG4 in their blood that are twenty or thirty times higher than the upper limit of normal. In a significant minority of patients, however, the serum IgG4 concentration is normal.
Patients may have active disease with no signs or symptoms for months or even years before the diagnosis is made, which can cause organ damage before the patient is even aware of being sick.
If diagnosed before serious organ damage has occurred, IgG4-RD typically responds well to treatment but chronic therapy is necessary.
IgG4-related disease is an immune-mediated condition, meaning that it involves the occurrence of disease in organs as the result of a dysregulated immune system. Increasing evidence suggests that IgG4-RD is an autoimmune condition, much like rheumatoid arthritis and systemic lupus erythematosus. The classic IgG4-RD patient is a middle-aged to elderly individual–more likely to be male than female. In rare cases, the disease also affects children.
How Is IgG4-Related Disease Treated?
If diagnosed before serious organ damage has occurred, IgG4-RD typically responds well to treatment but chronic therapy and the attempts to avoid side-effects of treatment, particularly glucocorticoids, remain the rule. Glucocorticoids are typically viewed as the initial treatment of IgG4-RD, but the shortcomings of this treatment approach are widely appreciated. Although nearly all patients with IgG4-RD respond to glucocorticoids, approximately 40% of those fail to achieve complete remission or relapse within one year, even if glucocorticoids are continued at a minimum of 5 mg/day. The disease often recurs after prednisone tapering, as well.
The role of conventional DMARDs in IgG4-RD is not clear, and much evidence suggests that the impact of these drugs in the absence of prednisone is small. Rituximab, however, is frequently an excellent treatment for IgG4-RD and it is not typically associated with many of the adverse effects linked to glucocorticoids. Other treatment strategies are now being developed based on the large amount of information learned in recent years about the pathophysiology of IgG4-RD.
Further information:
Rituximab51 is a chimeric monoclonal antibody against the protein CD20 , which is primarily found on the surface of immune system B cells . [5] When it binds to this protein it triggers cell death.
Adverse events
Serious adverse events, which can cause death and disability, include:
Severe infusion reaction
Cardiac arrest
Cytokine release syndrome
Tumor lysis syndrome, causing acute kidney injury
Infections
Progressive multifocal leukoencephalopathy (PML) caused by JC virus reactivation
Hepatitis B reactivation
Other viral infections
Progressive multifocal leukoencephalopathy (PML) caused by JC virus reactivation
Immune toxicity, with depletion of B cells in 70% to 80% of lymphoma patients
Pulmonary toxicity
Bowel obstruction and perforation
Prednisone52 is a glucocorticoid medication mostly used to suppress the immune system and decrease inflammation in conditions such as asthma, COPD, and rheumatologic diseases. It is also used to treat high blood calcium due to cancer and adrenal insufficiency along with other steroids. It is taken by mouth.
Common side effects with long-term use include cataracts, bone loss, easy bruising, muscle weakness, and thrush. Other side effects include weight gain, swelling, high blood sugar, increased risk of infection, and psychosis. It is generally considered safe in pregnancy and low doses appear to be safe when breastfeeding. After prolonged use, prednisone needs to be stopped gradually.
Prednisone is a prodrug and must be converted to prednisolone by the liver before it becomes active. Prednisolone then binds to glucocorticoid receptors, activating them and triggering changes in gene expression.
Disease-modifying antirheumatic drugs (DMARDs)53 comprise a category of otherwise unrelated disease-modifying drugs defined by their use in rheumatoid arthritis to slow down disease progression. The term is often used in contrast to nonsteroidal anti-inflammatory drugs (which refers to agents that treat the inflammation, but not the underlying cause) and steroids (which blunt the immune response but are insufficient to slow down the progression of the disease).
The term "antirheumatic" can be used in similar contexts, but without making a claim about an effect on the disease course. Other terms that have historically been used to refer to the same group of drugs are "remission-inducing drugs" (RIDs) and "slow-acting antirheumatic drugs" (SAARDs).
Baicalin is of therapeutic value here by selectively regulating follicular regulatory T cell differentiation, thus suppressing autoimmune reactivity and helping to reduce the symptoms but without the adverse events.
Yang et al (2020) investigated its effectiveness at treating a related autoimmune condition, lupus54:
Abstract
Baicalin is a natural compound isolated from Chinese herb, which has been reported as an anti-inflammatory drug. Here, we demonstrated that Baicalin treatment could reduce urine protein, inhibit anti-ds-DNA antibody titers, and ameliorate lupus nephritis in MRL/lpr lupus-prone mice. Baicalin inhibited Tfh cell differentiation and IL-21 production, but promoted Foxp3+ regulatory T cell differentiation including part of follicular regulatory T (Tfr) cells. Intravenous injection of Baicalin-induced Foxp3+ regulatory T cells could relieve nephritis, inhibit Tfh cell differentiation and IL-21 production. Baicalin inhibited mTOR activation, reduced mTOR agonist-mediated Tfh cell expansion and increased Tfr cells. These data suggest that Baicalin attenuates lupus autoimmunity by up- and downregulating the differentiation of Tfr cells and Tfh cells, respectively. Baicalin and ex vivo expanded Foxp3+ regulatory T cells are promising therapeutics for the treatment of lupus.
It is also of value in preventing and treating vascular disease such as atherosclerosis55.
And in 2019, Da et al wrote a paper on how it can be used to protect the skin from an IgG4-related autoimmune mediated blistering disorder (paywalled):
Baicalein protects normal human epidermal keratinocytes against bullous pemphigoid immunoglobulin G-induced alteration56.
The Kampo medicines Sho-saiko-to and Sairei-to have been used to relieve bullae formation in patients with BP (Supplemental Table 1). Ou-gon is derived from Scutellaria baicalensis Georgi roots and commonly included in both Sho-saiko-to and Sairei-to. The flavone, 5,6,7-trihydroxyflavone (baicalein) (Supplemental Fig. 1), a major compound in Ou-gon, is known to have anti-inflammatory activity and inhibitory effect on reactive oxygen species (ROS) production in NG108-15 cells. The aim of the present study was to elucidate the action mechanisms of baicalein by investigating its inhibitory effects against anti-BP antibody-induced cell damage, intracellular ROS accumulation, interleukin (IL)-6 and IL-8 production, and cell detachment in cultured normal human epidermal keratinocytes (NHEKs) in vitro.
In the abstract by R Gundry (8 Nov. 2021)57 he describes how a PULS score was taken from 566 patients aged 28-97, equal numbers M-F, both 3 to 5 months before the first shot and from 2 to 10 weeks following the 2nd mRNA COVID shot.
In conclusion, the mRNA vacs numerically increase (but not statistically tested) the markers IL-16, Fas, and HGF, all markers previously described by others for denoting inflammation on the endothelium and T cell infiltration of cardiac muscle, in a consecutive series of a single clinic patient population receiving mRNA vaccines without a control group.
Soluble Fas (sFas) is an inhibitor of apoptosis, and markers for that increased from 22+/- 15 above the norm to 46+/-24 above the norm post vax, an average increase of 209%:
Soluble FAS ligand was found to be associated with elevated IgG458 by van Asten et al (2021), yet another factor to consider as this will also be elevating the risk of developing IgG4 related autoimmune disorders such as lupus:
We performed a screen using a secreted protein library to identify novel factors that promote this process and may be used to combat undesired Ab formation. We tested the differentiating capacity of 756 secreted proteins on human naive or memory B cell differentiation in a setting with suboptimal T cell help in vitro (suboptimal CD40L and IL-21). High-throughput flow cytometry screening and validation revealed that type I IFNs and soluble FAS ligand (sFASL) induce plasmablast differentiation in memory B cells. Furthermore, sFASL induces robust secretion of IgG1 and IgG4 Abs, indicative of functional plasma cell differentiation. Our data suggest a mechanistic connection between elevated sFASL levels and the induction of autoreactive Abs, providing a potential therapeutic target in autoimmunity.Indeed, the modulators identified in this secretome screen are associated with systemic lupus erythematosus and may also be relevant in other autoimmune diseases and allergy.
The concentration of serum sFasL in patients with autoimmune diseases washigher than that in normal individuals. sFasL could reduce arthritis in collagen induced arthritis (CIA) mice model by subcutaneous injection. Conclusion: sFasL may be involved in either induction of apoptosis or autoimmune diseases.
Figure 5 Cell apoptosis induced by different doses of sFasL (25, 50 and 100 μg/L).
Figure 6 Levels of soluble FasL in serum from patients with different diseases. Cont: Serum from healthy individuals; IDDM: Serum from patients with IDDM; SLE: Serum from IDDM; RAa: Serum from RA patients with activated stage; Ca-ga: Serum from patients with gastric cancer; Leuk: Serum from patients with leukemia; Shadow bar: Serum level detected by commer-cial sFasL kit. Open bar: Serum level detected by anti-sFasL antibody.
IgG4-related Cardiovascular Disease
In 2018, Oyama-Manabe et al listed a wide spectrum of IgG4-related cardiovascular diseases, including aortitis, periaortitis, arteritis, periarteritis, coronary artery involvement and pericarditis60.
They discussed how IgG4 related autoimmunity can account for 50% of all inflammatory abdominal aortic aneurysms, so involvement must considered whenever a case is reported.
The abdominal aorta is most frequently affected. There are many more useful radiological images and case histories in the full paper, but this gives a good indication of the range of pathologies IgG4 can cause:
Immunoglobulin G4 (IgG4)-related disease can affect the cardiovascular system, including the coronary arteries and pericardium and especially the walls of large and medium-sized vessels. The presence of coronary involvement is critical, as this condition can cause myocardial ischemia or sudden cardiac death. Although histopathologic examination remains the reference standard for detecting organ involvement and diagnosing IgG4-related disease, obtaining biopsy or surgical specimens from the vessel wall is still challenging. Because patients may be only mildly symptomatic, noninvasive imaging evaluation of IgG4-related cardiovascular disease (CVD) has an essential role in not only the diagnosis but also the management of this condition. Multidetector CT is a useful noninvasive examination for establishing the primary diagnosis and defining anatomic landmarks and their relationships. The spectrum of vessel involvement is vast, with varied manifestations. Radiologists should be familiar with inflammatory vasculitis, aneurysmal change, and pseudotumor formation in all vessels and the distribution of these conditions throughout the body.
Immunoglobulin G4 (IgG4)–related disease is a newly recognized disease entity characterized by the infiltration of IgG4-positive plasma cells and fibrosis in systemic organs and the elevation of serum IgG4 levels (1). In 2001, patients with autoimmune pancreatitis were found to have elevated serum concentrations of IgG4 (1). Since Kamisawa et al (2) proposed the concept of IgG4-related autoimmune disease in 2003, IgG4-related lesions similar to those of autoimmune pancreatitis have been identified in several extrapancreatic organs, including the bile ducts, gallbladder, lymph nodes, retroperitoneum, kidneys, and lungs (3–5).
Cardiovascular involvement in IgG4-related disease, such as aortitis, arteritis, periaortitis, periarteritis, and inflammatory aneurysm, also has been detected, mainly in the abdominal aorta (6–9). IgG4-related inflammatory abdominal aortic aneurysms, accounting for approximately 5% of all surgical abdominal aortic aneurysms and 50% of all inflammatory abdominal aortic aneurysms (9), are one of the most common findings of IgG4-related disease (6). Aneurysm or dissection of the thoracic aorta associated with IgG4-related disease also has been sporadically reported (10,11).
Figure 1a
Figure 1b
Figure 1c
Figure 1d
IgG4-related inflammatory aortic aneurysm in an 83-year-old woman.(a, b) Cross-sectional macroscopic images of a resected abdominal aortic wall with hematoxylin-eosin (a) and Verhoeff–Masson trichrome (b) staining show lymphoplasmacytic infiltration (arrowheads in a) with irregular thickening involving mainly the adventitia (white arrow) and to a lesser extent the media (ie, inner layer) (black arrow). (Original magnification, ×20.) The specimen with Verhoeff–Masson trichrome staining shows dense fibrosis. (c, d) High-power-field photomicrographs stained with hematoxylin-eosin (c) and immunostained for IgG4 (d) show the lymphoplasmacytic infiltrate (c) and extensive dense infiltrate of IgG4-positive plasma cells (d) within the aortic wall, mainly in the adventitia. (Original magnification, ×400.) The ratio of IgG4-positive cells to IgG-positive cells was almost 100%.
Figure 2a
Figure 2b
Figure 2c
IgG4-related aortitis and periaortitis in a 69-year-old man.(a, b) Axial contrast-enhanced delayed phase CT images show homogeneously enhanced wall thickening of the left subclavian and brachiocephalic arteries (arrows in a) and abdominal aorta (arrowheads in b). (c) Coronal FDG PET/CT fusion image shows abnormal focal FDG uptake, indicative of active inflammation, at the levels of the left subclavian and brachiocephalic arteries (arrows) and abdominal aorta (arrowhead).
IgG4-related Coronary Arteritis, Periarteritis, and Aneurysm
Coronary artery involvement such as coronary arteritis and aneurysms, which manifest as periarterial fibrosclerotic thickening that occurs as a pseudotumor formation surrounding the coronary arteries, has been reported relatively recently (34–37). Because there is limited general awareness of this disease among physicians, the radiologist may be the first to detect the coronary involvement.
Figure 9a
Figure 9b
IgG4-related coronary aneurysm in a 73-year-old man.(a) Axial FDG PET/CT image shows focal uptake of FDG in a pseudotumor (arrow), with an SUVmax of 4.0, at the right atrioventricular groove. (b–d) ECG-gated coronary CT angiographic volume-rendered reconstruction (b), curved planar reconstruction (c), and axial image (d) show a large pseudotumor (arrow), seen as the pigs-in-a-blanket sign, in an RCA aneurysm (diameter, 27 mm) without luminal stenosis or dilatation. The patient also has a left circumflex artery aneurysm. (e) Follow-up axial CT image obtained 1 year later, after steroid administration, shows a marked treatment response: The diameter of the RCA aneurysm has decreased to 12 mm (arrow).
IgG4-related Pericarditis
Clinical cases involving IgG4-related pericarditis are limited (41–43). Sakamoto et al (43) reported that two patients with IgG4-related pericarditis had a fatal outcome and suggested that IgG4-related pericarditis might have a rapid clinical course. Although we experienced one case of IgG4-related pericarditis, with a thickened pericardium and focal FDG uptake without massive effusion (Fig 10), this case could have represented constrictive pericarditis and massive pericardial effusion.
Figure 10a
Figure 10b
IgG4-related pericarditis in a 43-year-old man.(a) Axial nonenhanced CT image shows a thickened pericardium (arrow) without pericardial effusion. (b) Corresponding FDG PET/CT image shows focal FDG uptake (SUVmax, 3.7) in the thickened pericardium (arrow).
Characteristic Features of IgG4-related CVD, Takayasu Arteritis, Giant Cell Arteritis, and Atherosclerosis:
Treatment and Therapeutic Response Monitored with Imaging
Treatment with steroids is most beneficial during the early stages of IgG4-related CVD, and it possibly prevents the progressive involvement of other organs (33). At longitudinal assessment, some patients may have diminished disease activity without having undergone treatment. We encountered a case of IgG4-related disease involving sclerosing mesenteritis that manifested as a pseudotumor, which decreased in size during follow-up without any treatment (Fig 6). However, the patient subsequently developed bilateral common iliac artery involvement and multiple coronary stenoses due to IgG4-related CVD.
In contrast, Mavrogeni et al (57) reported thatrelapses are not unusual and existing lesions usually do not resolve completely. According to the Japanese consensus criteria for IgG4-related disease, the starting dose of prednisolone should be 0.5–0.6 mg/kg per day (22). Treatment is often effective within 2–4 weeks, allowing the steroid dose to be tapered within approximately 2 months. In cases of life-threatening multiple-organ disease, a second agent such as rituximab is often added to the treatment regimen (58).
Tajima et al (27) reported that high-dose corticosteroid therapy might increase the risk of rupture of developed aneurysms by making the arterial wall thinner (27). In our case, steroid therapy was effective and led to a marked reduction in the size of the pseudotumor around the patient’s coronary arteries (Fig 9).
Disclosures of Conflicts of Interest.—N.O.M. Activities related to the present article: disclosed no relevant relationships. Activities not related to the present article: consultant for Canon Medical Systems, grants or grants pending from Japan Society for the Promotion of Science (JSPS) KAKENHI. Other activities: payment for lectures from Daiichi-Sankyo, Philips Medical Systems, Eisai, Bayer Healthcare, and Canon Medical Systems. K.K. Activities related to the present article: disclosed no relevant relationships. Activities not related to the present article: grants or grants pending from AMED, JSPS KAKENHI, Hitachi Medical Systems, and Bayer Healthcare; payment for lectures from Hitachi Medical Systems, Daiichi-Sankyo, Bayer Healthcare, GE Healthcare, Philips Medical Systems, Siemens Healthineers, and Canon Medical Systems. Other activities: disclosed no relevant relationships.
Anti-tumor suppressor antibodies and cancer
From September 2022, Kanduc reports on the findings from an in silico study analysing molecular mimicry and the related cross-reactive potential between SARS-CoV-2 spike glycoprotein (gp) antigen and human tumor-suppressor proteins. She concludes with warnings of a post COVID-19 “cancer epidemics worldwide” and recommends intensification of clinical surveillance in oncology and to undertake rigid cancer prevention actions, including healthy lifestyle, continuous controls and other actions.
“Medical Definition of Tumor suppressor gene. Tumor suppressor gene: A protective gene that normally limits the growth of tumors. When a tumor suppressor gene is mutated (altered), it may fail to keep a cancer from growing.61”
“A tumor suppressor gene (TSG), or anti-oncogene, is a gene that regulates a cell during cell division and replication.[1] If the cell grows uncontrollably, it will result in cancer. When a tumor suppressor gene is mutated, it results in a loss or reduction in its function. In combination with other genetic mutations, this could allow the cell to grow abnormally. The loss of function for these genes may be even more significant in the development of human cancers, compared to the activation of oncogenes.[2]
TSGs can be grouped into the following categories: caretaker genes, gatekeeper genes, and more recently landscaper genes. Caretaker genes ensure stability of the genome via DNA repair and subsequently when mutated allow mutations to accumulate.[3] Meanwhile, gatekeeper genes directly regulate cell growth by either inhibiting cell cycle progression or inducing apoptosis.[3] Lastly landscaper genes regulate growth by contributing to the surrounding environment, when mutated can cause an environment that promotes unregulated proliferation.[4] The classification schemes are evolving as medical advances are being made from fields including molecular biology, genetics, and epigenetics.”
“Unlike oncogenes, tumor suppressor genes generally follow the two-hit hypothesis, which states both alleles that code for a particular protein must be affected before an effect is manifested.[7] If only one allele for the gene is damaged, the other can still produce enough of the correct protein to retain the appropriate function. In other words, mutant tumor suppressor alleles are usually recessive, whereas mutant oncogene alleles are typically dominant.62”
The last point is important, it is the effective expression of the protein that is the key to efficacy. Additionally, you need a healthy varied T-cell response to target any cancer cells that escape the tumor suppressors.63 These can also be inhibited by spike protein via multiple pathways (see Substack posts from December ‘21 64).
Pathogenic priming is proposed as a mechanism, including by previous exposure to non-COVID19 bacteria with hexapeptides expressing molecular mimicry.
Clinical, multiple anecdotal accounts and Defense Medical Epidemiology Database (DMED) data65 is now presenting clear signals of a multifold increase in incidence of various cancer types, many of which are reportedly aggressive type 4 recurrences.
Abstract
Background and Objectives Whether exposure to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) may predispose to the risk of cancer in individuals with no prior cancers is a crucial question that remains unclear. To confirm/refute possible relationships between exposure to the virus and ex novo insurgence of tumors, this study analyzed molecular mimicry and the related cross-reactive potential between SARS-CoV-2 spike glycoprotein (gp) antigen and human tumor-suppressor proteins.
Materials and Methods Tumor-associated proteins were retrieved from UniProt database and analyzed for pentapeptide sharing with SARS-CoV-2 spike gp by using publicly available databases.
Results An impressively high level of molecular mimicry exists between SARS-CoV-2 spike gp and tumor-associated proteins. Numerically, 294 tumor-suppressor proteins share 308 pentapeptides with the viral antigen. Crucially, the shared peptides have a relevant immunologic potential by repeatedly occurring in experimentally validated epitopes. Such immunologic potential is of further relevancy in that most of the shared peptides are also present in infectious pathogens to which, in general, human population has already been exposed, thus indicating the possibility of immunologic imprint phenomena.
Conclusion This article described a vast peptide overlap between SARS-CoV-2 spike gp and tumor-suppressor proteins, and supports autoimmune cross-reactivity as a potential mechanism underlying prospective cancer insurgence following exposure to SARS-CoV-2. Clinically, the findings call for close surveillance of tumor sequelae that possibly could result from the current coronavirus pandemic.
Keywords: SARS-CoV-2 spike gp, tumor-suppressor proteins, molecular mimicry, cross-reactivity, long COVID, cancer epidemic
Moreover, and of special importance, it was noted that the viral versus human peptide sharing also involved human proteins related to pleuropulmonary blastoma, non-small cell lung cancer, breast invasive ductal carcinoma, multiple human cancers, tumor predisposition syndrome, and mesothelioma, inter alia. That is, the data suggested the possibility that morbidity/mortality increases in various tumors might represent long-term sequelae following exposure to SARS-CoV-2 (Kanduc 22 and pertinent references therein).
Hence, this study was undertaken to further explore the relationship between SARS-CoV-2 infection/active immunization and carcinogenesis, and specifically focused on the amino acid (aa) sequence identities between SARS-CoV-2 spike glycoprotein (gp) and tumor-suppressor human proteins. Analyses revealed a vast peptide sharing potentially able to generate pathogenic autoantibodies via cross-reactivity and immunologic imprinting phenomena, thus possibly leading to or enhancing the onset of a wide spectrum of cancer diseases.
Results and Discussion
Searching UniProt database for tumor-suppressor proteins produced 782 protein entries (in)directly related to tumor-suppressor activity and listed in Supplementary Table S1 (available in online version only). Of the 782 proteins, 294 have pentapeptides in common with the spike gp, in a total of 308 occurrences (in all, 462, including multiple occurrences). These numbers certify the existence of an impressive, unexpected level of molecular mimicry between the viral antigen and the cancer-related human proteins.
Table 1 shows data relative to a representative sample of 19 tumor-suppressor proteins and documents that the peptide commonality with the viral antigen amounts to 29 pentapeptides. From a pathological perspective, Table 1 clearly illustrates that even hitting only 19 out of the 294 tumor-suppressor proteins described in Supplementary Table S2 (available in online version only) might equate to induce or enhance carcinogenesis in almost all of the human organs, from brain and liver to lung and bones. Examples of the cancers that might be evoked/potentiated by exposure to SARS-CoV-2 in the next future are T cell acute lymphoblastic leukemia, oligodendrogliomas, breast/ovarian cancers, sarcoma, malignant mesothelioma, B cell chronic lymphocytic leukemia, and non-small cell lung carcinoma, among the others.
Immunologic Potential of the Peptide Sharing between SARS-CoV-2 Spike gp and Tumor-Suppressor Proteins
The gloomy outlook hinted at by the findings described in Table 1 becomes all the more likely in light of the high immunologic potential of the shared peptides. De facto, investigation of IEDB shows that the 29 pentapeptides shared by the spike gp antigen and the 19 tumor-suppressor proteins ( Table 1 ) occur and recur in 150 epitopes derived from SARS-CoV-2 that have been experimentally validated and are cataloged as immunoreactive ( Table 2 ).
In essence, Table 2 factually supports the possibility that cross-reactions can be triggered by SARS-CoV-2 infection/active immunization and hit human proteins related to carcinogenesis. Very much this conclusion applies when considering that the extent of the potential immunologic cross-reactivity as well as the spectrum of potentially inducible tumors may be exponentially higher in light of the fact that Tables 1 and refer to the peptide commonality involving only a tiny part (19 out of 294) of the human proteins that—if altered—may lead to cancer.
What amounts to pathogenic priming by previous exposure to certain microbes:
Potential Immunologic Imprint
The 29 pentapeptides common to SARS-CoV-2 spike gp and tumor-suppressor proteins ( Table 1 ) are not only present in immunoreactive epitopes ( Table 2 ) but, in addition, almost all of them (24 out of 29) are also present in microbial organisms such as Bordetella pertussis , C. diphtheriae , C. tetani , H. influenzae , and N. meningitides ( Table 3 ). That is, most of the shared peptides are also present in pathogens that an individual possibly encountered during his life because of infections and/or vaccinal routes.
Such interpathogen peptide commonality introduces the immunologic memory as a factor capable of enhancing the extent of the immune cross-reactive response against the tumor-suppressor proteins. That is, as already described since 1947, 4849 the immune system does not induce ex novo primary responses toward a recent infection. Rather, the immune system recalls, amplifies, and intensifies preexisting memory responses toward past infections. In this way, what should have been a primary response to a recent infection is transformed into an anamnestic, secondary, and magnified response to past infections. Simply put, as already discussed in previous reports, 505152535455 the early history of the individual's infections/vaccinations dictates the immune outcomes of any successive infections/vaccinations.
The original priming pathogenic bacterium has gone, we are now largely immune to it and any recurring auto-immune response is attenuated below our tolerance to cope with.
But if a strong immune response is generated by shared spike protein hexapeptides without the original pathogen as a target (eg due to “vaccination” or ”boosting”), or due to repeated COVID-19 infections with escaped variants, then non-neutralising autoantibody levels can surge, remain elevated for months and may be redirected to other homologous targets as discussed in the rest of this review, including the tumour suppressor proteins:
…following exposure to SARS-CoV-2 by infection or vaccination, the expected primary response to the virus can turn into a secondary response to previously encountered pathogens against which the immune system already reacted and of which has stored an immunologic memory, that is, the microbial organisms reported in Table 3 . However, the previously encountered pathogens are no more present in the human organism, so that the anamnestic immune response triggered by the exposure to SARS-CoV-2 by infection or vaccination ends to divert onto available immune determinants that, in the present case, are the common determinants present in the tumor-suppressor human proteins. Pathologically, one has to consider that usually an anamnestic secondary immune response is characterized by high avidity and high affinity, besides being quantitatively relevant. Therefore, as a final result, exposure to SARS-CoV-2 by infection and/or vaccination can trigger immediate and violent cross-reactive attacks against the proteins that protect the human being from carcinogenesis.
The author has some sobering advice in their conclusion, which appears to be quite prescient as the data comes in. In this regard, as this was an in silico study without in vitro clinical data, she recommends intensified clinical surveillance in oncology, rigid cancer prevention actions and a coordinated public health response to cope with the expected increase in incidence:
Conclusion
The findings described in Tables 1 to to33 and Supplementary Table S2 (available in online version only) indicate that molecular mimicry and cross-reactivity between peptides common to SARS-CoV-2 and tumor-related proteins might cause/contribute to cancer epidemics worldwide in the next future.The potential cancer risk might be enhanced by immunologic imprinting phenomena, given the fact that the comparative analyses shown in Table 3 indicate the possibility that a preexisting immune response to previously encountered pathogens could be magnified and intensified following SARS-CoV-2 infection/active immunization. These data are disturbing and invite to immediately intensify clinical surveillance in oncology and to undertake rigid cancer prevention actions, including healthy lifestyle and continuous controls. It will be vital to formulate/implement actions that contemplate fast and safe procedures for clinical trials, development of specific and reliable tumor markers for diagnosis, accurate follow-up of treatments, and, administratively, medical health records, detailed registries, biobanks, health surveys, and coordinated observational studies. Never before do all the recommendations of the European plan for the fight against cancer appear current and necessary. 58 De facto, tumors appear to be the predominant pathologies that will populate the post pandemic long COVID-19.
No funding was received and no conflicts of interest were declared.
Cancer risk, stratified by age
To further analyse the risk of cancer stratified by age we can refer to data from meta analysis of radiotherapy patients and atomic bomb survivors. Blood cancers tend to precede solid cancers by several years. And recurrences of older cancers previously in remission may precede these time scales further, dependent on tumor histology and epigenetics. From Cobb et al (1959)66:
Abstract
1. The incubation period of radiation-induced leukemia in adults is estimated to be about 5 years with 90 per cent of the cases occurring less than 10 years after exposure.
2. Assuming genesis during gestation, there is a somewhat shorter incubation period for children.
3. If one is willing to assume that the incubation period of leukemia induced by other means is approximately the same, there is now plain indication to search for other causes of leukemia up to 10 years before onset in adults, and during gestation or the first few weeks of postnatal life in the case of children.
4. This approach to the estimation of the incubation period should prove profitable in other malignant diseases.
In context of the above we have a very useful study by Shuryak et al (2010): Cancer Risks After Radiation Exposure in Middle Age67.
For newborns and infants exposed to cancer initiating agents and promotors the risk increases exponentially. This is to be expected as the immune system is still naive and, due to rapid cell growth, any mutated cancer cells will also form a larger percentage of their tissue mass and undergo rapid expansion.
The very young patient would also lack self awareness or communication skills of course, making diagnosis all the more challenging. This is yet another reason to exercise extreme caution and to conduct long term clinical trials (10 years +) with full risk/benefit analysis before considering administering such agents to children.
Initiation of even non cancer initiating autoimmune disorders at such an early stage in their development could also have devastating consequences going forwards, but with both the results may not be symptomatic until after some considerable time post exposure.
With spike protein, although ionising radiation is not the initiator or the promotor, it activates similar pathways involving reactive oxygen species generation, damage to mitochondrial DNA, bystander effects and so on as discussed in other Substacks and as such can act as initiator and promotor in susceptible individuals.
Further clinical validation of the comparisons would be valuable as there will be some differences in pathology but the principle of age related risk should be common to both due to immunosenescence of old age.
Abstract
Background
Epidemiological data show that radiation exposure during childhood is associated with larger cancer risks compared with exposure at older ages. For exposures in adulthood, however, the relative risks of radiation-induced cancer in Japanese atomic bomb survivors generally do not decrease monotonically with increasing age of adult exposure. These observations are inconsistent with most standard models of radiation-induced cancer, which predict that relative risks decrease monotonically with increasing age at exposure, at all ages.
Methods
We analyzed observed cancer risk patterns as a function of age at exposure in Japanese atomic bomb survivors by using a biologically based quantitative model of radiation carcinogenesis that incorporates both radiation induction of premalignant cells (initiation) and radiation-induced promotion of premalignant damage. This approach emphasizes the kinetics of radiation-induced initiation and promotion, and tracks the yields of premalignant cells before, during, shortly after, and long after radiation exposure.
Results
Radiation risks after exposure in younger individuals are dominated by initiation processes, whereas radiation risks after exposure at later ages are more influenced by promotion of preexisting premalignant cells. Thus, the cancer site–dependent balance between initiation and promotion determines the dependence of cancer risk on age at radiation exposure. For example, in terms of radiation induction of premalignant cells, a quantitative measure of the relative contribution of initiation vs promotion is 10-fold larger for breast cancer than for lung cancer. Reflecting this difference, radiation-induced breast cancer risks decrease with age at exposure at all ages, whereas radiation-induced lung cancer risks do not.
Conclusion
For radiation exposure in middle age, most radiation-induced cancer risks do not, as often assumed, decrease with increasing age at exposure. This observation suggests that promotional processes in radiation carcinogenesis become increasingly important as the age at exposure increases. Radiation-induced cancer risks after exposure in middle age may be up to twice as high as previously estimated, which could have implications for occupational exposure and radiological imaging.
Excess relative risks (ERRs) per Gy for cancer incidence in Japanese atomic bomb survivors as a function of age at radiation exposure. ERRs were estimated at an attained age of 80 years and sex averaged, except for female breast cancer. Solid cancers refers to all primary malignant tumors excluding hematopoietic cancers. The data points are derived from Walsh (5) and Little (6) and the error bars represent 90% confidence intervals.
Schematic illustrating the dominant factors determining the variation in radiation-induced cancer risk with age at exposure. Jagged arrows indicate different times of radiation exposure, and the solid circles represent risks at a given attained age (eg, 80 years). A) Excess risk per year due to radiation initiation; for an exposure at a younger age, initiated cells have longer to exploit their growth advantage over normal cells. B) Excess risk per year due to radiation promotion; people irradiated at older ages, when there are more premalignant cells for promotion to act upon, are expected to have larger promotion-driven risks. C) Excess lifetime risks due to radiation-induced initiation and promotion. Initiation and promotion result in very different variations in cancer risk as a function of age at exposure; the downturn in excess lifetime risk shown in (C) for very old ages at exposure is due mainly to competing risks.
Infertility
More research into potential autoimmune mediated infertility.
Dotan et al published a paper in 2021 with their findings that SARS-CoV-2 spike glycoprotein was found to share 41 minimal immune determinants (pentapeptides) with 27 human proteins that relate to oogenesis, uterine receptivity, decidualization, and placentation68. 23 of the 27 shared pentapeptides are also present in SARS-CoV-2 spike glycoprotein-derived epitopes that have been experimentally validated as immunoreactive. They caution this may lead to reproductive dysfunction, recommend increased vigilence and in-depth experimental studies.
Oogenesis: the production or development of an ovum.
Uterine receptivity: the capability of the uterus to allow an embryo to implant.
Decidualization: a process that results in significant changes to cells of the endometrium in preparation for, and during, pregnancy. This includes morphological and functional changes (the decidual reaction) to endometrial stromal cells (ESCs), the presence of decidual white blood cells (leukocytes), and vascular changes to maternal arteries. The sum of these changes results in the endometrium changing into a structure called the decidua. In humans, the decidua is shed during childbirth.69
Placentation: the formation or arrangement of a placenta or placentae in a woman's or female animal's uterus.
Abstract
Introduction: Oogenesis, the process of egg production by the ovary, involves a complex differentiation program leading to the production of functional oocytes. This process comprises a sequential pathway of steps that are finely regulated. The question related to SARS-CoV-2 infection and fertility has been evoked for several reasons, including the mechanism of molecular mimicry, which may contribute to female infertility by leading to the generation of deleterious autoantibodies, possibly contributing to the onset of an autoimmune disease in infected patients.
Objective: The immunological potential of the peptides shared between SARS-CoV-2 spike glycoprotein and oogenesis-related proteins; Thus we planned a systematic study to improve our understanding of the possible effects of SARS-CoV-2 infection on female fertility using the angle of molecular mimicry as a starting point.
Methods: A library of 82 human proteins linked to oogenesis was assembled at random from UniProtKB database using oogenesis, uterine receptivity, decidualization, and placentation as a key words. For the analyses, an artificial polyprotein was built by joining the 82 a sequences of the oogenesis-associated proteins. These were analyzed by searching the Immune Epitope DataBase for immunoreactive SARS-CoV-2 spike glycoprotein epitopes hosting the shared pentapeptides.
Results: SARS-CoV-2 spike glycoprotein was found to share 41 minimal immune determinants, that is, pentapeptides, with 27 human proteins that relate to oogenesis, uterine receptivity, decidualization, and placentation. All the shared pentapeptides that we identified, with the exception of four, are also present in SARS-CoV-2 spike glycoprotein-derived epitopes that have been experimentally validated as immunoreactive.
…Citing only a few, we can list here the loss of germ cells, severe reduction in testis and ovary size, alteration in male sex determination, sex reversal, alteration of folliculogenesis, alteration of the balance of the sexually dimorphic gene expression, reduced fertility, alterations of puberty with precocious puberty, absence of or incomplete sexual maturation, dysfunction of reproductive function, non-obstructive azoospermia and premature ovarian insufficiency.
…Although the present data warrant in-depth experimental studies, especially by testing large series of sera collected from COVID-19-ill patients in dedicated arrays for human proteins related to oogenesis, they encourage us to be vigilant in the future on issues of possible infertility in patients who have been infected by SARS-CoV-2. It should be emphasized that the molecular mimicry we found does not indicate female reproductive dysfunction in COVID-19 patients. Nevertheless, our findings suggest potential cross-reactivity between the homologous peptides that may result in the development of autoantibodies and new-onset of related autoimmune manifestations. Thus, in our perspective, detecting such autoantibodies should be attempted.
The authors declared no conflict of interest.
Guillain-Barré syndrome
Autoimmune induced Guillain-Barré syndrome discussed by Marinos C. Dalakas in 202070.
“Sialic acid (N-acetylneuraminic acid, Neu5Ac) is recognized as a “self” marker by major serum protein complement factor H and shows reduced interaction with the innate immune system via sialic acid-binding immunoglobulin-like lectin (Siglec), which is known as one of the significant regulators of phagocytic evasion.”
The implication being that once the neuron is no longer immune privileged as “self” due to spike protein binding it becomes liable to autoimmune attack:
Abstract
Objective To present the COVID-19–associated GBS, the prototypic viral-triggered autoimmune disease, in the context of other emerging COVID-19–triggered autoimmunities, and discuss potential concerns with ongoing neuroimmunotherapies.
Methods Eleven GBS cases in four key COVID-19 hotspots are discussed regarding presenting symptoms, response to therapies and cross-reactivity of COVID spike proteins with nerve glycolipids. Emerging cases of COVID-19–triggered autoimmune necrotizing myositis (NAM) and encephalopathies are also reviewed in the context of viral invasion, autoimmunity and ongoing immunotherapies.
Results Collective data indicate that in this pandemic any patient presenting with an acute paralytic disease-like GBS, encephalomyelitis or myositis-even without systemic symptoms, may represent the first manifestation of COVID-19. Anosmia, ageusia, other cranial neuropathies and lymphocytopenia are red flags enhancing early diagnostic suspicion. In Miller-Fisher Syndrome, ganglioside antibodies against GD1b, instead of QG1b, were found; because the COVID-19 spike protein also binds to sialic acid-containing glycoproteins for cell-entry and anti-GD1b antibodies typically cause ataxic neuropathy, cross-reactivity between COVID-19–bearing gangliosides and peripheral nerve glycolipids was addressed. Elevated Creatine Kinase (>10,000) is reported in 10% of COVID-19–infected patients; two such patients presented with painful muscle weakness responding to IVIg indicating that COVID-19–triggered NAM is an overlooked entity. Cases of acute necrotizing brainstem encephalitis, cranial neuropathies with leptomeningeal enhancement, and tumefactive postgadolinium-enhanced demyelinating lesions are now emerging with the need to explore neuroinvasion and autoimmunity. Concerns for modifications-if any-of chronic immunotherapies with steroids, mycophenolate, azathioprine, IVIg, and anti-B-cell agents were addressed; the role of complement in innate immunity to viral responses and anti-complement therapeutics (i.e. eculizumab) were reviewed.
Conclusions Emerging data indicate that COVID-19 can trigger not only GBS but other autoimmune neurological diseases necessitating vigilance for early diagnosis and therapy initiation. Although COVID-19 infection, like most other viruses, can potentially worsen patients with pre-existing autoimmunity, there is no evidence that patients with autoimmune neurological diseases stable on common immunotherapies are facing increased risks of infection.
Disclosure
M. Dalakas is an associate editor for Neurology: Neuroimmunology & Neuroinflammation. Disclosures available: Neurology.org/NN.
Brainstem-related respiratory failure and other pathologies
Mathew et al (2022) published this study, an “immunoinformatics prediction of potential immunodominant epitopes from human coronaviruses and association with autoimmunity”71. To avoid repetition of findings from previous studies I extract some interesting comments:
A recent study has identified shared antigenic epitopes between human molecular chaperons and SARS-CoV-2, with a potential role of inducing autoimmunity against endothelial cells using molecular mimicry (Marino et al. 2020). Similarly, it has been proposed that brainstem-related respiratory failure in COVID-19 patients may take place as a result of molecular mimicry between SARS-CoV-2 and neuronal proteins (Lucchese and Flöel 2020).
The IEDB analysis revealed SARS-CoV-2 68.49% of conserved SARS-CoV-2 peptides (50/73) were shown to bind to HLA class I molecules (HLA A, B, and C) with variable affinity, possibly inducing CD8 + and CD4 + T-cell responses (Anderson et al. 2020). The majority of HLA types were associated with autoimmune diseases and hyper-inflammatory conditions, such asMS, ankylosing spondylitis, PGA, SLE, T1D, and autoimmune vitiligo.
Previous studies have linked autoimmune conditions to other viruses. An interaction has been observed between anti-EBV (Epstein-Barr Virus) antibodies and HLA-DRB1*15 increasing the risk for MS (Sundqvist et al. 2012). Additionally, a strong connection has been established between HLA-DRB1*1301 (a marker for pediatric autoimmune hepatitis) and protracted forms of HAV (hepatitis A virus) infection (Fainboim et al. 2001). In terms of SARS-CoV-2, the immunogenic symptoms observed in COVID-19 patients are relatively similar to those observed in autoimmune conditions (Rodríguez et al. 2020).
Recent studies suggested a correlation between COVID-19 and an autoimmune conditions in kids, known as Kawasaki disease (Galeotti and Bayry 2020). A proposed mechanism (hypothesis) involves the role of TNF-α (Amirfakhryan 2020). Since children who are susceptible to KD exhibit genetically downregulated ACE2 receptor, SARS-CoV-2 infection will further downregulate ACE2 expression by TNF-α, leading to Kawasaki-like disease (Amirfakhryan 2020). Interestingly, 70% of SARS-CoV-2 predicted peptides bind to HLA types associated with other viral infections (e.g., HIV-1 and chickenpox susceptibility). This raises the questions of whether people previously exposed to either virus could have CD8 + and CD4 + T-cell responses against SARS-CoV-2.
Anti-DNA and anti-phosphatidylserine antibodies
The presence of anti-DNA and anti-phosphatidylserine antibodies were found to predict the development of severe COVID-19 in this study by Gomes et al (2021)72.
High levels of autoimmune antibodies are observed in COVID-19 patients but their specific contribution to disease severity and clinical manifestations remains poorly understood. We performed a retrospective study of 115 COVID-19 hospitalized patients with different degrees of severity to analyze the generation of autoimmune antibodies to common antigens: a lysate of erythrocytes, the lipid phosphatidylserine (PS) and DNA. High levels of IgG autoantibodies against erythrocyte lysates were observed in a large percentage (up to 36%) of patients. Anti-DNA and anti-PS antibodies determined upon hospital admission correlated strongly with later development of severe disease, showing a positive predictive value of 85.7% and 92.8%, respectively. Patients with positive values for at least one of the two autoantibodies accounted for 24% of total severe cases. Statistical analysis identified strong correlations between anti-DNA antibodies and markers of cell injury, coagulation, neutrophil levels and erythrocyte size. Anti-DNA and anti-PS autoantibodies may play an important role in the pathogenesis of COVID-19 and could be developed as predictive biomarkers for disease severity and specific clinical manifestations.
Central tolerance
A study using a murine model of virus induced autoimmune disorders and the difficulties presented to diagnosis (2022)74. Due to the broad antibody responses found, central tolerance is considered more important than just molecular mimicry.
It would appear from the assembled literature that, according to genetic and epigenetic predisposition, each individual has a level of tolerance to autoimmune antibodies, a threshold that if crossed leads to symptomatic disease after a time lag that may easily stretch to several years.
There must be caution exercised in that repeat boosting and/or consequential re-infections may push many individuals past this threshold, as per the warning at the start of this literature review:
Autoimmune diseases such as rheumatoid arthritis and Type 1 diabetes are thought to arise when people with a genetic susceptibility to autoimmunity encounter something in the environment that triggers their immune systems to attack their own bodies. Scientists have made progress in identifying genetic factors that put people at risk, but the environmental triggers have proven more elusive.
Researchers at Washington University School of Medicine in St. Louis have discovered that a viral infection can set a destructive process in motion, culminating in autoimmunity long after the infection has resolved. The researchers investigated the impact of viral infection on T cells, a group of immune cells that play a key role in many autoimmune conditions. In the study, which was conducted in mice, the researchers showed that murine roseolovirus infects the thymus -- the organ where self-destructive T cells are identified and eliminated -- and disrupts the screening process in the organ. Months after infection, the mice develop an autoimmune disease of the stomach driven by self-destructive T cells.
The study, published Feb. 28 in the Journal of Experimental Medicine, describes a previously unknown way a virus can trigger autoimmunity. Further, it suggests that human roseoloviruses, close relatives of murine roseolovirus, warrant investigation as possible causes of autoimmunity in people.
"It is very hard to find the culprit of a crime that was never even at the scene of the crime," said senior author Wayne M. Yokoyama, MD, the Sam J. Levin and Audrey Loew Levin Professor of Arthritis Research. "As clinicians, we often look directly in the diseased tissue, and if we find no virus we conclude that the disease was not caused by a virus. But here we have a situation in which a virus is doing its damage someplace else entirely. This virus goes to the thymus, which is where T cells undergo a process to select those cells useful for immune defense but also get rid of T cells that are too likely to damage the body's own tissues. And what we find is that this whole process, which is called central tolerance, is affected. T cells that shouldn't leave the thymus get out, and they manifest months later in the stomach, causing an autoimmune disease in a location that was never infected with the virus."
Human and mouse roseoloviruses are members of the herpesvirus family. In people, roseoloviruses cause roseola, a mild childhood illness that involves a few days of fever and rash. Most people have been infected with at least one roseolovirus by the time they start kindergarten. Like other herpesviruses, roseoloviruses cause lifelong infections, although the virus goes dormant and rarely causes symptoms after the initial infection.
Scientists have long suspected that roseoloviruses may be linked to autoimmunity. But the ubiquity of the viruses makes investigating any such connection difficult. It is hard to look for differences between infected and uninfected people when nearly everyone is infected early in life.
Instead, Yokoyama, first author Tarin Bigley, MD, PhD, a fellow in pediatric rheumatology, and colleagues studied murine roseolovirus, a recently discovered virus that infects the thymus and T cells of mice in the wild. The researchers infected newborn mice with the virus. Twelve weeks later, all of the mice had developed autoimmune gastritis, or stomach inflammation, though there were no signs of the virus in their stomachs. If the virus was promptly eliminated with antiviral drug treatment in the first few days, while it was still actively replicating, the mice did not develop gastritis three months later. If, however, the researchers waited to give an antiviral until the mice were 8 weeks old -- after the active infection had resolved but before the mice showed signs of stomach problems -- the drug did no good at all; the mice still went on to develop gastritis a few weeks later.
Scientists already knew that viral infection can lead to autoimmunity if some of the virus's proteins happen to resemble normal human proteins. Antibodies meant to target the virus end up also reacting with normal human cells. The researchers found that the mice with gastritis had developed antibodies against proteins on stomach cells. But they also had developed antibodies against a wide array of normal proteins associated with other autoimmune conditions. In addition, they had many T cells that targeted the body's own normal proteins, and other changes to the T cell population that biased the immune system toward autoimmunity.
"We don't think the autoimmune gastritis is the result of molecular mimicry because we observed such a broad autoantibody response," Bigley said. "The observation that infected mice produced diverse autoantibodies, in addition to the anti-stomach autoantibodies, suggested thatmurine roseolovirus infection early in life was inducing a wide-ranging defect in the body's ability to avoid targeting its own proteins. This is why we focused our studies on the impact of infection on central tolerance rather than molecular mimicry."
The next step is to investigate whether a similar process occurs in people.
“Universal” influenza vaccines and related autoimmune disorders
A 2022 published paper by Labombarde et al found an association between “universal” influenza vaccines with a wide range of non-conserved epitopes and the induction of autoimmune disorders75. It is reasonable to expect the same outcome from any attempts to develop universal coronavirus vaccines too. A worsening of symptoms of pre-existing autoimmune conditions is again highlighted:
Abstract
Infection and vaccination repeatedly expose individuals to antigens that are conserved between influenza virus subtypes. Nevertheless, antibodies recognizing variable influenza epitopes greatly outnumber antibodies reactive against conserved epitopes. Elucidating factors contributing to the paucity of broadly reactive influenza antibodies remains a major obstacle for developing a universal influenza vaccine. Here, we report that inducing broadly reactive influenza antibodies increases autoreactive antibodies in humans and mice and exacerbates disease in four distinct models of autoimmune disease. Importantly, transferring broadly reactive influenza antibodies augments disease in the presence of inflammation or autoimmune susceptibility. Further, broadly reactive influenza antibodies spontaneously arise in mice with defects in B cell tolerance. Together, these data suggest that self-tolerance mechanisms limit the prevalence of broadly reactive influenza antibodies, which can exacerbate disease in the context of additional risk factors.
Gamma interferon induced autoimmunity, rheumatoid arthritis and bone destruction
A 2018 study by Tang et al discusses gamma interferon induced autoimmunity and bone destruction76.
Vaccination causes highly elevated levels of IFN-γ for a sustained period of time:
“Using an interferon-gamma release assay (IGRA) test, we aimed to monitor cellular post-vaccination immunity in healthy subjects vaccinated with BNT162b2 mRNA COVID-19 vaccine (Comirnaty). We tested 37 healthcare workers (mean age 54.3 years, range 28-72, 22 females, 15 males) following COVID-19 mRNA COVID-19 vaccine and 15 healthy unvaccinated native persons as control subjects using QuantiFERON SARS-CoV-2 RUO test, performed approximately 1 month after vaccination. We also measured virus-neutralizing antibodies. Thirty-one out of 37 tested subjects had significantly raised levels of SARS-CoV-2 specific IFNγ against SARS-CoV-2 Ag1 and Ag2 1 month following COVID-19 vaccination.77”
RA = rheumatoid arthritis. Osteoblasts build bone matrix, osteoclasts break it down:
Interferon-gamma seems to exert different effects in different stages of RA. In animal experiment, IFN-γ accelerates the onset and development of RA in the early stage. IFN-γ may promote autoimmunity and activate immune response, increasing the level of osteoclastic factors and leading to the development of RA and bone destruction. The indirect stimulating effect of IFN-γ on osteoclasts may be predominant in the early stage of RA. However, IFN-γ seems to have a protective role in RA in the effector phase. The activation of immune systems in the onset of RA can attract more monocytes and macrophages from blood and peripheral tissue into joints to cause massive amplification of osteoclast formation. IFN-γ reduces c-Fms and RANK to inhibit osteoclast formation. IFN-γ also induces TRAF6 degradation or downregulates NFATc1 to inhibit the RANK–RANKL pathway to prevent osteoclast differentiation. In patients with RA, most of studies show administration of IFN-γ is an effective therapy, but some patients fail to display an adequate response. The difference in the genetic and epigenetic factors, the duel effect of IFN-γ in osteoclastogenesis, disease severity, and rate of progression may be the reason for these contradictory results.
Anti-idiotype antibodies
With respect to syndromes like long-COVID, one concerning hypothesis is the generation of antibodies to antibodies (ie anti-idiotype or “Ab2” antibodies) that have similar pathogenicity as the original spike protein. As these are products of the immune system, production in response to homologous epitopes could continue indefinitely, at least until immune exhaustion occurs or memory B cell anergy78.
Chronic low-level BCR cross-linkage and a lack of sufficient costimulation are believed to result in B-cell anergy, whereas high BCR cross-linkage with costimulation leads to activation or without proper costimulation leads to clonal deletion. B cells of several types in humans have been demonstrated to be autoreactive and anergic (top). In addition, memory B cells (bottom) from patients with HIV have been shown to be “exhausted,” which is similar to anergy. B cells with a similar phenotype have also been found in other chronic infectious diseases including HCV8 and malaria.
The pathogenesis of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection is incompletely understood, with its effects on multiple organ systems1 and the syndrome of “long Covid” occurring long after the resolution of infection.2 The development of multiple efficacious vaccines has been critical in the control of the pandemic, but their efficacy has been limited by the appearance of viral variants, and the vaccines can be associated with rare off-target or toxic effects, including allergic reactions, myocarditis, and immune-mediated thrombosis and thrombocytopenia in some healthy adults. Many of these phenomena are likely to be immune-mediated.3 How can we understand this diversity in immune responses in different persons?
Figure 1.
Anti-idiotype Antibodies and SARS-CoV-2.
One way of thinking about the complexity of the immune response is through the lens of anti-idiotype immune responses. The Network Hypothesis, formulated in 1974 by Niels Jerne, described a mechanism by which the antibody responses to an antigen themselves induced downstream antibody responses against the antigen-specific antibody.4 Every antibody that is induced and specific for an antigen (termed “Ab1” antibody) has immunogenic regions, particularly in their variable-region antigen-binding domains, that are unique as a result of genetic recombination of immunoglobulin variable, diversity, and joining (VDJ) genes; VDJ recombination results in new and therefore immunogenic amino acid sequences called idiotopes, which are then capable of inducing specific antibodies against Ab1 antibodies as a form of down-regulation. A similar paradigm has been proposed for T cells. However, these regulatory immune responses are also capable of doing much more. The paratopes, or antigen-binding domains, of some of the resulting anti-idiotype (or “Ab2”) antibodies that are specific for Ab1 can structurally resemble that of the original antigens themselves. Thus, the Ab2 antigen-binding region can potentially represent an exact mirror image of the initial targeted antigen in the Ab1 response, and Ab2 antibodies have even been examined for potential use as a surrogate for the antigen in vaccine studies. However, as a result of this mimicry, Ab2 antibodies also have the potential to bind the same receptor that the original antigen was targeting (Figure 1). Ab2 antibodies binding to the original receptor on normal cells therefore have the potential to mediate profound effects on the cell that could result in pathologic changes, particularly in the long term — long after the original antigen itself has disappeared.
This aspect of regulation of immune-cell responses was postulated by Plotz in 1983 as a possible cause of autoimmunity arising after viral infection5 and has since been supported experimentally by direct transfer of anti-idiotype antibodies. Ab2 antibodies generated against the enterovirus coxsackievirus B3 in mice can bind myocyte antigens, resulting in autoimmune myocarditis,6 and anti-idiotype responses can act as acetylcholine receptor agonists, leading to myasthenia gravis symptoms in rabbits.7In addition, by displaying the mirror image of the viral antigen, Ab2 alone can even mimic the deleterious effects of the virus particle itself, as has been shown with bovine viral diarrhea virus antigen.8
For SARS-CoV-2 infection, attention centers on the spike (S) protein and its critical use of the angiotensin-converting–enzyme 2 (ACE2) receptor to gain entry into the cell. Given its critical role in regulating angiotensin responses, many physiological effects can be influenced by ACE2 engagement.9The S protein itself has a direct effect on suppressing ACE2 signaling by a variety of mechanisms and can also directly trigger toll-like receptors and induce inflammatory cytokines.10Anti-idiotype responses may affect ACE2 function, resulting in similar effects. However, preclinical and clinical assessments of antibody responses to SARS-CoV-2 vaccines have focused solely on Ab1 responses and virus-neutralizing efficacy. The delineation of potential anti-idiotype responses has inherent difficulties because of the polyclonal nature of responses, dynamic kinetics, and the concurrent presence of both Ab1 and Ab2 antibodies. Furthermore, ACE2 expression within cells and tissues can be variable. The different vaccine constructs (RNA, DNA, adenoviral, and protein) are also likely to have differential effects on Ab2 induction or in the mediation of vaccine effects that differ from responses to infection. Some off-target effects may not be directly linked to Ab2 responses. The association of thrombotic events with some SARS-CoV-2 vaccines in young women and the etiologic role of anti–platelet factor 4–polyanion antibodies may be the result of the adenoviral vector. However, the reported occurrence of myocarditis after vaccine administration bears striking similarities to the myocarditis associated with Ab2 antibodies induced after some viral infections.6 Ab2 antibodies could also mediate neurologic effects of SARS-CoV-2 infection or vaccines, given the expression of ACE2 on neuronal tissues, the specific neuropathologic effects of SARS-CoV-2 infection,11 and the similarity of these effects to Ab2-mediated neurologic effects observed in other viral models.
It would therefore be prudent to fully characterize all antibody and T-cell responses to the virus and the vaccines, including Ab2 responses over time. Using huACE2 transgenic mice and crossing them with strains that are predisposed to autoimmunity or other human pathologic conditions can also provide important insights. An understanding of potential Ab2 responses may also provide insights into Ab1 maintenance and efficacy and into the application of antibody-based therapeutic agents. However, much more basic science research is needed to determine the potential role idiotype-based immunoregulation of both humoral and cell-mediated responses may play both in antiviral efficacy and in unwanted side effects of both SARS-CoV-2 infection and the vaccines that protect us from it.
Diagnosis & Therapeutics
Identifying the trigger can be very challenging due to a myriad of downstream effects and time delays between exposure to the original antigen, generation of autoantibodies and finally presentation of any symptoms.
The Cleveland Clinic guidance to patients on diagnosis and a list some of the questions your healthcare provider might ask80:
How are autoimmune diseases diagnosed?
Diagnosing an autoimmune disease usually takes healthcare providers longer than it does to diagnose other diseases. This is because many autoimmune diseases have similar symptoms with each other and with other diseases. You can help your healthcare provider with the diagnosing process by bringing the following to your appointment:
A detailed list of any symptoms and how long you’ve had them.
A record of your family’s health history. Note if anyone in your family has an autoimmune disease.
In addition to interviewing you about your symptoms, your healthcare provider may do some blood tests to check for autoimmune diseases, including:
Antinuclear antibody test (ANA).
Complete blood count (CBC).
Erythrocyte sedimentation rate (ESR).
Specific symptoms combined with specific blood markers may prove that you have an autoimmune disease.
What medications are you taking?
What are your symptoms?
How severe are your symptoms?
Have you had to go to the emergency department because of your symptoms?
How long have you had these symptoms?
In what ways are your symptoms affecting your quality of life?
Is there anything that “triggers” your symptoms? Anything that makes them worse?
Is there a history of autoimmune diseases in your family?
Which autoimmune diseases run in your family?
What over-the-counter or alternative medicines have you tried, if any?
As for therapeutics, the challenge is in inhibiting pathogenic autoantibodies without suppressing the rest of the immune system at the same time. The problem with the frequently prescribed steroids is that long term use is contraindicated81:
A new study published in the journal PLOS Medicine found that glucocorticoids, a type of steroid medication, increase the risk of cardiovascular disease in some individuals.
Previous research had shown that the lowest doses of steroids did not impact cardiovascular risk. However, this recent study, published on December 3, concluded that cardiovascular risk nearly doubles in patients who take low-dose steroids and increases even further in patients who take higher doses over extended periods of time.
Researchers reviewed 87,794 medical records from the U.K. between 1998 and 2017. Patients in the analysis had received steroids for at least one of the following conditions: giant cell arteritis, polymyalgia rheumatica, inflammatory bowel disease, lupus, rheumatoid arthritis, or vasculitis. The average subject age was 56 years, and 34% were men.
Some of the cardiovascular events these patients experienced include:
Heart attack
Heart failure
Atrial fibrillation
Peripheral arterial disease
Stroke
Abdominal aortic aneurysm
However, on a positive note, a 2003 study by Bossù et al found that vaccination induced inhibition of interleukin 18 protected mice from a spontaneous lupus-like autoimmune disease82:
Abstract
The lupus-like autoimmune syndrome of MRL/Mp-Tnfrsf6lpr (lpr) mice is characterized by progressive lymphadenopathy and autoantibody production, leading to early death from renal failure. Activation of T helper lymphocytes is one of the events in the pathogenesis of the disease in these mice and likely in human systemic lupus erythematosus. Among T helper lymphocytedependent cytokines, IFN-γ plays a pivotal role in the abnormal cell activation and the fatal development of the lpr disease. IL-18, an inducer of IFN-γ in T lymphocytes and natural killer cells, may contribute to the disease because cells from lpr mice are hypersensitive to IL-18 and express high levels of IL-18. To assess the contribution of IL-18 to the pathogenesis in the animal model, in vivo inhibition of IL-18 was attempted. Young lpr mice were vaccinated against autologous IL-18 by repeated administration of a cDNA coding for the murine IL-18 precursor. Vaccinated mice produced autoantibodies to murine IL-18 and exhibited a significant reduction in spontaneous lymphoproliferation and IFN-γ production as well as less glomerulonephritis and renal damage. Moreover, mortality was significantly delayed in anti-IL-18-vaccinated mice. These studies support the concept that IL-18 plays a major role in the pathogenesis of the autoimmune syndrome of lpr mice and that a reduction in IL-18 activity could be a therapeutic strategy in autoimmune diseases.
Apart from Baicalin as discussed previously, I am also maintaining a list of therapeutics for multiple sclerosis (MS) and peripheral neuropathy (PN). When there are further developments in treating autoimmune disorders I will post them there or post a link to them:
Ready to dive deeper into the extracellular nightmare? - Lucky to talk with Dr. J Matthew Rhett:Look into gap junctions and the heart. Fine regulation of cell-cell interaction is needed to maintain synchronization of action potential propagation in the heart. Easy to see how expression of membrane-anchored spike could lead to sudden cardiac events.
It would appear from the balance of evidence presented, - results of the assembled literature and clinical reports, that an extreme risk to public health due to autoimmune diseases is not just a potential risk but one that is indeed being realised.
The full effects may not be apparent for many years, by which time options for effective treatment may well be limited, diagnosis a challenge and many tissues permanently damaged by then with a shortening of lifespan and extra demands placed on medical services the consequence.
I would strongly advise that the current generation of adenovirus vector and mRNA transfection agents have their authorisations reviewed immediately, not least pending lack of long term investigations into autoimmunity, pregnancy, child pathologies and extremely high rates of adverse events but also due to the availability of safe, proven antivirals such as those used in the FLCCC & Zelenko protocols.
Agrescit medendo, the cure is worse than the disease.
The last word must go to Rob Verkerk Ph.D (19th February 2021)83:
Molecular mimicry could come back to bite us
Before offering some concerns about the various environmental triggers that might be concealed in COVID vaccines, let’s look at Prof Shoenfeld’s main concerns about the active part of the vaccines — the antigen — typically part of the genetic sequence of the SARS-CoV-2 spike protein.
This concern is just as relevant when the synthetic antigen is shipped into the body inside another cell or vehicle (e.g. AstraZeneca, Novavax) or it’s been instructed to be produced by the muscle cells after they receive instructions from the mRNA in the Pfizer and Moderna vaccines.
Shoenfeld’s primary concern boils down to what’s called molecular mimicry. There are a number of genetic sequences that are identical both in the human genome and that of SARS-CoV-2 – with Shoenfeld and colleagues identifying 26.
The immunologists go on to draw particular attention to the identical sequences in a specific group of proteins found deep in the lungs (the site of ARDS/covid pneumonia), the alveolar surfactant proteins, and the glycoprotein of SARS-CoV-2. This is a concern Shoenfeld along with co-author Darja Kanduc, from the University of Bari, Italy, shared in a paper in Clinical Immunology published last June.
It’s why Shoenfeld and colleagues have been banging on the drum during the vaccine development phase last year, arguing that peptide sequences used in the new vaccines should be unique and not be common to ones found in the body.
For a predisposed individual, an adverse reaction to the vaccine, Shoenfeld and colleagues argue, could be enough for them to be tipped over the edge — into autoimmune disease. One of the most obvious signals for predisposition is to already have one of the over 100 autoimmune diseases that are charging through industrialized societies. Yet, with the father of autoimmunity sounding the warnings of autoimmune risks, there is scarcely a word of caution being uttered by governments rolling out the mass vaccination programs. Shame on them.
Conflict of Interest
The author has no conflict of interest to declare.
Thank you for reading DoorlessCarp’s Scientific Literature Review. This post is public so feel free to share it.
Alexander, P. Warning: coming many Americans, many people will die because of these COVID injections, many healthy children WILL die due to these shots; FDA, CDC, NIH, Moderna, & Pfizer secretly told me this, (2022),
Lyons-Weiler, J. Pathogenic priming likely contributes to serious and critical illness and mortality in COVID-19 via autoimmunity, Journal of Translational Autoimmunity, Volume 3, (2020), 100051, ISSN 2589-9090,
Adams Waldorf KM, Nelson JL. Autoimmune disease during pregnancy and the microchimerism legacy of pregnancy. Immunol Invest. 2008;37(5):631-44. doi: 10.1080/08820130802205886. PMID: 18716941; PMCID: PMC2709983.
Kanduc, D., Shoenfeld, Y. Molecular mimicry between SARS-CoV-2 spike glycoprotein and mammalian proteomes: implications for the vaccine. Immunol Res 68, 310–313 (2020). https://doi.org/10.1007/s12026-020-09152-6
Aristo, V. Vojdani, E & Kharrazian, D. Reaction of Human Monoclonal Antibodies to SARS-CoV-2 Proteins With Tissue Antigens: Implications for Autoimmune Diseases. Frontiers in Immunology, 11, (2021), DOI=10.3389/fimmu.2020.617089,
Talja I, Reimand T, Uibo O, Reimand K, Aun S, Talvik T, Janmey PA, Uibo R. Antibodies to neurofilaments. Ann N Y Acad Sci. 2009 Sep;1173:130-6. doi: 10.1111/j.1749-6632.2009.04624.x. PMID: 19758141.
Yano T, Yamada K, Kimura A, Takeshita T, Minohara M, Kira J, Senju S, Nishimura Y, Tanihara H. Autoimmunity against neurofilament protein and its possible association with HLA-DRB1*1502 allele in glaucoma. Immunol Lett. 2005 Sep 15;100(2):164-9. doi: 10.1016/j.imlet.2005.03.017. PMID: 16005081.
McLachlan SM, Rapoport B. Autoimmune response to the thyroid in humans: thyroid peroxidase--the common autoantigenic denominator. Int Rev Immunol. 2000;19(6):587-618. doi: 10.3109/08830180009088514. PMID: 11129117.
Takashi Nakamura, Hideyoshi Harashima. Dawn of lipid nanoparticles in lymph node targeting: Potential in cancer immunotherapy. Advanced Drug Delivery Reviews, Volume 167, 2020, Pages 78-88, ISSN 0169-409X,
Christopher A. Beaudoin, Arian R. Jamasb, Ali F. Alsulami, Liviu Copoiu, Andries J. van Tonder, Sharif Hala, Bridget P. Bannerman, Sherine E. Thomas, Sundeep Chaitanya Vedithi, Pedro H.M. Torres, Tom L. Blundell. Predicted structural mimicry of spike receptor-binding motifs from highly pathogenic human coronaviruses. Computational and Structural Biotechnology Journal, Volume 19, 2021, Pages 3938-3953, ISSN 2001-0370,
Moody R, Wilson KL, Boer JC, Holien JK, Flanagan KL, Jaworowski A and Plebanski M (2021) Predicted B Cell Epitopes Highlight the Potential for COVID-19 to Drive Self-Reactive Immunity. Front. Bioinform. 1:709533. doi: 10.3389/fbinf.2021.709533
Gerd Wallukat, Bettina Hohberger, Katrin Wenzel, Julia Fürst, Sarah Schulze-Rothe, Anne Wallukat, Anne-Sophie Hönicke, Johannes Müller. Functional autoantibodies against G-protein coupled receptors in patients with persistent Long-COVID-19 symptoms. Journal of Translational Autoimmunity, Volume 4, 2021, 100100, ISSN 2589-9090.
Wang H, Chen Q, Hu Y, et al. Pathogenic antibodies induced by spike proteins of COVID-19 and SARS-CoV viruses. Research Square; 2021. DOI: 10.21203/rs.3.rs-612103/v2.
Chen Y, Xu Z, Wang P, Li XM, Shuai ZW, Ye DQ, Pan HF. New-onset autoimmune phenomena post-COVID-19 vaccination. Immunology. 2022 Apr;165(4):386-401. doi: 10.1111/imm.13443. Epub 2022 Jan 7. PMID: 34957554.
Yang J, Yang X, Yang J, Li M. Baicalin ameliorates lupus autoimmunity by inhibiting differentiation of Tfh cells and inducing expansion of Tfr cells. Cell Death Dis. 2019 Feb 13;10(2):140. doi: 10.1038/s41419-019-1315-9. PMID: 30760702; PMCID: PMC6374440.
Zheng X, Wang P, Jia M, Li Q, Zhang A, Zhou Q. Baicalin Alleviates Thrombin-Induced Inflammation in Vascular Smooth Muscle Cells. Biomed Res Int. 2022 Jan 21;2022:5799308. doi: 10.1155/2022/5799308. PMID: 35097121; PMCID: PMC8799346.
Da X, Tie D, Ochi Y, Morita E. Baicalein protects normal human epidermal keratinocytes against bullous pemphigoid immunoglobulin G-induced alteration. J Dermatol Sci. 2019 Aug;95(2):84-87. doi: 10.1016/j.jdermsci.2019.06.010. Epub 2019 Jul 2. PMID: 31307861.
Li NL, Nie H, Yu QW, Zhang JY, Ma AL, Shen BH, Wang L, Bai J, Chen XH, Zhou T, Zhang DQ. Role of soluble Fas ligand in autoimmune diseases. World J Gastroenterol. 2004 Nov 1;10(21):3151-6. doi: 10.3748/wjg.v10.i21.3151. PMID: 15457562; PMCID: PMC4611260.
Oyama-Manabe N, Yabusaki S, Manabe O, Kato F, Kanno-Okada H, Kudo K. IgG4-related Cardiovascular Disease from the Aorta to the Coronary Arteries: Multidetector CT and PET/CT. Radiographics. 2018 Nov-Dec;38(7):1934-1948. doi: 10.1148/rg.2018180049. Epub 2018 Oct 5. PMID: 30289734.
Sidney Cobb, Martha Miller, Niel Wald. On the estimation of the incubation period in malignant disease: The brief exposure case, leukemia. Journal of Chronic Diseases, Volume 9, Issue 4, (1959), Pages 385-393, ISSN 0021-9681,
Shuryak I, Sachs RK, Brenner DJ. Cancer risks after radiation exposure in middle age. J Natl Cancer Inst. 2010 Nov 3;102(21):1628-36. doi: 10.1093/jnci/djq346. Epub 2010 Oct 25. PMID: 20975037; PMCID: PMC2970575.
Dotan A, Kanduc D, Muller S, Makatsariya A, Shoenfeld Y. Molecular mimicry between SARS-CoV-2 and the female reproductive system. Am J Reprod Immunol. 2021 Dec;86(6):e13494. doi: 10.1111/aji.13494. Epub 2021 Sep 17. PMID: 34407240; PMCID: PMC8420155.
Marinos C. Dalakas. Guillain-Barré syndrome: The first documented COVID-19–triggered autoimmune neurologic disease. More to come with myositis in the offing.
Mathew, S., Fakhroo, A.D., Smatti, M. et al.Immunoinformatics prediction of potential immunodominant epitopes from human coronaviruses and association with autoimmunity. Immunogenetics 74, 213–229 (2022). https://doi.org/10.1007/s00251-021-01250-5
Claudia Gomes, Marisol Zuniga, Kelly A Crotty, Kun Qian, Nubia Catalina Tovar, Lawrence Hsu Lin, Kimon V Argyropoulos, Robert Clancy, Peter Izmirly, Jill Buyon, David C Lee, Maria Fernanda Yasnot-Acosta, Huilin Li, Paolo Cotzia, Ana Rodriguez. Autoantibodies predict COVID-19 severity. Life Science Alliance Sep 2021, 4 (11) e202101180; DOI: 10.26508/lsa.202101180.
Khogeer H, Alfattani A, Al Kaff M, Al Shehri T, Khojah O, Owaidah T. Antiphosphatidylserine antibodies as diagnostic indicators of antiphospholipid syndrome. Lupus. 2015 Feb;24(2):186-90. doi: 10.1177/0961203314552462. Epub 2014 Sep 24. PMID: 25253571.
Washington University School of Medicine. "New way viruses trigger autoimmunity discovered: In mice, roseolovirus disrupts immune cells' process of learning self-recognition." ScienceDaily. ScienceDaily, 28 February 2022.
Labombarde JG, Pillai MR, Wehenkel M, Lin CY, Keating R, Brown SA, Crawford JC, Brice DC, Castellaw AH, Mandarano AH, Guy CS, Mejia JR, Lewis CD, Chang TC, Oshansky CM, Wong SS, Webby RJ, Yan M, Li QZ, Marion TN, Thomas PG, McGargill MA. Induction of broadly reactive influenza antibodies increases susceptibility to autoimmunity. Cell Rep. 2022 Mar 8;38(10):110482. doi: 10.1016/j.celrep.2022.110482. PMID: 35263574; PMCID: PMC9036619.
Thank you for putting all of this together. I research a lot, but I have a finite ability to understand subjects to this level of detail.
I noticed there were a lot of studies published prior to the vaccines showing the spike protein had an unprecedented degree of molecular mimicry with human tissue and various complaints to regulators sent out. Given that the vaccines were designed to have these antigens then present on the surface of cells, it became quite clear this would be a very bad idea and a recipe for autoimmunity.
In Pfizer's leaked EMA (europe's FDA) documents, they opted out of performing the required autoimmunity studies, which I took as a tacit admission it was known the vaccines would cause autoimmunity.
At this point in time, I feel the spike protein was developed to cause as many chronic long term diseases as possible in the human population.




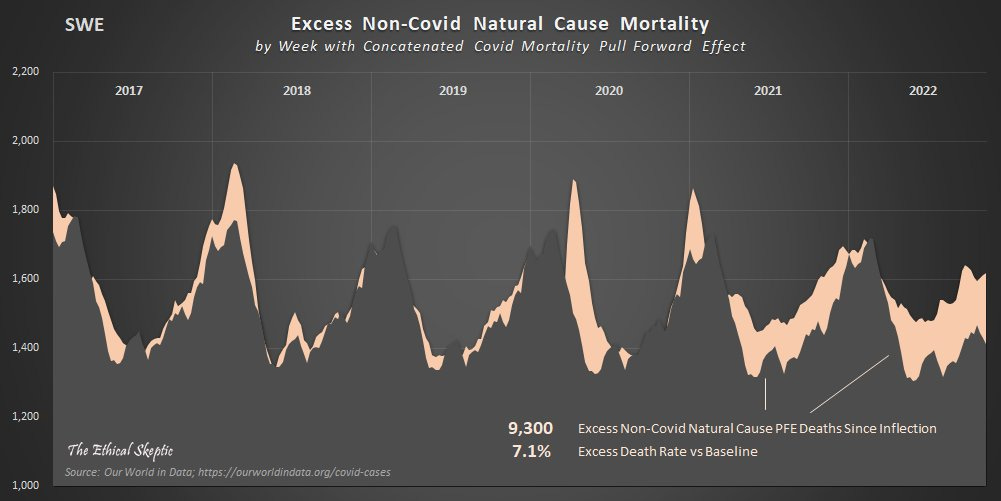


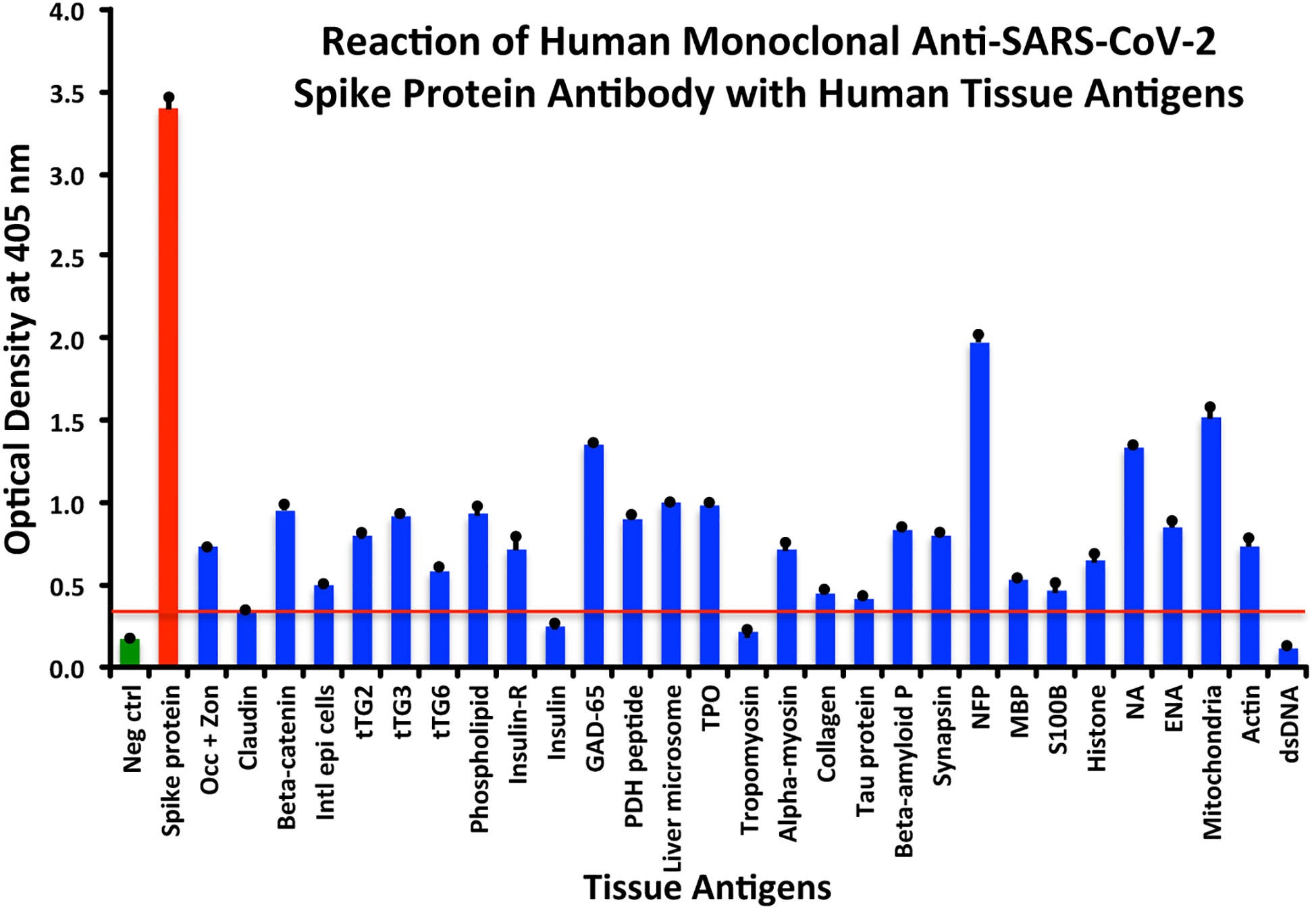
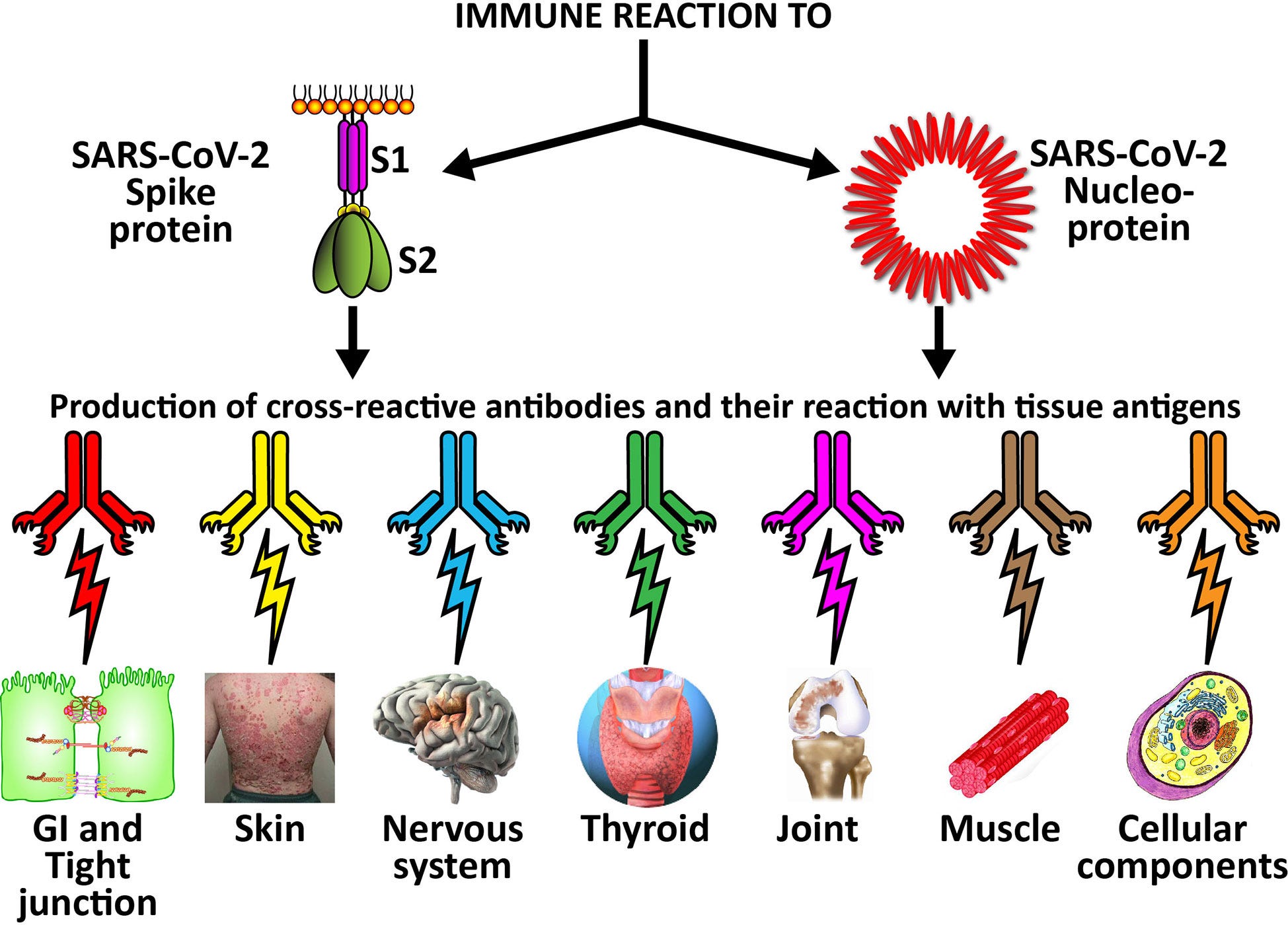


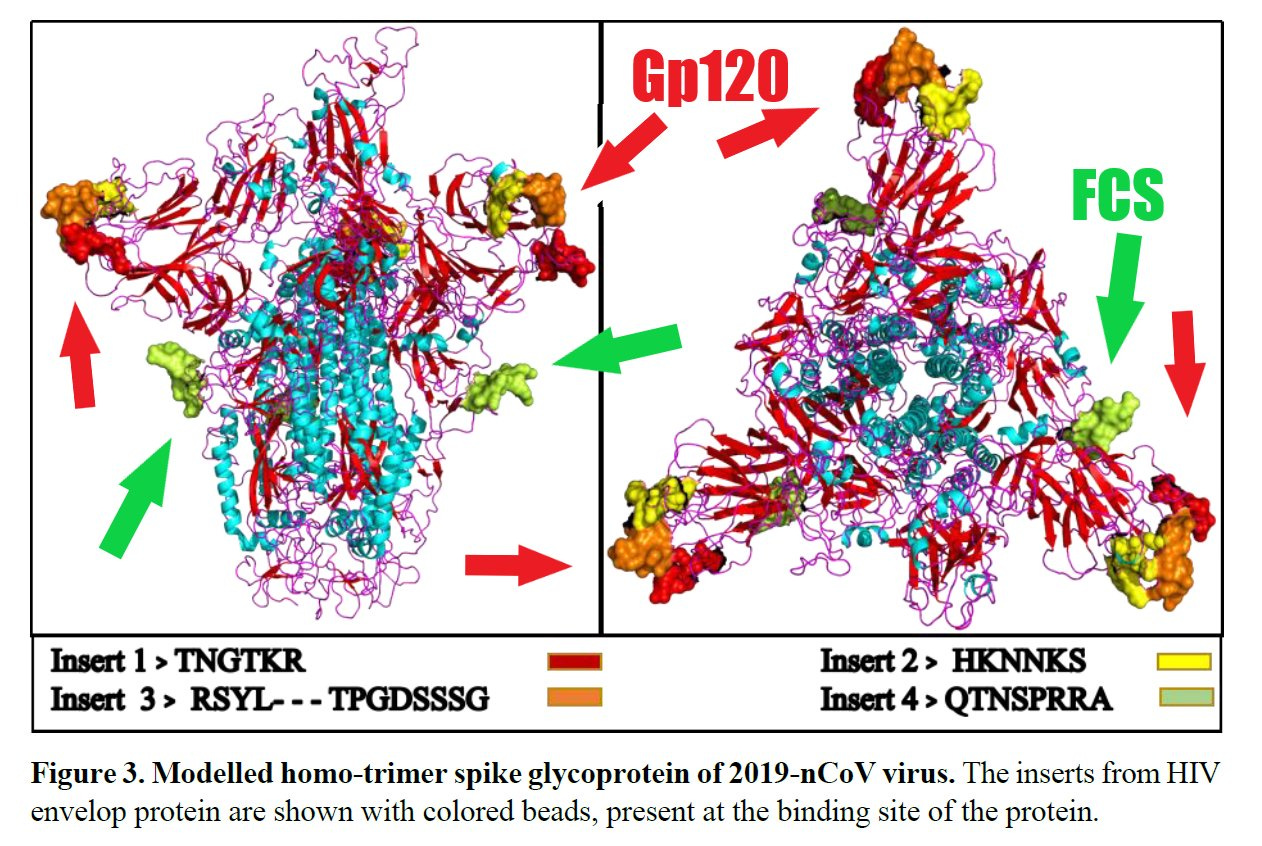
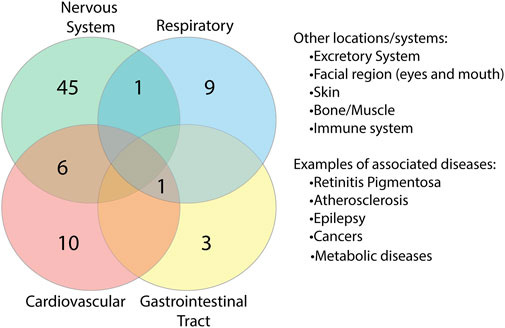

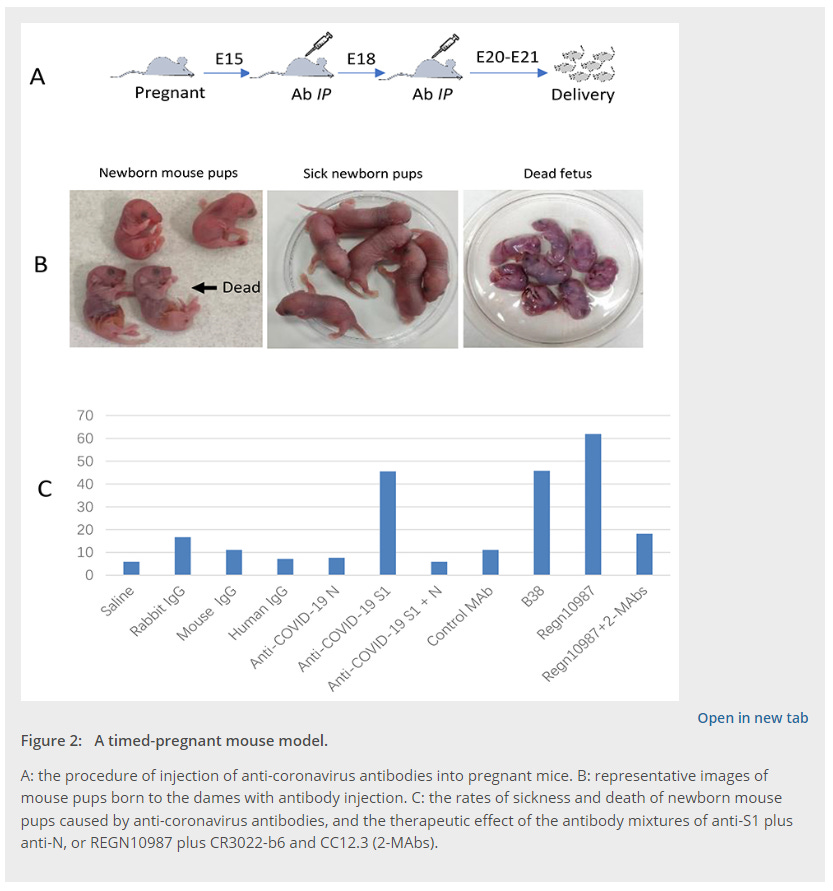


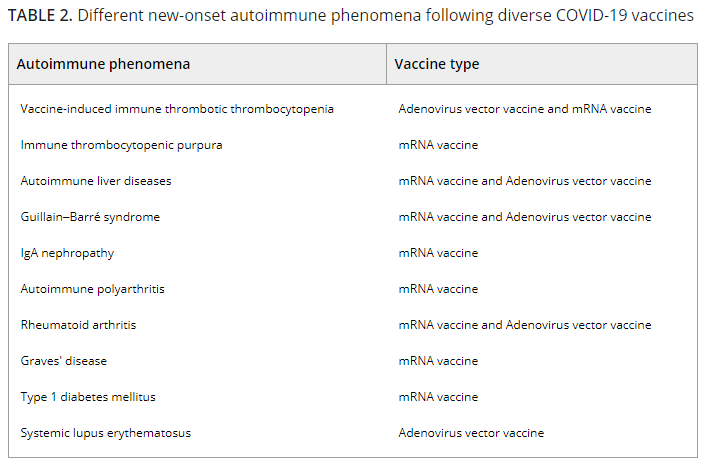




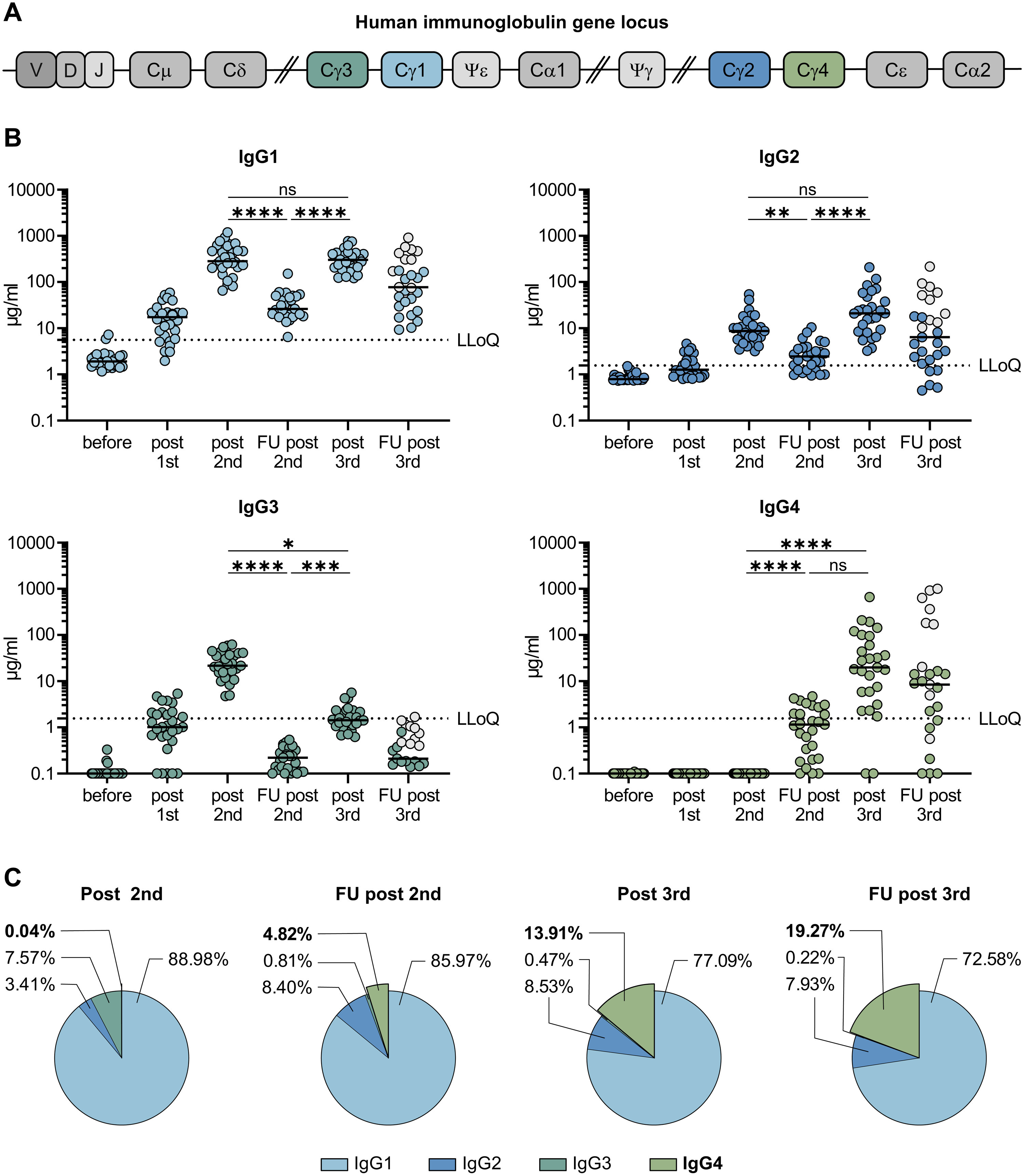
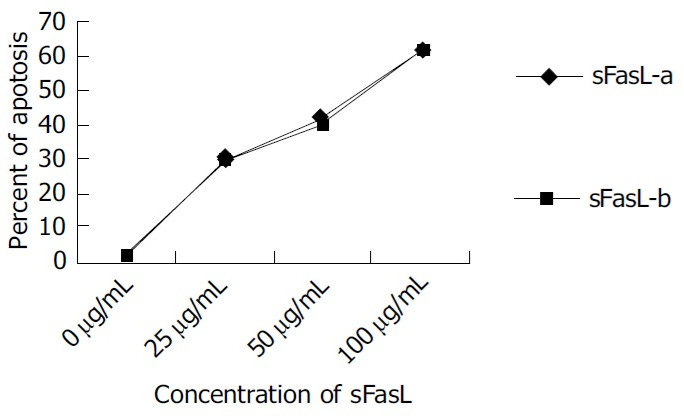












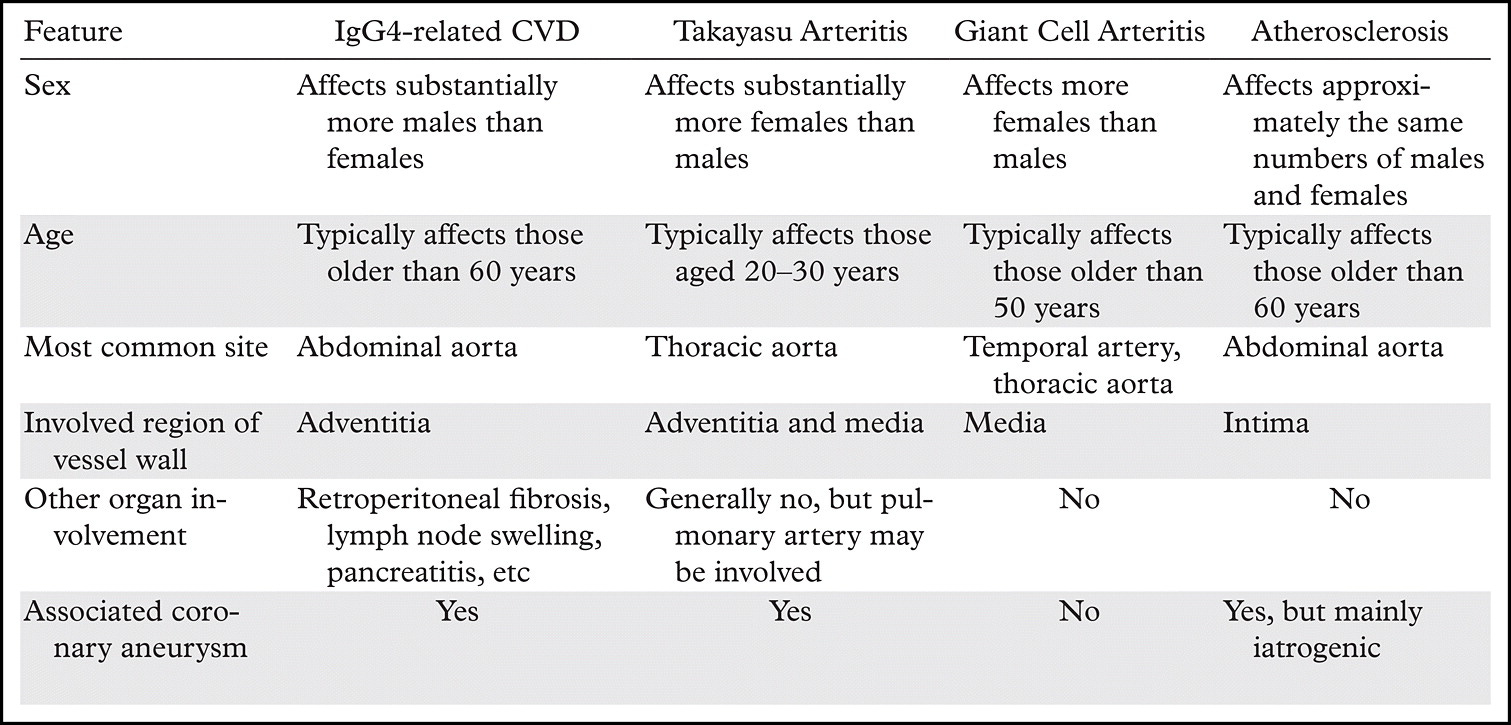




. In addition, memory B cells (bottom) from patients with HIV have been shown to be “exhausted,” which is similar to anergy. B cells with a similar phenotype have also been found in other chronic infectious diseases including HCV8 and malaria.7")
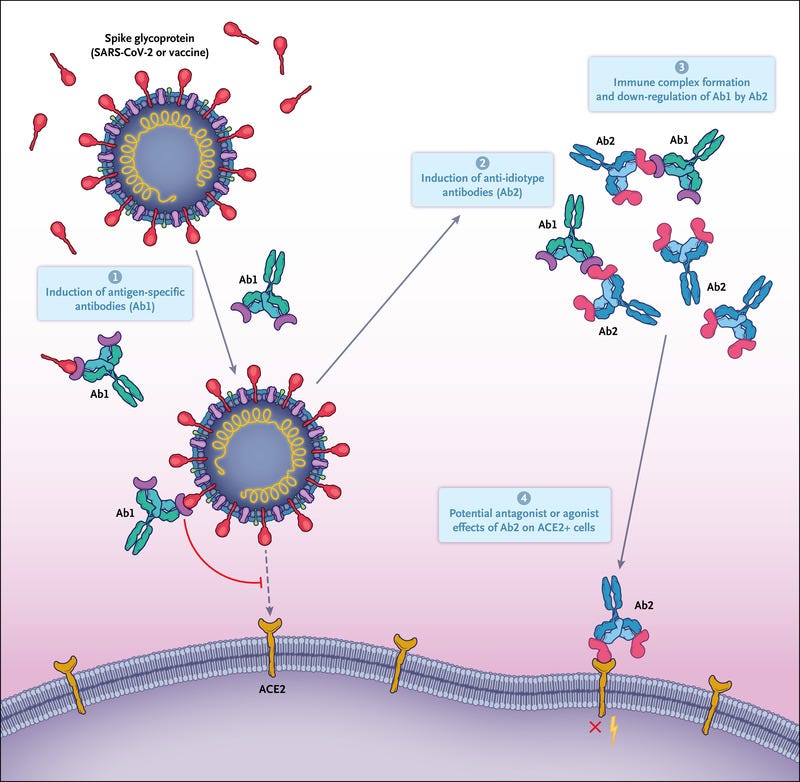

New paper reviewed by Walter:
New Onset Autoantibodies After Any Exposure to the Spike Protein of SARS-CoV-2
Evidence proving my hypothesis from 2020 that molecular mimicry of the Spike Protein is inducing autoimmune disease.
WALTER M CHESNUT
27 FEB 2024
https://wmcresearch.substack.com/p/new-onset-autoantibodies-after-any?utm_source=post-email-title&publication_id=770713&post_id=142110351&utm_campaign=email-post-title&isFreemail=true&r=if8oy&open=false&utm_medium=email
Thank you for putting all of this together. I research a lot, but I have a finite ability to understand subjects to this level of detail.
I noticed there were a lot of studies published prior to the vaccines showing the spike protein had an unprecedented degree of molecular mimicry with human tissue and various complaints to regulators sent out. Given that the vaccines were designed to have these antigens then present on the surface of cells, it became quite clear this would be a very bad idea and a recipe for autoimmunity.
In Pfizer's leaked EMA (europe's FDA) documents, they opted out of performing the required autoimmunity studies, which I took as a tacit admission it was known the vaccines would cause autoimmunity.
At this point in time, I feel the spike protein was developed to cause as many chronic long term diseases as possible in the human population.