Updated: 22nd March ‘24 (Comments from a cardiologist on the case report).
Reading time:
short story - novelette - novella 1- novel - PhD thesis - War and Peace - U.S. Tax Code
TL;DR: If you suffer from hypomagnesemia, as many of us do, addressing the deficiency may almosthalve your risk of dying from coronary heart disease, stroke, thrombosis, atrial fibrillation, sudden cardiac death, or a ruptured aneurysm.
Any extracts used in the following article are for non-commercial research and educational purposes only and may be subject to copyright from their respective owners.
Adult bodies contain around 25g of magnesium (Mg). 50-60% of this is in the bones and the rest is in soft tissues. Mg is a cofactor in at least 300 enzyme systems responsible for the regulation of many diverse biochemical reactions involved with blood pressure, blood glucose levels, protein synthesis, muscle function and nerve function.2
Mg is thus highly reactive, both physically and biologically. A lot of us had fun at school burning holes in lab workbenches as its binding with oxygen releases a lot of thermal energy. It will even ‘burn’ dry ice (frozen CO2) as magnesium is a more reactive metal than carbon, binding to form magnesium oxide:
Highly exothermic, with lots of smoke and a fire you cannot extinguish.
A bit like something else:
Incendiary bombs on wheels
Mg deficiency is commonly referred to as the ‘modern day silent epidemic’ or an ‘invisible deficiency’ as it is very difficult to diagnose just by a blood test alone. Less than 1% of our magnesium is in the blood, and of this, only less than 0.3% is in the serum, with a poor correlation to deficiency.3
It is currently estimated that 60% of adults do not get the average dietary intake (ADI) of Mg, and that around 45% of Americans are magnesium deficient. Tying in nicely with the last 2 Substacks on atherosclerosis and gut microbiota, deficiency is not just associated with these but disease states such as hypertension, diabetes, and neurological disorders, as well as many others.4
This Substack will review some of the literature concerning these, starting with cardiovascular disease (CVD).
Discussion
Pharma has a stranglehold on our health services and supporting charities, at least in the West. It's almost the rule that if a treatment is easily available, cheap, and effective then you probably won’t be told about it. It may well be that you have been treated for one or more of the following diseases for years without once being told by your doctor about the importance of magnesium.
It is not my place to tell you what to take or not, it’s about autonomy. After all, if chemotherapeutics work for you then keep going, but what reviews like this can do is offer viable alternatives, supporting evidence, and most importantly give you informed consent. Quite often alternatives are complementary to allopathic drugs, working better than each in isolation. As with microbiota and chemotherapy, some of these drugs just do not work well at all if you are Mg deficient.
(Bold emphasis mine throughout).
NHS advice about magnesium
TL;DR: You shouldn’t need to supplement. It’s good for energy and thyroid function. Don’t take too much or it will give you diarrhoea.
Advice like this makes you want to go and place an order right away, I don’t think!
Magnesium
Magnesium is a mineral that helps:
turn the food we eat into energy
make sure the parathyroid glands, which produce hormones important for bone health, work normally
Good sources of magnesium
Magnesium is found in a wide variety of foods, including:
spinach
nuts
wholemeal bread
How much magnesium do I need?
The amount of magnesium you need is:
300mg a day for men (19 to 64 years)
270mg a day for women (19 to 64 years)
What happens if I take too much magnesium?
Taking high doses of magnesium (more than 400mg) for a short time can cause diarrhoea.
There's not enough evidence to say what the effects might be of taking high doses of magnesium for a long time.
What does the Department of Health and Social Care advise?
You should be able to get all the magnesium you need by eating a varied and balanced diet.
If you take magnesium supplements, do not take too much as this could be harmful.
Having 400mg or less a day of magnesium from supplements is unlikely to cause any harm.
This is from a British Heart Foundation (BHF) forum:
Hi guys
Easy one for you this time
Magnesium yes or no ?
I saw my cardiologist for the first time friday he asked what meds I was taking so I told him and mentioned I was taking magnesium and he told me to stop taking it as they dont recommend it does anyone know why he would say that
I thought it a bit strange him saying that
Phil
The replies were mostly dismissive and along the lines of there not being enough evidence or supplementation might interfere with other drugs. Most hilarious was an acknowledgment that Mg can lower your BP! It acts as a natural calcium blocker; we will return to this later.
Magnesium supplements can interact with some calcium channel blockers causing blood pressure to drop to low. Then can also interfere with blood clotting medication reducing there effectiveness.
Also, most supplements are pretty useless as most of the content is excreted in the urine.
You are much better off get your magnesium from food sources such as green leafy vegetables, seafood and legumes.
Picking up the last point, to get your adult RDA of 300mg of Mg from one of the richest vegetable sources, you would need to put away about 350g of cooked spinach, every day.5
Now I love spinach leaves but the thought of that turns me green.
Diet is usually the best source but for various reasons may not suffice, and I will discuss this in the next Substack.
Cancer Research UK (CRUK) don’t even bother mentioning the M-word; they are very dismissive in general about alternatives.
And they sure like to scare the bejesus out of you!
Check with a pharmacist or your healthcare team before taking any supplements. Some of these could interfere with how well cancer drugs work. Supplements at a high dose could be toxic or harmful to your health..
Side effects
Some vitamins or minerals could interfere with how well cancer drugs work. Antioxidant supplements such as co enzyme Q10, selenium and the vitamins A, C and E can help to prevent cell damage. But there is some evidence that taking high dose antioxidant supplements during cancer treatment might make the treatment less effective.
Get advice from your doctor, specialist nurse or dietitian if you want to take supplements and are having any kind of cancer treatment.
Individual supplements and vitamins
There is no reliable evidence that dietary or nutritional supplements can prevent, cure or control the growth of cancer. Check with your specialist before you take any supplements to make sure they won't interfere with any cancer treatment you are having.
Dang it, according to Cancer Research UK there is “no reliable evidence”.
If only they had access to multi-million-pound research funding, scientists, and facilities to confirm previous findings with further studies and clinical trials.
CRUK circular logic
Putting pharma-funded myths to one side, let us look at the experimental evidence and meta-analyses.
Cardiovascular Disease
As for the main BHF site, it doesn’t mention magnesium once as a therapeutic. This is curious since its benefits have been known since at least the 1930s. Just how much research do these charities need?6
For nearly 8 decades, researchers have extensively studied the roles of magnesium in cardiovascular health. In 1935 Zwillinger (7.) first reported that intravenous injection of magnesium sulfate suppressed digitalis-induced cardiac arrhythmia in humans. In the late 1950s the hypothesis that magnesium intake reduces cardiovascular risk gained further support from ecologic studies, including Kobayashi’s (8.) first report of inverse correlations between regions of different water hardness and mortality rates due to cerebrovascular diseases in Japan, which were subsequently confirmed in many additional ecologic studies of different geographical areas of diverse populations.
Magnesium is necessary to activate vitamin D, to unlock all its systemic benefits:789
Magnesium is Required to Activate vitamin d
Magnesium is needed to move vitamin D around in the blood and to activate vitamin D.4 Magnesium deficiency can also reduce active vitamin D (1,25 dihydroxyvitamin D) levels and impair parathyroid hormone response.31 This may lead to “magnesium-dependent vitamin-D-resistant rickets.”32 Magnesium is also required to inactivate vitamin D when levels become too elevated.4 Thus, optimal magnesium status is required for optimal vitamin D status.33Both magnesium and vitamin D are important to the immune system independently. Together, they may be beneficial in COVID-19 infection because magnesium is necessary to activate vitamin D.
From: “Figure 2. Possible roles of magnesium in vitamin D synthesis. Magnesium is involved in both activation and inactivation of vitamin D. Abbreviations: 1,25(OH)2D, 1,25-dihydroxyvitamin D (biologically active form); 24,25(OH)2D, 24,25-Dihydroxyvitamin D; 25(OH)D, calciferol (inactive form); D2, vitamin D2 (from nonanimal sources); D3, vitamin D3 (from animal sources); DBP, vitamin D–binding protein; Mg, magnesium; VDR, vitamin D receptors.” Source: https://www.degruyter.com/document/doi/10.7556/jaoa.2018.037/html
Vitamin D also needs vitamin K2 to decrease undercarboxylated osteocalcin. This is necessary to move calcium from where it is not needed (lining your arteries) to where it is needed, in your bones, contributing to bone mineral density (BMD).10
You may therefore find that you aren’t just deficient in Mg, but D, K2 as well as zinc and copper.1112
Ca supplementation alone is not recommended for fracture prevention in the general postmenopausal population. Patients at risk of fracture with insufficient dietary intake and absorption could benefit from calcium supplementation, but it needs to be customized, taking into account possible side-effects and degree of adherence. VitD supplementation is essential in patients at risk of fracture and/or vitD deficiency. VitK2 and Mg both appear to be involved in bone metabolism. Data suggest that VitK2 supplementation might improve bone quality and reduce fracture risk in osteoporotic patients, potentially enhancing the efficacy of Ca ± vitD. Mg deficiency could negatively influence bone and muscle health.
In 2018 DiNicolantonio et al discussed how subclinical (= asymptomatic) magnesium deficiency contributes to a public health cardiovascular disease crisis.13 Anathema to the pharma model, it’s cheap and easy to fix!
Certain individuals will need to supplement with magnesium in order to prevent suboptimal magnesium deficiency, especially if trying to obtain an optimal magnesium status to prevent chronic disease. Subclinical magnesium deficiency increases the risk of numerous types of cardiovascular disease, costs nations around the world an incalculable amount of healthcare costs and suffering, and should be considered a public health crisis. That an easy, cost-effective strategy exists to prevent and treat subclinical magnesium deficiency should provide an urgent call to action.
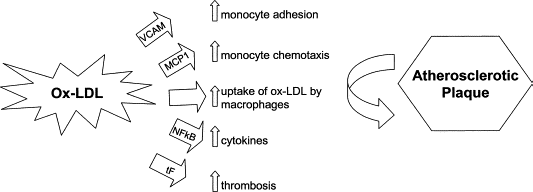
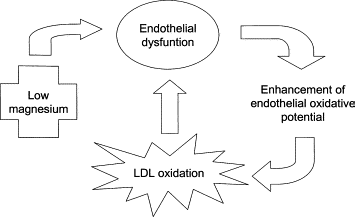
Maier (2003 and 2011) and discussed how low magnesium can mediate heart disease through various mechanisms; particularly through oxidation of LDL and endothelial dysfunction leading to plaque formation.1415
LDL = low-density lipoprotein; sometimes called “bad cholesterol”:
Experimentally induced low plasma levels of magnesium accelerate atherogenesis by increasing LDL concentrations and their oxidative modifications, and by promoting inflammation. In vitro studies have shown that low magnesium determines endothelial dysfunction, the initiating event leading to the formation of the plaque. Moreover, oral magnesium therapy has been shown to improve endothelial function in patients with coronary artery disease. Magnesium, which is an inexpensive, natural and rather safe element, could be useful in preventing atherosclerosis and as an adjuvant therapy in patients with clinical manifestations of the disease.
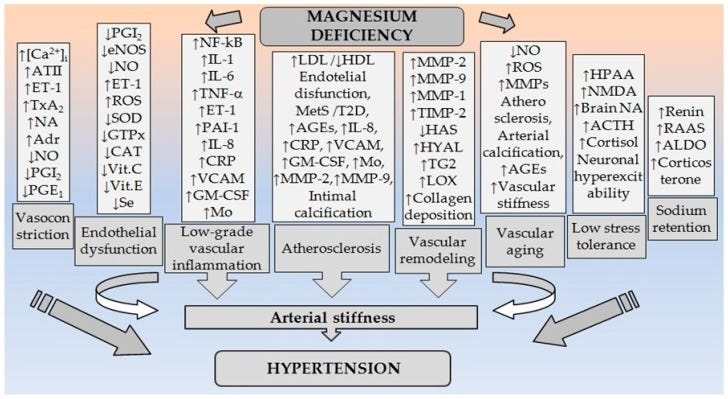
In 2018, Kostov & Halacheva further discussed this in “Role of Magnesium Deficiency in Promoting Atherosclerosis, Endothelial Dysfunction, and Arterial Stiffening as Risk Factors for Hypertension”.16 Not only does Mg act as a natural anti-hypertension drug but it has other atherosclerosis inhibiting effects we are more familiar with from studies into ACE-inhibitors.
Key takes and interpretation:
MgD = Magnesium deficiency
Calcium deposits in your arteries can cause them to stiffen. Magnesium helps prevent this. It also increases the production of substances that help blood vessels to expand, thus lowering blood pressure, whilst countering substances that cause blood vessels to constrict:
Magnesium is a natural calcium antagonist. It potentiates the production of local vasodilator mediators (prostacyclin and nitric oxide) and alters vascular responses to a variety of vasoactive substances (endothelin-1, angiotensin II, and catecholamines).
Magnesium helps prevent atherosclerosis by reducing inflammation and oxidation:
MgD stimulates the production of aldosterone and potentiates vascular inflammatory response, while expression/activity of various antioxidant enzymes (glutathione peroxidase, superoxide dismutase, and catalase) and the levels of important antioxidants (vitamin C, vitamin E, and selenium) are decreased.
Produced by the adrenal glands, catecholamines are “fight or flight” neurotransmitters and hormones produced in response to stress. This is great for escaping from sabre-toothed tigers, but in excess they can produce coronary spasm, arrhythmias, and cardiac dysfunction by inducing intracellular Ca2+ overload in cardiomyocytes:17
Magnesiumbalances the effects of catecholamines in acute and chronic stress.
MgD may be associated with the development of insulin resistance, hyperglycemia, and changes in lipid metabolism, which enhance atherosclerotic changes and arterial stiffness.
“Matrix metalloproteinase” (MMP) is a mouthful, but where you see the suffix -ase you have an enzyme in biochemistry. In this case, MMP speeds up the breakdown of collagen and elastin proteins. Normally age-associated, this is bad as with impaired vascular wall strength you are at elevated risk of stroke, aneurysm, or dissection:
Magnesiumregulates collagen and elastin turnover in the vascular wall and matrix metalloproteinase activity.
If an artery is inelastic then if greater volumes of blood are going into it the blood pressure must increase to maintain flow rates or to distend the walls, leading to hypertension:
Magnesiumhelps to protect the elastic fibers from calcium deposition and maintains the elasticity of the vessels.
Considering the numerous positive effects on a number of mechanisms related to arterial hypertension, consuming a healthy diet that provides the recommended amount of magnesium can be an appropriate strategy for helping control blood pressure.
The often recommended daily intake for adults is 320–400 mg/day (or 6 mg/kg/bodyweight for both sexes) [1]. Epidemiological studies in Europe and North America show that people who consume Western-style diets have low Mg2+ content, <30–50% of the RDA for Mg2+.
It is assumed that the Mg2+ intake in the USA has decreased over the past 100 years from about 500 mg/day to 175–225 mg/day. This is probably the result of the increasing use of fertilizers and processed foods [4].
Lay off the junk food and don’t boil them to death:
Refining or processing of food may deplete Mg2+ content by nearly 85%. Especially boiling of Mg2+-rich foods can result in a significant loss of Mg2+ [3].
Mineral water may help, but avoid polycarbonate bottles laden with bisphenol A (BPA), BBP, DBP, DEHP or phthalates.18
Furthermore, the incidence rate of MgD can vary considerably in different regions due to the large differences of Mg2+ content in drinking water, which can provide up to 30% of daily needs [1].
It’s not a significant source, but try to use unrefined salt. Despite its appearance Pink Himalayan salt is only about 0.1% magnesium;19 Celtic sea salt is better at 0.441%.20
Therefore, it seems reasonable to assume that MgD is mainly related to the low intake of Mg2+ in food and drinking water, including the use of purified salt to cook, which may lead to a negative balance over time [1]. The processing and cooking of food may therefore explain the apparently high prevalence of low Mg2+ intake in many populations [3].
A significant association was found between dietary Mg2+ intake and total cardiovascular disease risk. The greatest risk reduction was observed when dietary Mg2+ intake increased from 150 mg/day to 400 mg/day. Higher serum Mg2+ concentrations with 0.1 mmol/L were associated with a 9% lower risk for total cardiovascular events [8].
Mechanisms contributing to this. Choose your weapon:
Prevention of vascular calcification is particularly useful.
HTN = Hypertension
VSMCs = Vascular smooth muscle cells
Another pathogenic feedback loop:
Vascular calcification is the extracellular deposition of Ca2+ in the arterial wall and is intimately linked with the HTN. On the other hand, HTN was considered a risk factor for atherosclerosis and associated calcification.
Two types of extracellular vascular calcification are recognized, intimal and medial. Intimal calcification is exclusively associated with atherosclerosis. Medial calcification may contribute to increasing BP by decreasing the elasticity of the media.
Decreased elasticity results in arterial stiffening which accelerates pulse wave velocity and widening the pulse pressure, leading ultimately to HTN.
Intimal and, especially, medial vascular calcification are associated with arterial stiffening, the major cause of isolated systolic HTN in the elderly [103].
…studies suggested a potentially active intracellular role for Mg2+ ions in attenuating the vascular calcification process [33,35,104]. In confirmation of this, Hruby et al. reported on favorable associations between dietary and supplemental Mg2+ intake and lower calcification of the coronary arteries [105].
It's never too late to start:
Furthermore, it was found that higher Mg2+ levels prevented calcification of bovine VSMCs, and further progression of the already established calcification.
The Wnt/β-Catenin pathway regulates stem cell pluripotency (cell fate decisions) during tissue development:
Inhibition of the Wnt/β -catenin signaling pathway was identified as one of the possible intracellular mechanisms by which Mg2+ achieved its anti-calcifying effect [104].
Ultimately, the view is that MgD in patients with HTN is linking with significant adverse effects on BP. In the Atherosclerosis Risk in Communities (ARIC) study, serum Mg2+ level in hypertensive patients was inversely proportional to the systolic BP.
It should be noted that MgD is not found in all patients with HTN. On the other hand, not all people with hypomagnesemia have high BP. These differences are probably due to the fact that patients with high BP do not constitute a homogenous group [78]. This may be one of the possible causes for the discrepancy between epidemiological and clinical data.
Hypomagnesemia = “an electrolyte disturbance caused by a low serum magnesium level of less than 1.46 mg/dL in the blood. However, this condition is typically asymptomatic until serum magnesium concentration is less than 1.2 mg/dL (0.5 mmol/L).”21
Despite these discrepancies concerning Mg2+ status and high BP, some hypertensive patients constantly demonstrate hypomagnesemia. Among them are patients with obesity, insulin resistance, hypertriglyceridemia, severe forms of HTN, hyperaldosteronism (volume-dependent HTN), pregnancy induced HTN, and patients of African-American origin [120].
Many nutritional experts feel the ideal intake for Mg2+ should be based on the body weight (e.g., 4–6 mg per kg/day) [4].
As our vascular system ages, our risk of MgD grows due to reduced intake, reduced absorption, increased renal wastage, decreased renal reabsorption, age-related illnesses, and due to side effects of drugs to treat these. Impaired magnesium take-up can, in turn, contribute to vascular aging in positive feedback loops:
At the molecular and cellular levels, arterial aging and HTN-associated vascular changes are characterized by reduced NO production, increased generation of reactive oxygen species (oxidative stress), activation of transcription factors, induction of “aging” genes, stimulation of proinflammatory and profibrotic signaling pathways, reduced collagen turnover, calcification, VSMCs proliferation, and ECM remodeling. These processes contribute to increased fibrosis, which is further promoted by prohypertensive vasoactive agents, such as ATII, ET-1, and ALDO [12].
A final note on treating hypertension by addressing mineral imbalances was discussed by Houston (2011). Although supplementing with magnesium in isolation was shown as effective in several studies, the best results were obtained by reducing sodium along with increased intake of both magnesium and potassium. This was often as effective as taking one antihypertensive drug.22
I have had to warn about an incoming wave of early deaths as both synthetic mRNA gene therapies and statin poisons lead to accelerated aging of your cardiovascular system. By your 50’s, you may have the CV system of an 80-year-old.
We don’t have the complete medical history but this is representative:
Tragic cardiac arrest
Aircraft Type: Piper PA-28-161 Cherokee Warrior II
Date & Time: 29 June 2022 at 1000
Commander's Flying Experience: CPL, 8,876 hours
Last 90 days: 184 hours
Last 28 days: 78 hours
A qualified pilot had planned to fly the PA-28 from Blackpool Airport to another airfield but when he arrived at the flying club and checked the latest wind, he decided the crosswind was above his personal limit to fly on his own. Still wanting to go flying so that he remained within the flying club's recency requirements, the pilot asked an instructor if he would accompany him for a single circuit. The instructor agreed to fit in the circuit after he finished a trial lesson.
Following the trial lesson the instructor met the pilot in the PA-28 and the pilot taxied the aircraft out to the runway. The pilot recalled that during the taxi they were talking normally.
He recalled telling the instructor he would keep the aircraft into wind for the power checks and the instructor replying. "looks good, there is nothing behind you". The pilot did not recall the instructor saying anything else after this point.
The pilot recalled that shortly after takeoff from Runway 28 the instructor's head rolled back. The pilot knew the instructor well and thought he was just pretending to take a nap whilst the pilot flew the circuit, so he did not think anything was wrong at this stage, He proceeded to fly the aircraft round the circuit.
As he turned onto base leg the instructor slumped over with his head resting on the pilot's shoulder, The pilot still thought the instructor was just joking with him and continued to fly the approach, He landed normally on Runway 28 and started to taxi back to the apron, However, the instructor was still resting on his shoulder and was not responding, and the pilot realised something was wrong. He signalled to the airport fire crew, who happened to be working on the apron, who came to assist. The fire crew and the air ambulance medical crew, who are based at the airport, attempted to revive the instructor but he remained unresponsive and they were unable to save him.
The instructor was 57 years old. He held a commercial pilot's licence with valid single and multi-engine piston aircraft ratings, a valid Instrument Rating and a Flight Instructor Rating.
He was employed as a full-time senior flight instructor, and had accumulated a total of 8,876 flying hours. He held a valid Class One Medical and his last aviation medical was on 10 February 2022, approximately four months before the incident flight. People who had spoken to him on the morning of the incident said he was his normal cheerful self and there were no indications that he was feeling unwell. The three people who had flown with him for the trial lesson just prior to the incident flight said he seemed well and nothing abnormal had occurred.
The post-mortem concluded that the instructor died from acute cardiac failure. His coronary arteries showed diffuse atheromatous disease (a condition where the arteries become clogged with fatty substances) and there was a coronary thrombus(blood clot) occluding his left main stem artery. Toxicology showed no significant findings. He had medical history of hypertensive disease (high blood pressure) and had been taking blood pressure medication since 2002.
Pilot magazine. May 2023; 65.
I asked a paramedic doctor friend about this case and they commented that this doesn’t appear to be your typical heart attack (myocardial infarction, MI).
Despite his medical history the patient didn’t appear to have any significant symptoms before the incident, he was very rapidly unconscious, the student thought he was joking, and thrombus blocking of the left main coronary artery appears to be critical.
Comments from a cardiologist:
LV = Left ventricle.
“A thrombotic occlusion of the left coronary main stem renders such a large part of the LV ischaemic that sudden cardiac death can also occur via left heart failure (close to electromechanical dissociation).”
- Cardiac arrhythmia
What Is an Arrhythmia?
An arrhythmia, or irregular heartbeat, is a problem with the rate or rhythm of your heartbeat. Your heart may beat too quickly, too slowly, or with an irregular rhythm. It is normal for your heart rate to speed up during physical activity and to slow down while resting or sleeping. It is also normal to feel as if your heart skips a beat occasionally. But a frequent irregular rhythm may mean that your heart is not pumping enough blood to your body. You may feel dizzy, faint, or have other symptoms.
Arrhythmias are treatable with medicine or procedures to control the irregular rhythms. If not treated, arrhythmias can damage the heart, brain, or other organs. This can lead to life-threatening stroke, heart failure, or cardiac arrest. During cardiac arrest, the heart suddenly and unexpectedly stops beating, causing death if it is not treated within minutes.
Even as far back as 1986 researchers like Laban & Charbon were commenting about how under-reported magnesium was as a therapeutic.
Key takes from the abstract for “Magnesium and cardiac arrhythmias: nutrient or drug?”:23
The antiarrhythmic potency of Mg has been described repeatedly since 1935, both as a factor in human disease and in animal experiments. Nevertheless, this therapeutic efficacy is rarely mentioned in textbooks.
Both the pharmacological effect of Mg and the correction of Mg deficiency have been used in treatment of digitalis toxicity, variant angina, Torsades de Pointes, as well as in arrhythmia of unknown origin.
Digitalis is a cardiac glycoside that treats heart failure by affecting the balance of sodium and potassium in heart cells; Gentamicin is a strong aminoglycoside antibiotic; Cisplatin is a platinum-containing chemotherapy medication:
The most frequent cause is probably alcoholism. Iatrogenic factors include digitalis, diuretics, gentamicin, as well as cisplatinum, which appreciably enhance urinary Mg loss. Correction of Mg-deficiency by parental and/or oral administration should lead to recovery.
As far as PubMed is concerned there are relatively few reviews into the use of magnesium to treat arrhythmias, and most of these are from the 1980’s and 90’s.
In 2013, 3530 participants (mean age, 44 years; 52% women) from the Framingham Offspring Study had their serum magnesium analysed to look for any association with the incidence of atrial fibrillation.
In the 20 years of follow-up, 228 participants developed AF. 9.4 per 1000 person-years (95% confidence interval, 6.7-11.9) were in the lowest quartile of serum Mg. This compared to 6.3 per 1000 person-years (95% confidence interval, 4.1-8.4) in the highest quartile of serum Mg (≥1.99 mg/dL) - a reduced incidence of 50%.24
The most recent study of interest was from 2017 by Baker, and the lack of funding for further research means that there are still many gaps in the literature.
We keep coming back to the Willie Sutton Rule for investing and how it is the business model used by Pharma and for the charities they sponsor:
“…it stresses the need for an individual to focus on activities that generate high returns, rather than on actions that might be frivolous or yield lower returns.”25
We're the single biggest independent funder of cardiovascular research in the UK. In recent years, we have invested around £100 million each year in research into heart and circulatory diseases. We work on policy to ensure the research environment is protected and can thrive.
Key takes from “Treating arrhythmias with adjunctive magnesium: identifying future research directions“26 (2017):
Magnesium is the fourth most abundant cation in the human body and is the second most prevalent cation in intracellular tissues. Myocardial cell action potentials are mediated by voltage-dependent Na+, K+, and Ca2+ channels which, when their function is altered, can lead to the genesis of cardiac dysrythmias.
Magnesium regulates the movement of ions through these channels within myocardial tissues. The potential ability of magnesium supplementation to prevent and/or treat arrhythmias has been recognized in clinical medicine for years.
Torsade de pointes = “an uncommon and distinctive form of polymorphic ventricular tachycardia (VT) characterized by a gradual change in the amplitude and twisting of the QRS complexes around the isoelectric line (see the image below). Torsade de pointes, often referred to as torsade, is associated with a prolonged QT interval, which may be congenital or acquired. Torsade usually terminates spontaneously but frequently recurs and may degenerate into ventricular fibrillation.”
From: “Torsade de Pointes. Torsades de pointes with prolonged QT interval (12-lead ECG of torsades de pointes (TdP) in a 56-year-old white female with low blood potassium (2.4 mmol/L) and low blood magnesium (1.6 mg/dL). Courtesy of Wikimedia Commons [Author Jason E Roediger, CCT, CRAT, https://commons.wikimedia.org/wiki/File:Torsades_de_Pointes_TdP.png].” Source: https://emedicine.medscape.com/article/1950863-overview
This includes termination of torsade de pointes, prevention of post-operative atrial fibrillation, acute treatment of atrial fibrillation, and improving the efficacy and safety of antiarrhythmic drugs.
Worth researching and trialling in depth, you would think?
Despite what is currently known about magnesium’s therapeutic potential, a number of limitations and gaps to the literature exist. Examples include the true incidence and impact of intracellular magnesium deficiency, target serum and intracellular magnesium concentration targets, the most efficacious magnesium salt form (Table 1),31 and the optimal dose and timing of magnesium administration.
From: “Figure 1 Effects of magnesium on the heart and vasculature. Reprinted with permission from reference 3. AV, atrioventricular; IL-1, interleukin-1; IL-6, interleukin-6; MVO2, myocardial oxygen consumption; NO, nitric oxide; PAI1, plasminogen activator inhibitor-1; PGI2, prostacyclin; PVR, peripheral vascular resistance; VCAM-1, vascular cell adhesion molecule-1.” Source: https://academic.oup.com/ehjcvp/article/3/2/108/2669829?login=false
IKr, is a part of the control mechanism for ventricular repolarization. “It is a crucial step in cardiac electrical activity consisting of a recovery period with the return of the ions to their previous resting state, which corresponds with the relaxation of the myocardial muscle, thus setting the stage for the next depolarization and contraction”.27
TdP = torsade de pointes.
One of the more common uses of i.v. magnesium is for the treatment of TdP.28 In fact, low tissue magnesium concentrations is associated with increased QT dispersion, potentially representing a risk factor for the development of triggered arrhythmias such as TdP.61Torsade is thought to occur as a result of early after-depolarizations (EADs) resulting in triggered automaticity, unidirectional block, and intramural re-entry circuit development.62Magnesium suppresses the EADs and automaticity by decreasing IKr current and L-type Ca2+ activity (which is thought to be responsible for the triggered automaticity), thereby terminating the rhythm.63–65
AF = atrial fibrilation.
Approximately 25–40% of patients undergoing cardiac surgery develop post-operative AF, resulting in prolonged hospital length of stay, increased risk of stroke, and higher hospital costs.67,68 Studies show a significant association between low pre-operative intracellular magnesium concentrations and an elevated risk of post-operative atrial fibrillation (POAF).69,70
Studies have shown that up to 38% of patients with sustained ventricular arrhythmias have a serum magnesium deficiency and 72% have an excessive magnesium loss.97 Correction of this deficiency with i.v. magnesium resulted in a decrease in ventricular ectopic beats (P < 0.0001), couplets (P < 0.003), and episodes of non-sustained VT (P < 0.01) vs. placebo.97 Oral supplementation with magnesium and potassium also reduced ventricular premature beats (P = 0.001) vs. placebo over a 3-week period.98 A number of case reports have also showed magnesium to be effective for terminating various drug-induced ventricular arrhythmias.24–27
The BHF, and others, are clearly in no hurry. If magnesium was rare and precious it might be a different story. Until then we have to do our own research.
These gaps in evidence make incorporating the potentially important research findings into practice a challenge for clinicians caring for high-risk patients. They also represent critical need of study to allow the large body of evidence with magnesium to be translated to clinical practice.
One trial that was conducted by Nielsen et al in 2007 had the following objective:
“To determine whether or not dietary magnesium restriction to about 33% of the Recommended Dietary Allowance (RDA) causes changes in glucose, cholesterol and electrolyte metabolism that could lead to pathologic consequences.”28
Thirteen women aged 45 -75 completed the study. They confirmed that magnesium depletion due to poor diet was associated with AF (and therefore risk of death), and that this quickly responded to supplementation.
Key takes from “Dietary magnesium deficiency induces heart rhythm changes, impairs glucose tolerance, and decreases serum cholesterol in post menopausal women"29
Results: During magnesium depletion, heart rhythm changes appeared in 5 women and resulted in 4 prematurely entering the magnesium repletion period (42 to 64 days of depletion instead of 78). Three women exhibited atrial fibrillation and flutter that responded quickly to magnesium supplementation. Magnesium deprivation resulted in a non-positive magnesium balance that became highly positive with magnesium repletion. Magnesium deprivation decreased red blood cell membrane magnesium, serum total cholesterol and erythrocyte superoxide dismutase concentrations, increased the urinary excretion of sodium and potassium, and increased serum glucose concentration.
Conclusions: Magnesium balance may be a suitable indicator of magnesium depletion under experimental conditions. Magnesium deficiency resulting from feeding a diet that would not be considered having an atypical menu induces heart arrhythmias, impairs glucose homeostasis, and alters cholesterol and oxidative metabolism in post menopausal women. A dietary intake of about 4.12 mmol (100 mg) Mg/8.4 MJ is inadequate for healthy adults and may result in compromised cardiovascular health and glycemic control in post menopausal women.
I’m actually impressed that they were able to pull this off:
Upon arrival in the metabolic unit, all women immediately began consuming the basal magnesium-deficient diet. The original design of the experiment was to have the magnesium deprivation period to last 93 days, but because of heart arrhythmias, this was shortened to 78 days. The subjects were replenished with magnesium for 58 days by supplementing the diet with 8.23 mmol (200 mg) of magnesium as magnesium gluconate per day.
You may wonder what Mg-deficient diet they gave them for trial purposes?
The diet used in the study was based on ordinary Western foods and is shown in Table 1. A three-day menu rotation was used to give some variety but assured that variation in nutrient intake was not consequential. As shown in Table 2 the diet supplied approximately 101 mg (4.16 mmol) magnesium per 8.4 KJ (2,000 kcal).
This intake was near the first percentile intake of women aged over 51 years according to the 1994 Continuing Survey of Food Intake of Individuals (CSFII) [21]. The diet energy distribution was 9.7% protein, 36.1% fat and 54.2% carbohydrate. The diet was based on the 1989 Recommended Dietary Allowances (RDA) [20] because it was formulated before the issuance of the current Dietary Reference Intakes.
They did give them supplements as the independent variable was magnesium, not other essentials:
To assure adequacy, supplements were used for nutrients present in low or unknown quantities in the diet. These supplements were (per day) 625 mg (16 mmol) potassium as potassium chloride, 270 mg (6.74 mmol) calcium as calcium gluconate, 20 mg (0.36 mmol) iron as ferrous gluconate, 6 mg zinc (92umol) as zinc sulfate, 1.1 mg (17umol) copper as copper sulfate, 0.33 mg boron (31umol) as boric acid, 133ug(301 mmol) of folic acid, 100ug biotin, and 400 IU of vitaminD3.
Unfortunately it's all too easy to have a diet that is potentially fatally deficient in Mg, just like their 2/3rds deficient rotating menu.
It's one of the reasons why I take Mg as part of my essential daily stack.
I would say this selection is quite typical for a lot of us, or even a step up in nutrition for some!
Fig. 2 indicates that serum magnesium concentration responded differently than red blood cell membrane concentration to magnesium deprivation. Initially, serum magnesium decreased, but rebounded to the admission value on day 40 and appeared to decline slightly the last 20 days of the magnesium deprivation period.
Albumin is water soluble and the most abundant circulating protein found in plasma.
Macroglobulins are large globular proteins and are also found in the blood and other body fluids.
Linear regression analysis conducted in 1985 suggested that 25% of the total serum magnesium is bound to albumin and 8% to globulins,30 and boneacts as a magnesium pool to buffer abrupt changes in serum Mg concentration.31
Consuming the diet providing 12.67 to 13.13 mmol (308 to 319 mg) Mg/d did not increase the serum magnesium concentration. If just the last five weeks in each dietary period are used for the comparison, serum magnesium concentration was higher during magnesium depletion than repletion (Table 5). Both the albumin-bound and macro-globulin serum fractions were involved in this significant serum difference (Table 5).
It still took up to two weeks for the supplementation to correct heart rhythm changes, it’s not necessarily instant:
The first woman (age 59.5 years) began the magnesium repletion period after 42 days of deprivation because of the appearance of atrial flutter and fibrillation. These heart rhythm changes disappeared two weeks after the magnesium repletion was started and did not reappear for the remainder of the study.
After 64 days of magnesium depletion, a subject (age 65.2 years) exhibited atrial flutter andfibrillation that disappeared shortly after magnesium repletion and did not appear. At 75 days, another subject (age 47.2 years) exhibited an increase in VPDs and atrial flutter. The atrial flutter disappeared two weeks after magnesium repletion began and the VPDs declined to below baseline at the end of the magnesium repletion period.
These were low to start with:
Blood pressure was not significantly affected by magnesium depletion. During the last five weeks of depletion and repletion the mean systolic/diastolic pressures of the 13 volunteers were 114/70 mm and 113/70 mm, respectively.
This is encouraging, and comparable in efficacy to the ACE inhibitor drug Lisinopril, but without its side effects:32
However, the volunteer that showed heart rhythm changes after 42 days of depletion had an elevated mean blood pressure of 146/89 mm during depletion that decreased to an average 126/81 mm during the last five weeks of magnesium repletion.
Arrhythmia is a good marker for Mg deficiency:
One sign of primary dietary magnesium deficiency most likely is heart arrhythmia. In this study, the arrhythmias that responded the best and quickest to magnesium repletion were atrial flutter and fibrillation (exhibited by three subjects). Increased VPDs during the magnesium depletion period did not respond quickly to magnesium repletion, but the number ofVPDs decreased to baseline in one subject, near baseline in another, and below baseline in a third by the end of repletion.
The suggestion that atrial flutter and fibrillation can result from dietary magnesium deficiency is supported by the finding that supplemental magnesium has been used to successfully convert atrial fibrillation to sinus rhythm [11]. Also, patients with atrial fibrillation have been found to have low erythrocyte magnesium concentrations [31].
Magnesium regulation of sodium and potassium is important too:
The heart arrhythmias also may have been related to the change in the urinary excretion of sodium and potassium. Feyertag et al [33] found that a magnesium supplement of 15mmol magnesium citrate compared to a placebo for 3 weeks given to patients after myocardial infarction decreased ventricular extrasystoles. Urinary potassium and sodium excretion also increased in the magnesium supplemented patients.
Much evidence exists that magnesium has a regulatory role in Na+ and K+ transport, cellular distribution, and intracellular concentration. Magnesium activates the Na+,K+-ATPase pump that has a major role in regulating Na+ and K+ transport[34].
They didn’t expect this, and it shows that low cholesterol is not necessarily a good thing. This was the foundation of the long-debunked “lipid hypothesis”:33
The finding that the concentration of total cholesterol was lower during magnesium depletion than repletion was surprising.
Perhaps the change in circulating cholesterol reflected a change in erythrocyte cellular membrane lipid composition. Lipid components of the erythrocyte mem-brane exchange rapidly with plasma lipoproteins, and erythrocyte cellular membrane composition and fluidity is altered by magnesium deficiency [8].
Recent studies suggest that magnesium deficiency can promote atherogenesis through mechanisms (e.g., LDL-cholesterol oxidation, formation of pro-inflammatory substances) other than by increasing circulating cholesterol [7,38]. The only indicator of reactive oxygen metabolism measured in this study was ESOD, which was significantly decreased by magnesium deprivation.
ESOD =Erythrocyte superoxide dismutase, a critical antioxidant.
Depressed ESOD may be an indicator that dietary magnesium deficiency may enhance the susceptibility of postmenopausal women to oxidative injury.
Mg depletion can also contribute to diabetes due to impaired insulin sensitivity.
IVGTT = Intravenous glucose tolerance test.
The response to the IVGTT indicates that dietary magnesium deficiency in humans impairs glucose homeostasis. The findings that fasting glucose was higher and rose to a higher concentration suggest impaired glucose disposal and possibly decreased insulin sensitivity during magnesium deprivation.
This would be in agreement with findings that indicate intra-cellular magnesium concentration modulates insulin action and oxidative glucose metabolism, and epidemiological studies showing that higher daily intakes of magnesium are associated with a lower incidence of noninsulin-dependent diabetes mellitus [40].
Of course, I next went to the charity “Diabetes UK” for further advice on this.
I think you can guess…
Quite significant findings from this small-scale, but significant study and a profound conclusion:
The present experiment suggests that signs of dietary magnesium deficiency may include heart arrhythmias, impaired glucose homeostasis, and altered lipid and oxidative metabolism. The study also establishes that an intake of 4.12 mmol Mg/8.4 MJ (100 mg Mg/2000 kcal) is inadequate for postmenopausal women. Because 10% of the elderly women in the United States consume less than 5.6mmol (136 mg) Mg/d, magnesium deficiency may be a significant factor compromising cardiovascular health and glycemic control in this population.
Although I can only find the abstract, Ahsan (1997) adds to our understanding and why it is malfeasance not to be seriously addressing the problem outside of the ER:34
Despite the ubiquitous nature of Mg, low serum Mg occurs either from decreased absorption or due to increased excretion.
Hypomagnesemia is surprisingly common in hospital populations and is more prevalent in acute than in chronic cases but often remains undetected or overlooked.
Magnesium deficiency may result in hypokalaemia and hypocalcaemia.Myocardial Mg depletion may result in influx of Na+ and Ca+2 into the mitochondria which may lead to myocardial cell death.Hence, low Mg concentration may be a factor for a wide variety of clinical conditions.
- Aortic aneurysm
In 2015, Jolly et al conducted a retrospective analysis of the incidence of hypomagnesemia in 110 patients undergoing open or endovascularabdominal aortic aneurysm (AAA) surgery, and 101 who underwent open elective AAA repair.
35 (32%) of the endovascular repair group, and 73 patients (73%) of the open elective AAA group had hypomagnesaemia.35
This is likely to have an effect on cardiac activity and lead to cardiac complications such as arrhythmias and poorer postoperative outcomes, especially in the open AAA repair subgroup. This stresses the importance of serum magnesium and cardiac monitoring in the postoperative phase.
…Serum magnesium levels are not routinely monitored preoperatively in most elective procedures. The prevalence of hypomagnesaemia in the general population is estimated to be around 7% but is significantly higher (60%) in a postoperative intensive care setting.
…While working in a regional vascular unit, we came across a large proportion of OR patients who had hypomagnesaemia postoperatively. Likewise, a number of patients who developed a tachyarrhythmia following surgery were found to be hypomagnesaemic and were managed successfully with magnesium replacement.
From: “The incidence of hypomagnesaemia following abdominal aortic aneurysm surgery”
Magnesium-depleting drugs associated with their condition, such as diuretics, aminoglycosides, and cyclosporin.
Beta-adrenergic mediated lipolysis in response to stress and increased fatty acid circulation. This can cause insoluble magnesium soaps to precipitate out intracellular magnesium.
Higher prevalence of PPI/P-CAB use.
If you suffer from indigestion this is worth noting as proton-pump inhibitors (PPI’s) such as Omeprazole are among the top 10 most prescribed drugs in the United States. Hypomagnesemia has, since at least 2012, been recognized as a side effect of PPIs.36
An antihistamine alternative to PPI’s, Ranitidine (better known as Zantac®) was voluntarily withdrawn from the market by 2022. This is almost worthy of its own Substack, as analysis found that the drug turns carcinogenic with NDMA accumulation whilst on the shelf.37
GSK lost $30bn in market cap in the fallout last year, as Ranitidine was one of the first blockbuster drugs with $1bn in annual sales.38
A story that passed me by at the time, you may wonder why on earth this was not detected sooner?
How did it get this far and get signed off by the regulators?
Although as it was after 2020 perhaps not…
N-Nitrosodimethylamine (NDMA or DMN), a nitrosamine, acts as a transplacental carcinogen and rodent studies showed that either low doses for 7-8 months or a single high dose resulted in liver and kidney tumor formation.39
A study by Emery Pharma3 assessed the creation of NDMA during the natural degradation of the ranitidine active pharmaceutical ingredient and finished drug product over time at different temperatures. The study found that 150 mg of ranitidine tablets USP contained 18 ng of NDMA at baseline, but after storing it at 25 °C for 12 days, NDMA dosages increased to 25 ng, and storing it at 70 °C resulted in a dose increased to 142 ng. Ranitidine 150 mg, sold as Zantac Cool Mint, was found to increase from 19 ng NDMA at baseline to 70 ng NDMA when stored at 70 °C for 14 days, just below of the FDA’s maximum acceptable level.
From: “Ranitidine’s N-nitrosodimethylamine Problem May be Tip of the Iceberg“ (2021)
After Zantac was withdrawn, it was replaced by another type of antihistamine (a H2 blocker or H2 receptor antagonist, H2RA), this time containing famotidine, under the brand name Zantac 360°®
So all is good now and it won’t lead to illness and untimely deaths of thousands?
Well not necessarily, according to at least one case study. Famotidine, even though it is not a PPI and is approved by the FDA as “safe and effective”, just may re-introduce the problem of hypomagnesemia: “Famotidine might cause impaired absorption of magnesium, leading to hypomagnesemia and functional hypoparathyroidism.”4041
H2 blockers are also increase by 50% your risk of suffering from gout-like acute joint pain due to calcium pyrophosphate crystal deposition (CPPD).
And achlorhydria itself (a condition in which the stomach does not produce hydrochloric acid, such as through taking H2 blockers long term) has been found to be associated with a near five-fold increase in your risk of developing gastric cancer.42
“Did magnesium deficiency help cause the abdominal aortic aneurysm in the first place?”
A couple of studies confirmed the association.
Patients with AAA have many of the same risk factors as patients with coronary artery disease (CAD), and I discussed the shared pathways in a recent Substack.
In 2021, Ito et al analysed serum magnesium of 100 patients with pre-dialysis chronic kidney disease stage 5. They found that higher Mg levels were significantly associated with a lower volume of abdominal aorta calcification.43
They called for further studies, but it is acknowledged to be a predictor of cardiovascular outcomes in coronary artery disease (CAD), especially of AAA. Chowdhury et al (2018) derived calcium scores from computed tomography (CT) scans of patients with either infrarenal (AAA, just below the kidneys) or descending thoracic aneurysms (TAA).44
They found that the odds ration (OR) for AAA and all cause mortality (2.246; 95% CI 1.591–9.476; p < 0.001) and cardiac mortality (1.321; 1.076–2.762; p = 0.003) was significantly associated with calcium score.
The association with TAA was even greater, over a six-fold and three-fold increase:
All cause mortality (6.444; 95% CI 2.574–6.137; p < 0.001) and cardiac mortality (3.456; 95% CI 1.765–4.654; p = 0.042).
Risk of cardiac morbidity increased more than two-fold: (2.128; 95% CI 1.973–4.342; p = 0.002).
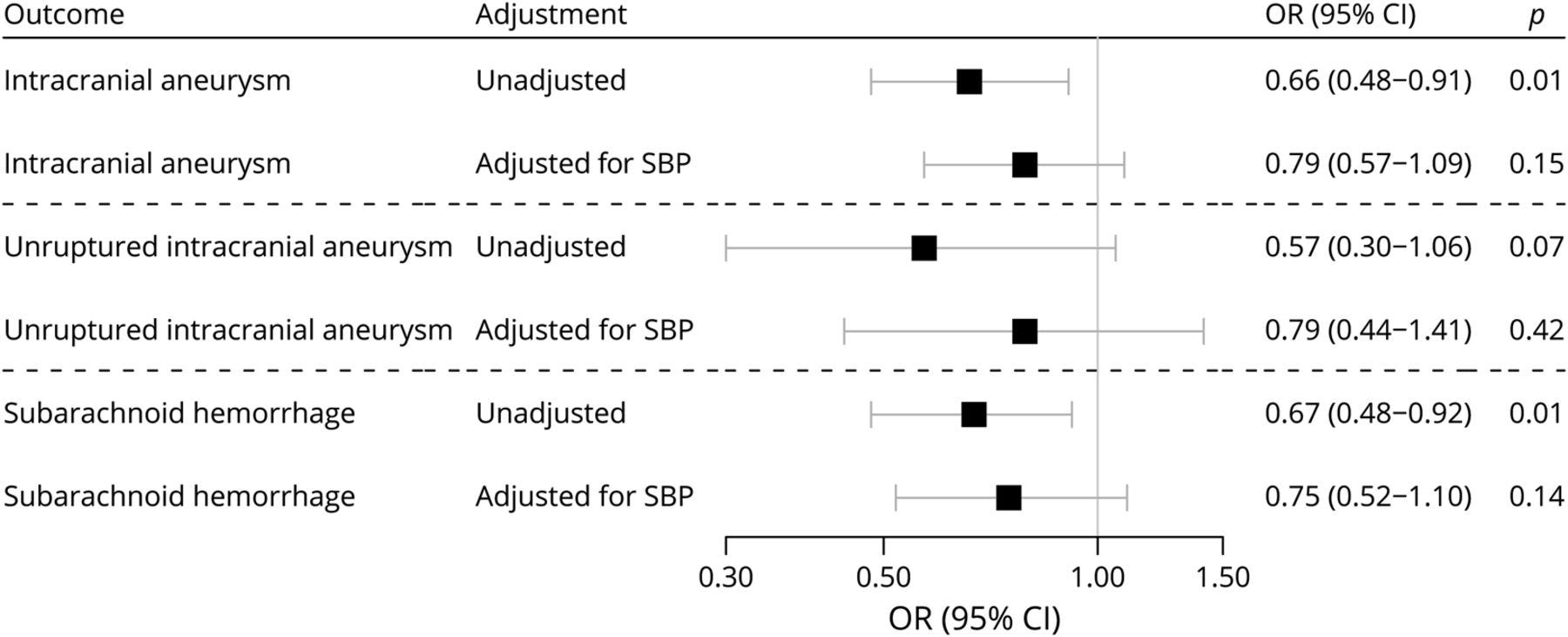
And also from 2021, Larsson & Gill conducted a Mendelian (i.e. genetic) randomization study into the association of serum magnesium with the risk of intracranial aneurysm.45 This is also known as a brain aneurysm or a cerebral aneurysm. A ruptured brain aneurysm is life-threatening:
…to our knowledge this is the first MR study to identify a potential causal association between serum magnesium concentrations and risk of intracranial aneurysm and aneurysmal subarachnoid hemorrhage.
…In addition to a blood pressure–lowering effect, increased magnesium concentrations may reduce the risk of intracranial aneurysm rupture by improving endothelial function4,5 and reducing oxidative stress.12
From: “Association of Serum Magnesium Levels With Risk of Intracranial Aneurysm A Mendelian Randomization Study” (2021)
In 2022, Ryu et al published a retrospective analysis of 1,006 Korean patients with acute ischemic stroke.46 The OR for a poor functional outcome was 2.15 (95% CI, 1.16–3.98; P=0.015). In other words, addressing your hypomagnesemia can halve your risk of a poor outcome from a stroke.
With minor strokes, the effects were even more striking, with severe Mg deficiency increasing your risk of a poor outcome over 4-fold (OR 4.2; 95% CI, 1.67–10.59; P=0.002).
In the cardioembolic stroke group, the adjusted OR was 3.41 (95% CI, 1.24–9.41; P=0.018).
Prevention of stroke in the first place also needs to be factored in, whether with poor outcomes or not. The authors recommended future research should further investigate the role of magnesium as a neuroprotective agent.
- Thrombosis
Also in 2022 but from Japan, Tonai et al conducted a retrospective observational study into the association between hypomagnesemia and coagulopathy in sepsis.47
Coagulation is a key mediator of poor sepsis outcomes and studies have found that being deficient in thrombin generation (a unique molecule that functions both as a procoagulant and anticoagulant) is associated with greater inpatient and 90-day mortality.48
Tonai et al investigated the link between serum magnesium levels and overt disseminated intravascular coagulation (DIC) at the time of ICU admission. DIC is a rare but serious condition that causes abnormal blood clotting throughout the body's blood vessels.
Their thresholds were:
Hypomagnesemia: < 1.6 mg/dL.
Normal serum magnesium: 1.6–2.4 mg/dL.
Hypermagnesemia: > 2.4 mg/dL.
They found that patients with hypomagnesemia had more coagulation and more DIC, with biomarkers including:
Percentages with DIC in each group were split 41.9% vs 20.6% vs 24.0% for hypomagnesemia vs normal serum Mg vs hypermagnesemia.
The risk of DIC for the hypomagnesemia group was increased by nearly 70% (OR 1.69; 95% confidence interval, 1.00–2.84; P = 0.048).
Most notably they found that hypomagnesemia was independently associated with DIC in patients with sepsis. In other words, magnesium deficiency itself and not the sepsis was likely responsible:
From: “Fig. 2. Coagulation parameters between different serum magnesium levels (hypomagnesemia, normal magnesium level, and hypermagnesemia) in sepsis. Box-and-whisker plot depicting a difference in coagulation parameters between different serum magnesium levels (hypomagnesemia [Hypo] vs. normal magnesium level [Normal] vs. hypermagnesemia [Hyper]) in patients with sepsis admitted to the ICU. Admission serum levels of (a) platelet count (104/μL); (b) fibrinogen (mg/dL); (c) PT-INR; (d) FDP (μg/mL); (e) AT III activity (%); (f) PC activity (%); (g) TAT (ng/mL); (h) PIC (μg/mL); (i) PAI-1 (ng/mL). Boxplots display median with first and third quartile, and whiskers indicate smallest and largest nonoutlier observations. *P-value < 0.05, comparison versus hypomagnesemia (Steel–Dwass test). Abbreviations: AT III, antithrombin III; FDP, fibrin degradation products; ICU, intensive care unit; PC, protein C; PIC, plasmin-α2 plasmin inhibitor complex; PT-INR, prothrombin time-international normalized ratio; TAT, thrombin-antithrombin complex; PAI-1, plasminogen activator inhibitor-1.” Source: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9685885/
DIC is one of the crucial complications of sepsis because it can lead to organ failure and death by causing microvascular thrombosis.
Mg supplements have also been shown to inhibit platelet-dependent thrombosis(PDT) in patients with coronary artery disease. In 1999 Shechter et al conducted a a randomized prospective, double-blind, crossover, and placebo-controlled study of 42 patients with CAD.49
37 men and 5 women were enrolled (mean age 68 +/- 9). They received aspirin and either 800-1200mg/day of magnesium oxide tablets or placebo. This is a curious choice as MgO has one of the lowest bioavailability scores, but even so, they found that it reduced occurrences of median PDT by 35% vs placebo. This was despite aspirin therapy in both groups:
Do magnesium deficiency-induced pathologies lead to increased rates of mortality? In 2016 Semsarian & Ingles published a paywalled editorial in the BMJ: “Preventing sudden cardiac death in athletes”.50
Guess what they didn’t recommend screening for?
The authors were called out for this major omission in a rapid response by Peter Lewis, a “General Practitioner with Special Interest In Integrative Medicine”:
Surprisingly, in their editorial, Preventing sudden cardiac death in athletes, Semsarian and Ingles did not mention the importance of magnesium and omega-3 fatty acids.
The link between magnesium deficiency and sudden cardiac death has been suggested by a substantial number of published studies over the past few decades. Data come from epidemiologic, autopsy, clinical, and animal studies. They suggest that: (1) Sudden death is common in areas where community water supplies are Mg-deficient. (2) Myocardial Mg content is low in people who die of sudden death. (3) Cardiac arrhythmias and coronary artery vasospasm can be caused by Mg deficiency and (4) Intravenous Mg reduces the risk of arrhythmia and death immediately after acute myocardial infarction (i). Further, magnesium is lost in sweat during strenuous exertion, exacerbating any pre-existing magnesium insufficiency or deficiency.
One such study by the somewhat appropriately named Kieboom et al (1986) analyzed the link between serum magnesium and the risk of death from coronary heart disease (CHD) and sudden cardiac death (SCD).51
9,821 participants (mean age 65 and 57% female) were followed up for a median of 8.7 years in the Rotterdam Study. They found that the hazard ratio for CHD mortality was reduced by a factor of 0.82 (95% CI 0.70–0.96) for each 0.1 mmol/L increase in serum magnesium level.
Further analysis showed that low serum Mg of <=0.80 mmol/L increased the risk of CHD mortality by 1.36 (95% CI 1.09–1.69) and SCD by 1.54 (95% CI 1.12–2.11).
It was also associated with accelerated subclinical atherosclerosis (increased carotid intima‐media thickness: +0.013 mm, 95% CI 0.005–0.020) and increased QT‐interval, mainly due to reduced heart rates.
After about 12 years the divergence in mortality rates for low vs high serum Mg and CHD and non-sudden CHD mortality increases markedly, almost exponentially:
In contrast, the increased risk of SCD remains fairly constant, but trends upward after about 4 years:
From: “Figure 2. Estimated cumulative probability curves for coronary heart disease mortality, nonsudden coronary heart disease mortality, and sudden cardiac death. Estimated cumulative probability curves are shown for coronary heart disease mortality (A), nonsudden coronary heart disease mortality (B), and sudden cardiac death (C) between different groups of serum magnesium levels, taking into account the competing risk of death by other causes. Low serum magnesium is defined as 0.34 to 0.80 mmol/L, medium serum magnesium (reference) as 0.81 to 0.88 mmol/L, and high serum magnesium as 0.89 to 1.74 mmol/L.” Source: https://www.ahajournals.org/doi/10.1161/jaha.115.002707
Management of hypomagnesaemia in primary care
Although advice to the general public is scant, its good to see this being circulated:
Key takes from an NHS guidance note for practitioners (not current clinical advice).52
Normal plasma magnesium concentration ranges from 0.70 - 1.05 mmol/L. Only about 1% total body magnesium is found in extracellular fluid; the remainder is in bone and soft tissue. About 25% of plasma magnesium is bound to albumin so high or low albumin concentrations will affect magnesium levels.
This is an interesting statement when you contrast it to the rapid onset of heart disturbances associated with the 100mg/day Western diet clinical trial. Are acute effects due to lack of buffering, and does it take many months to replete total body magnesium?
Changes in magnesium levels occur very slowly (over months or years).Serum magnesium does not always correlate with total body magnesium – it is possible to see a serum level within the reference interval, but a total body magnesium deficit with a chronic magnesium deficiency usually as a result of inadequate dietary magnesium. The reverse (a low serum level and normal total body magnesium) is also possible and is usually seen with drugs which increase excretion of magnesium.
Early signs of deficiency include loss of appetite, nausea, vomiting, fatigue, and weakness. As deficiency worsens, numbness, tingling, muscle contractions and cramps, seizures, personality changes, abnormal heart rhythms, and coronary spasms can occur. Severe deficiency can result in hypocalcaemia or hypokalaemia.
Magnesium deficiency has been associated with the following conditions:
Gastrointestinal loss, including malabsorption, malnutrition, Crohn's disease, coeliac disease
Chronic alcoholism
Poorly controlled type 2 diabetes
Renal disorders
Drug therapy – e.g. PPIs, diuretics, cisplatin, gentamicin, ciclosporin, foscarnet, amphotericin, pentamidine
The MHRA advise that prolonged use of PPIs has been associated with case reports of hypomagnesaemia, some serious. It suggests measuring magnesium levels before starting PPI treatment and periodically during prolonged treatment, especially in those who will take a PPI concomitantly with digoxin or drugs that may cause hypomagnesaemia (e.g. diuretics).
What does Dorset CCG recommend? Dorset CCG advises that magnesium levels should be measured in patients who are symptomatic and are likely to have diminished magnesium levels because of their therapy (e.g. long term PPIs and/or other medicines) and pre- existing conditions (Appendix One).
I will discuss bioavailability in the next Substack:
Robust evidence of the superiority of one oral magnesium preparation over another does not exist. Tolerability of a particular preparation may limit the dosage. Caution should be exercised when switching between magnesium preparations as magnesium preparations have differing bioavailability.
First line
Magnesium-L-aspartate (Magnaspartate®) is the preferred choice for treatment and prevention of magnesium deficiency in adults, adolescents and children from 2 years. Magnesium-L-aspartate (Magnaspartate®) is a 10 mmol sachet formulation to be mixed with water and for adults taken up to twice a day. It is the most cost effective licensed preparation available.
Second line
Magnesium glycerophosphate is available for patients unable to tolerate the magnesium-L-aspartate sachet formulation. Currently the only licensed magnesium glycerophosphate preparation is Neomag® (4 mmol chewable tablets). This is licensed in treatment and prevention of magnesium deficiency in adults, adolescents and children from 4 years.
All other magnesium preparations and salts (citrate) remain unlicensed. Magnesium glycerophosphate liquid 5 mmol/5mL (MagnaPhos®) is unlicensed but manufactured to GMP standards and currently the most cost effective liquid available for those unable to take the licensed preparations.
Their guidance does not follow dieticians advice to dose per Kg body weight/day and is certainly at the top end of the range:
1 mmol of elemental magnesium (Mg) = 24.3 mg of elemental Mg.
(From the atomic mass of Mg, = 24.3)
24mmol Mg = 583 mgof elemental Mg/day.
Dosing
The BNF states that for adults, magnesium may be given by mouth in a dose of 24mmol Mg daily in divided doses. See BNFc for children’s doses.
Thank you for reading DoorlessCarp’s Scientific Literature Reviews. This post is public so feel free to share it.
DoorlessCarp’s Scientific Literature Reviews is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
Scooby Couey and the gang expose the crooks controlling charitable research and advice
Disclaimer
This site is strictly an information website reviewing research into potential therapeutic agents. It does not advertise anything, or provide medical advice, diagnosis, or treatment. This site does not promote any of these as potential treatments or offer any claims for efficacy. Its content is aimed at researchers, registered medical practitioners, nurses, or pharmacists. This content is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website. Always consult a qualified health provider before introducing or stopping any medications as any possible drug interactions or effects will need to be considered.
Any extracts quoted in the previous article are for non-commercial research and educational purposes only and may be subject to copyright from their respective owners.
Naser SA, Abdelsalam A, Thanigachalam S, Naser AS, Alcedo K. Domino effect of hypomagnesemia on the innate immunity of Crohn’s disease patients.World J Diabetes. 2014;5(4):527-535. doi:10.4239/wjd.v5.i4.527
Song Y, Liu S. Magnesium for cardiovascular health: time for intervention.The American Journal of Clinical Nutrition. 2012;95(2):269-270. doi:10.3945/ajcn.111.031104
DiNicolantonio JJ, O’Keefe JH. Magnesium and Vitamin D Deficiency as a Potential Cause of Immune Dysfunction, Cytokine Storm and Disseminated Intravascular Coagulation in covid-19 patients.Mo Med. 2021;118(1):68-73. Accessed March 6, 2024. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7861592/
Kuang X, Liu C, Guo X, Li K, Deng Q, Li D. The combination effect of vitamin K and vitamin D on human bone quality: a meta-analysis of randomized controlled trials.Food Funct. 2020;11(4):3280-3297. doi:10.1039/C9FO03063H
Capozzi A, Scambia G, Lello S. Calcium, vitamin D, vitamin K2, and magnesium supplementation and skeletal health.Maturitas. 2020;140:55-63. doi:10.1016/j.maturitas.2020.05.020
Martín Giménez VM, Bergam I, Reiter RJ, Manucha W. Metal ion homeostasis with emphasis on zinc and copper: Potential crucial link to explain the non-classical antioxidative properties of vitamin D and melatonin.Life Sci. 2021;281:119770. doi:10.1016/j.lfs.2021.119770
DiNicolantonio JJ, O’Keefe JH, Wilson W. Subclinical magnesium deficiency: a principal driver of cardiovascular disease and a public health crisis. Open Heart. 2018;5(1):e000668. doi:10.1136/openhrt-2017-000668
Kostov K, Halacheva L. Role of Magnesium Deficiency in Promoting Atherosclerosis, Endothelial Dysfunction, and Arterial Stiffening as Risk Factors for Hypertension.Int J Mol Sci. 2018;19(6):1724. doi:10.3390/ijms19061724
Adameova A, Abdellatif Y, Dhalla NS. Role of the excessive amounts of circulating catecholamines and glucocorticoids in stress-induced heart disease.Can J Physiol Pharmacol. 2009;87(7):493-514. doi:10.1139/Y09-042
da Silva Costa R, Sainara Maia Fernandes T, de Sousa Almeida E, et al. Potential risk of BPA and phthalates in commercial water bottles: a minireview.Journal of Water and Health. 2021;19(3):411-435. doi:10.2166/wh.2021.202
Houston M. The Role of Magnesium in Hypertension and Cardiovascular Disease.J Clin Hypertens (Greenwich). 2011;13(11):843-847. doi:10.1111/j.1751-7176.2011.00538.x
Khan AM, Lubitz SA, Sullivan LM, et al. Low serum magnesium and the development of atrial fibrillation in the community: the Framingham Heart Study.Circulation. 2013;127(1):33-38. doi:10.1161/CIRCULATIONAHA.111.082511
Jolly K, Faulconer R, McEwan R, Becker H, Garnham A. The incidence of hypomagnesaemia following abdominal aortic aneurysm surgery.Ann R Coll Surg Engl. 2015;97(5):379-381. doi:10.1308/003588415X14181254790004
White CM. Ranitidine’s N-nitrosodimethylamine Problem May be Tip of the Iceberg.JAMA Network Open. 2021;4(1):e2035158. doi:10.1001/jamanetworkopen.2020.35158
Essrani R, Mehershahi S, Ravi SJK, et al. Famotidine induced hypomagnesemia leading to hypocalcemia.Oxf Med Case Reports. 2020;2020(1):omz133. doi:10.1093/omcr/omz133
Poynter D, Pick CR, Harcourt RA, et al. Association of long lasting unsurmountable histamine H2 blockade and gastric carcinoid tumours in the rat.Gut. 1985;26(12):1284-1295. Accessed March 12, 2024. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1433126/
Ito M, Yamaguchi M, Katsuno T, et al. Association between serum magnesium levels and abdominal aorta calcification in patients with pre-dialysis chronic kidney disease stage 5.PLOS ONE. 2021;16(6):e0253592. doi:10.1371/journal.pone.0253592
Chowdhury MM, Zieliński LP, Sun JJ, et al. Editor’s Choice – Calcification of Thoracic and Abdominal Aneurysms is Associated with Mortality and Morbidity.Eur J Vasc Endovasc Surg. 2018;55(1):101-108. doi:10.1016/j.ejvs.2017.11.007
Larsson SC, Gill D. Association of Serum Magnesium Levels With Risk of Intracranial Aneurysm.Neurology. 2021;97(4):e341-e344. doi:10.1212/WNL.0000000000012244
Tonai K, Katayama S, Koyama K, et al. Association between hypomagnesemia and coagulopathy in sepsis: a retrospective observational study.BMC Anesthesiol. 2022;22:359. doi:10.1186/s12871-022-01903-2
Winer LK, Salyer C, Beckmann N, Caldwell CC, Nomellini V. Enigmatic role of coagulopathy among sepsis survivors: a review of coagulation abnormalities and their possible link to chronic critical illness.Trauma Surg Acute Care Open. 2020;5(1):e000462. doi:10.1136/tsaco-2020-000462
Shechter M, Merz CN, Paul-Labrador M, et al. Oral magnesium supplementation inhibits platelet-dependent thrombosis in patients with coronary artery disease.Am J Cardiol. 1999;84(2):152-156. doi:10.1016/s0002-9149(99)00225-8
Kieboom BCT, Niemeijer MN, Leening MJG, et al. Serum Magnesium and the Risk of Death From Coronary Heart Disease and Sudden Cardiac Death.Journal of the American Heart Association. 5(1):e002707. doi:10.1161/JAHA.115.002707
Personal anecdote. My husband has been on a PPI for many years for very bad GERD. This was years ago. He then had small runs of premature ventricular tachycardia (PVCs) and the cardiologist couldn't figure out why. I suggested he was magnesium deficient but the cardiologist dismissed that suggestion. Nonetheless, hubby listened to his pharmacist wife, took magnesium and the PVCs resolved after about 4 months.
Microwave radiation stimulates voltage-gated calcium channels, and it's been hypothesized that magnesium's ability to act a a calcium channel blocker could be helpful for people who are EMR sensitive








2D, 1,25-dihydroxyvitamin D (biologically active form); 24,25(OH)2D, 24,25-Dihydroxyvitamin D; 25(OH)D, calciferol (inactive form); D2, vitamin D2 (from nonanimal sources); D3, vitamin D3 (from animal sources); DBP, vitamin D–binding protein; Mg, magnesium; VDR, vitamin D receptors.")




















's review of Meddling Kids")
Personal anecdote. My husband has been on a PPI for many years for very bad GERD. This was years ago. He then had small runs of premature ventricular tachycardia (PVCs) and the cardiologist couldn't figure out why. I suggested he was magnesium deficient but the cardiologist dismissed that suggestion. Nonetheless, hubby listened to his pharmacist wife, took magnesium and the PVCs resolved after about 4 months.
Microwave radiation stimulates voltage-gated calcium channels, and it's been hypothesized that magnesium's ability to act a a calcium channel blocker could be helpful for people who are EMR sensitive