17th June ‘22 (FLCC program, Management of Post-Vaccine Syndrome)
30th June ‘22 (Substack title renamed)
16th July ‘22 (Echinacea)
24th August ‘22 (Gynostemma pentaphyllum)
25th September ‘22 (Doxycycline; a focus on quercetin)
17th November ‘22 (Baicalin)
6th January ‘23 (Contents page. Browser support varies)
7th January ‘23 (Milk thistle/silymarin)
10th March ‘23: Link added to the Substack on therapeutic interactions.
Any extracts used in the following article are for non commercial research and educational purposes only and may be subject to copyright from their respective owners.
This is not an exhaustive list, has several contributors which unfortunately I can’t all credit and I will update the list accordingly as new therapies are presented. And please please add your own in the comments if you are shouting “why didn’t you mention Icelandic kelp extract??” or something like that, new studies are coming out all the time.
The “Long Covid’ condition is very complex, one size does not fit all but if we treat it as a combination of one or more pathologies comprising immune dysfunction, viral or spike protein persistence and oxidative stress then it explains why these therapies are effective for some and are gaining a following.
Combination therapies are also often more effective than a single therapeutic as effects can reinforce each other and multiple pathways can be targeted in a virtuous feedback cycle.
Additionally, as many of these therapeutics have strong antiviral efficacy and support the immune system in general (often including antitumor & autoimmunity moderating properties) a selection of them may be taken daily as prophylactics or at the first sign of infection.
Added 14th June ‘22:
Stacks
A combination of two or more nootropic substances is called a “stack."
Combining several compounds into a stack can have synergistic effects, such as in the cases of the ingredients in green tea and coffee.
For the full list and biochemistry research please read on and follow up the references, but here are a few basic stacks to get you started.
Although almost all are food or plant extracts with excellent safety profiles usual cautions apply as with any med.
Start by taking each in isolation at the lowest dose and take for a week, then start combining.
Don't expect instant miracles, these can take time to act systemically as your immune system and cellular health & metabolism recovers & gut biota stabilise. Antivirals start working within hours though.
Check with your doctor first if you are on any other meds for contraindications, have allergies to certain food groups etc and never just stop a med without consultation.
Check on webMD and other sites for cautions etc. These are good places to start:
Vitamin K2, MK-7, “fermented” or extracted from Natto for trans isomer. Even better with 5-10mg piperine. Take 200mg+ per day with meal or fatty food.
Take with D, magnesium, zinc, (ideally zinc with copper) as these are complementary for calcium management: out of your cardiovascular system and back in to teeth & bones eg via a daily multivitamin mineral sup. Zinc is also an essential complement to zinc ionophores like hydroxychloroquine & quercetin (hat-tip to the late Dr. Vladimir Zelenko's protocols).
Daily antiviral, immune & autoimmune health:
500mg - 2000mg milk thistle with 80% silymarin. Take at same time with:
Q10 30mg+ for cardiovascular & muscles.
Resveratrol 250-500mg +
Daily or weekly:
Hemp or CBD 1 gram = 1 teaspoon dried leaves as a tea or as oil do not exceed 60-70mg in total per day.
For joint pain/RA: Glucosamine sulphate 750mg+ and ideally with Chondroitin 75mg+ twice daily for at least 6 weeks.
Turmeric as above is also broad spectrum in efficacy. Take with 5-10mg piperine.
Further antiviral support when you get symptoms of an infection, early as possible ideally:
Quercetin 500-1000mg +
- Take quercetin with vitamin C and zinc, as above, for synergistic effects.
Artemisia is consumed on a daily basis in many African countries as an effective prophylactic against malaria & HIV.
Add to the above stack berberine or goldenseal 1000mg (750-2000 range). Ivermectin if you can get it but Berberine is just as good by many accounts.
Or/and at another part of the day Sweet Wormwood, Artemisia annua (NOT toxic Common Wormwood, A. absinthium) as 1 teaspoon dried leaves in porridge, as tea, or as infusion. It's bitter so add peppermint or fennel if needed.
Tincture, added to tea:
Take 0.7-2.0mL two to four times per day of a 1:4 tincture (in 50% alcohol).
Infusion:
To make an infusion, pour 1 cup boiling water over 1 teaspoon of dried leaf and infuse for 10-15 minutes. For therapeutic use it is recommended to drink 2 to 4 cups a day.
Echinacaea by tincture eg added to tea:
2.5ml, 3 times a day up to 10ml.
N-Acetyl Cysteine (NAC), 600mg once or twice a day. My advice is to keep back until you are infected because it can stop the ROS induced apoptosis of cancer cells by chemotherapy, Ivermectin & Quercetin.
Quick guide to buying Quercetin, Berberine or Baicalin
If its not a yellow-gold colour then it probably isn’t a high strength concentrate, buyer beware. Berberine is also very bitter.
Colour pallet varies depending on manufacturer but should not be whitish:
Quercetin
Berberine
Baicalin
I bookmarked the bones of this in May ‘21 in case it might help someone?
Although useful for turning down the immune system (ie anti-inflammatory) general advice is try to avoid long term use of corticosteroids as these can lead to cardiovascular disease & osteoporosis.
Instead, CBD, D & Glucosamine are natural immune regulators and are considered preferential to corticosteroids long term.
I would also add for mitochondrial function Metformin, Resveratrol via 500mg supplements or/and red wine & black grapes (Malbec, Cabernet Sauvignon, Merlot), an antioxidant rich diet, NAC, Q10, K2 sources and Ivermectin (IVM) or Hydroxychloroquine (HCQ), 10ml high omega-3 fish oils, quercetin to clear any remnant RNA spike sources. HCQ helps neurological issues too, + glucosamine as an anti cancer agent and to reduce elevated inflammatory cytokine levels.
As an aside it's no coincidence that at least 6 of the above have been cited as having significant anti-cancer properties: Metformin, Resveratrol, CBD, IVM, HCQ & Glucosamine. Turmeric is a seventh.
@ShemNehm contributed the following:
"There are lots of papers, that look at anti-oxidants as a potential therapeutic for Covid, e.g:
Perusing the list above, you'll see the usual suspects: Vitamins C&D, NAC, Thymoquinone, Quercetin, Turmeric, etc. I was wondering. I wonder if Astaxanthin could be added to the list:
“Vaccine Injury: Long COVID and inflammatory vaccine reaction share the same cause Spike Protein. People are going to need to know about natural remedies. This thread will offer some papers with advice. First luteolin.
Long-COVID syndrome-associated brain fog and chemofog: Luteolin to the rescue
* As ever this is not medical advice, you will need to check for suitability for you, do your own additional research for dosing, mode of action and for interactions plus consult a licensed medical practitioner who knows your full medical history. For example these may suppress other meds you are on or make a condition worse.
Therapeutic mechanisms in detail
Added 10th March ‘23: Includes baicalein, quercetin, ivermectin and lactoferrin.
In vitro antioxidant activity of olive leaf extract (Olea europaea L.) and its protective effect on oxidative damage in human erythrocytes (2018)
Olive leaves are an important source of antioxidants, such as phenolic compounds and flavonoids, which display effective antioxidant activity when various methodologies are used. OLE inhibits the action of reactive species that participate in cellular biochemical processes and protects human erythrocytes against oxidative damage. These results show that olive leaves are effective antioxidant in biological systems, suggesting that their intake may be related to prevention of oxidative stress in vivo, with consequent health benefits. Moreover, OLE have the potential to be used as natural antioxidants in preservation of food products, pharmaceuticals and cosmetics, in which chain reactions mediated by free radicals result in oxidative alterations.
The compounds responsible for the antioxidant effects of OLE are not yet fully understood. Thus, additional studies are required for identification and isolation of these compounds and their efficiency. In addition, further in vivo studies should be performed to confirm the results obtained so far.
Role of Mitochondria in the Mechanism(s) of Action of Metformin
Metformin is a drug from the biguanide family that is used for decades as the first-line therapeutic choice for the treatment of type 2 diabetes. Despite its worldwide democratization, owing to its clinical efficacy, high safety profile and cheap cost, the exact mechanism(s) of action of this anti-hyperglycemic molecule with pleiotropic properties still remains to be fully elucidated. The concept that metformin would exert some of its actions though modulation of the mitochondrial bioenergetics was initially forged in the 50s but undeniably revived at the beginning of the twenty-first century when it was shown to induce a weak but specific inhibition of the mitochondrial respiratory-chain complex 1. Furthermore, metformin has been reported to reduce generation of reactive oxygen species at the complex 1 and to prevent mitochondrial-mediated apoptosis, suggesting that it can protect against oxidative stress-induced cell death. Nevertheless, despite some recent progress and the demonstration of its key role in the inhibition of hepatic gluconeogenesis, the exact nature of the mitochondrial interaction between the drug and the complex 1 is still poorly characterized. Recent studies reported that metformin may also have anti-neoplastic properties by inhibiting cancer cell growth and proliferation, at least partly through its mitochondrial action. As such, many trials are currently conducted for exploring the repositioning of metformin as a potential drug for cancer therapy. In this mini-review, we discuss both historical and more recent findings on the central role played by the interaction between metformin and the mitochondria in its cellular mechanism of action.
Resveratrol induces mitochondrial biogenesis in endothelial cells (2009)
Abstract
Pathways that regulate mitochondrial biogenesis are potential therapeutic targets for the amelioration of endothelial dysfunction and vascular disease. Resveratrol was shown to impact mitochondrial function in skeletal muscle and the liver, but its role in mitochondrial biogenesis in endothelial cells remains poorly defined. The present study determined whether resveratrol induces mitochondrial biogenesis in cultured human coronary arterial endothelial cells (CAECs). In CAECs resveratrol increased mitochondrial mass and mitochondrial DNA content, upregulated protein expression of electron transport chain constituents, and induced mitochondrial biogenesis factors (proliferator-activated receptor-coactivator-1alpha, nuclear respiratory factor-1, mitochondrial transcription factor A). Sirtuin 1 (SIRT1) was induced, and endothelial nitric oxide (NO) synthase (eNOS) was upregulated in a SIRT1-dependent manner. Knockdown of SIRT1 (small interfering RNA) or inhibition of NO synthesis prevented resveratrol-induced mitochondrial biogenesis. In aortas of type 2 diabetic (db/db) mice impaired mitochondrial biogenesis was normalized by chronic resveratrol treatment, showing the in vivo relevance of our findings. Resveratrol increases mitochondrial content in endothelial cells via activating SIRT1. We propose that SIRT1, via a pathway that involves the upregulation of eNOS, induces mitochondrial biogenesis. Resveratrol induced mitochondrial biogenesis in the aortas of type 2 diabetic mice, suggesting the potential for new treatment approaches targeting endothelial mitochondria in metabolic diseases.
Resveratrol: A Double-Edged Sword in Health Benefits (2018)
Abstract
Resveratrol (3,5,4′-trihydroxy-trans-stilbene) belongs to polyphenols’ stilbenoids group, possessing two phenol rings linked to each other by an ethylene bridge. This natural polyphenol has been detected in more than 70 plant species, especially in grapes’ skin and seeds, and was found in discrete amounts in red wines and various human foods. It is a phytoalexin that acts against pathogens, including bacteria and fungi. As a natural food ingredient, numerous studies have demonstrated that resveratrol possesses a very high antioxidant potential. Resveratrol also exhibit antitumor activity, and is considered a potential candidate for prevention and treatment of several types of cancer. Indeed, resveratrol anticancer properties have been confirmed by many in vitro and in vivo studies, which shows that resveratrol is able to inhibit all carcinogenesis stages (e.g., initiation, promotion and progression). Even more, other bioactive effects, namely as anti-inflammatory, anticarcinogenic, cardioprotective, vasorelaxant, phytoestrogenic and neuroprotective have also been reported. Nonetheless, resveratrol application is still being a major challenge for pharmaceutical industry, due to its poor solubility and bioavailability, as well as adverse effects. In this sense, this review summarized current data on resveratrol pharmacological effects.
Covid and/or spike protein exposure can lead to or exacerbate amyloidosis, accelerating dementia & Parkinsons:
Resveratrol for Alzheimer’s disease (2017)
Abstract
The amyloid hypothesis suggests that the progressive accumulation and deposition of central nervous system amyloid with aging is the proximate cause of Alzheimer’s disease (AD). Thus, targeting molecular mechanisms of aging may represent a viable treatment approach. Caloric restriction prevents diseases of aging, including AD, in animal models, perhaps by activation of sirtuins. The sirtuins (such as mammalian SIRT1) are deacetylases that link energy balance (NAD+/NADH) to regulation of gene transcription. Resveratrol is a potent activator of SIRT1, and thus may mimic caloric restriction to prevent diseases of aging. We conducted a randomized, double blind, placebo-controlled, phase II trial of resveratrol for individuals with mild to moderate AD. Resveratrol (1) is detectable in cerebrospinal fluid (at low nanomolar levels), (2) is safe and well tolerated, (3) alters AD biomarker trajectories, (4) preserves blood–brain barrier integrity, and (5) modulates the CNS immune response. Further studies are needed to determine the safety and efficacy of resveratrol and the validity of this approach in the treatment and prevention of AD and other diseases of aging.
Quite an old paper but this kind of immunosuppression could be very useful to target autoimmunity & proinflammatory cytokines, but note that part of glucosamines’ autoimmune suppressing benefits are because it is a general immune suppressor, it may be contraindicated if you are already immunosuppressed.
Immunosuppressive Effects of Glucosamine (2002)
Glucosamine is a naturally occurring derivative of glucose and is an essential component of glycoproteins and proteoglycans, important constituents of many eukaryotic proteins. In cells, glucosamine is produced enzymatically by the amidation of glucose 6-phosphate and can then be further modified by acetylation to result in N-acetylglucosamine. Commercially, glucosamine is sold over-the-counter to relieve arthritis. Although there is evidence in favor of the beneficial effects of glucosamine, the mechanism is unknown. Our data demonstrate that glucosamine suppresses the activation of T-lymphoblasts and dendritic cells in vitro as well as allogeneic mixed leukocyte reactivity in a dose-dependent manner. There was no inherent cellular toxicity involved in the inhibition, and the activity was not reproducible with other amine sugars. More importantly, glucosamine administration prolonged allogeneic cardiac allograft survival in vivo. We conclude that, despite its documented effects on insulin sensitivity, glucosamine possesses immunosuppressive activity and could be beneficial as an immunosuppressive agent.
However, a recent report by Gouze et al. (27) demonstrated glucosamine-dependent inhibition of NF-κB activity in rat chondrocytes and IL-1β1bioactivity by up-regulation of the type II IL-1 decoy receptor.
Serratiopeptidase, A Serine Protease Anti-Inflammatory, Fibrinolytic, and Mucolytic Drug, Can Be a Useful Adjuvant for Management in COVID-19 (2021)
SEPD may be a promising therapeutic candidate for repurposing due to its immunomodulatory, anti-inflammatory, mucolytic, antifibrotic, antithrombotic, antiviral, and fibrinolytic properties. SEPD, being an age-old, inexpensive, natural, and tolerated drug, may be a better alternative over other mucolytics or adjuvant with other drugs particularly in individuals with symptoms of sputum or mucus or productive cough. Recently, the animal models of COVID-19 become available that may facilitate preclinical evaluations to distinguish whether these candidate compounds are likely to become effective drugs. Though, the suggestion on the use in COVID-19 remains inconclusive until the proof of concept preclinical and clinical studies undertaken. But the potential of SEPD can’t be overlooked ascribed to its promising possible benefits in COVID-19. It may be able to limit fatal complications, including pulmonary and cardiovascular diseases, and improve the prognosis of COVID-19. However, it is important to highlight that, to date, no studies have demonstrated the experimental or clinical effects of SEPD in COVID-19.
And another contraindication is if you have a G6PD deficiency (a hereditary genetic condition), in which case you should not use methylene blue at all.
Lemon Balm, which has many active ingredients such as quercetin and phenolics with antioxidant, antifungal, antibacterial and potent anticancer properties. May be infused in tea, which is how I take it at around 1 gram per cup:
Antitumoral effects of Melissa officinalis on breast cancer in vitro and in vivo (2012)
Abstract
Background: There is a long standing interest in the identification of medicinal plants and derived natural products for developing cancer therapeutics. Here we investigated the antiproliferative properties of Melissa officinalis (MO) from Turkey on breast cancer.
Methods: MO extracts were studied for cytotoxicity against breast cancer cell lines (MCF-7, MDA-MB-468 and MDA-MB-231). In vitro apoptosis studies were performed by annexin V staining and flow cytometry analyses. Immunohistochemistry for Ki-67 and caspase 7 in the tumoral tissue sections of DMBA-induced mammary tumors in rats was also performed, along with TUNEL assays to detect apoptotic cells. In vivo anticancer activity testing was carried out with reference to inhibition of growth of DMBA induced mammary tumors in rats.
Results: MO showed cytotoxicity against three cancer cell lines, inducing increase in Annexin-positive cells. Expression of caspase-7 protein and TUNEL positive cells were much higher in rats treated by MO, compared with the untreated control group, while expression of Ki-67 was decreased. Furthermore, in vivo studies showed that mean tumor volume inhibition ratio in MO treated group was 40% compared with the untreated rats.
Conclusion: These results indicated that MO extrcts have antitumoral potential against breast cancer.
Melissa officinalis Extract Induces Apoptosis and Inhibits Migration in Human Colorectal Cancer Cells (2020)
Abstract
Colorectal cancer (CRC) is one of the most frequently diagnosed cancers worldwide. Lifestyle-related factors, such as diet, are associated with the development of CRC. Cumulating evidence indicates noticeable chemopreventive effects of phytochemicals on CRC, suggesting that drinking herbal tea potentially reduces the risk of distal colon cancer via its antiproliferative and anti-angiogenic activities. We examine the antitumor effects of nine components frequently found in herbal tea and uncover the underlying molecular mechanism. Among them, the hot water extract of Melissa officinalis (MO) exhibited the highest anticancer activity on CRC cells. We revealed that MO reduced cell proliferation, induced cell cycle arrest at the G2/M phase, triggered caspase-dependent apoptotic cell death, and inhibited cell migration ability by modulating the epithelial–mesenchymal transition in HCT116 CRC cells. To examine the metabolite composition in the MO hot water extract, we applied mass spectrometry-based analysis and identified 67 compounds. Among them, the phenolic compounds, including lignans, phenylpropanoids, and polyketides, are widely found in natural products and possess various bioactivities such as anti-inflammatory, antioxidation, and anticancer effects. The results indicate that herbal tea consumption benefits CRC prevention and management.
Hypericum perforatum and Its Ingredients Hypericin and Pseudohypericin Demonstrate an Antiviral Activity against SARS-CoV-2 (2022)
Abstract
For almost two years, the COVID-19 pandemic has constituted a major challenge to human health, particularly due to the lack of efficient antivirals to be used against the virus during routine treatment interventions. Multiple treatment options have been investigated for their potential inhibitory effect on SARS-CoV-2. Natural products, such as plant extracts, may be a promising option, as they have shown an antiviral activity against other viruses in the past. Here, a quantified extract of Hypericum perforatum was tested and found to possess a potent antiviral activity against SARS-CoV-2. The antiviral potency of the extract could be attributed to the naphtodianthrones hypericin and pseudohypericin, in contrast to other tested ingredients of the plant material, which did not show any antiviral activity. Hypericum perforatum and its main active ingredient hypericin were also effective against different SARS-CoV-2 variants (Alpha, Beta, Delta, and Omicron). Concerning its mechanism of action, evidence was obtained that Hypericum perforatum and hypericin may hold a direct virus-blocking effect against SARS-CoV-2 virus particles. Taken together, the presented data clearly emphasize the promising antiviral activity of Hypericum perforatum and its active ingredients against SARS-CoV-2 infections.
Cannabidiol Inhibits SARS-CoV-2 Replication and Promotes the Host Innate Immune Response (preprint, 2021)
Abstract
The rapid spread of COVID-19 underscores the need for new treatments. Here we report that cannabidiol (CBD), a compound produced by the cannabis plant, inhibits SARS-CoV-2 infection. CBD and its metabolite, 7-OH-CBD, but not congeneric cannabinoids, potently block SARS-CoV-2 replication in lung epithelial cells. CBD acts after cellular infection, inhibiting viral gene expression and reversing many effects of SARS-CoV-2 on host gene transcription. CBD induces interferon expression and up-regulates its antiviral signaling pathway. A cohort of human patients previously taking CBD had significantly lower SARSCoV-2 infection incidence of up to an order of magnitude relative to matched pairs or the general population. This study highlights CBD, and its active metabolite, 7-OH-CBD, as potential preventative agents and therapeutic treatments for SARS-CoV-2 at early stages of infection.
Summary sentence:
Cannabidiol from the cannabis plant has potential to prevent and inhibit SARS-CoV-2 infection
"We have already observed the replication of SARS-CoV-2 virus in bacteria many times"🤔
What this means is that the virus is replicating in your gut bacteria or maybe acting as a latent pool of infection, affects your microbiota and possibly playing a part in long Covid. Watch those carbs!
SARS-CoV-2 and its bacteriophage abilities (and how to address it, and heal yourself)
Berberine has been researched widely as it has many different therapeutic properties, too many in fact to list here properly and a literature review in it's own right was warranted.
Several of the other therapeutics here regulate the same pathways so much of the research applies to ivermectin, quercetin, resveratrol etc too. Berberine must rate as a “supertherapeutic”.
Therapeutic properties of Berberine
A literature review (2022)
Abstract
This Substack is a scientific literature review of much of the current research into the therapeutic benefits of berberine.
It explores the rational for finding effective antivirals against COVID-19 as a matter of some urgency.
Berberine as a compound is described along with common plant based sources of the drug.
Significant antiviral activity has been demonstrated against alphaviruses, cytomegalovirus, herpes simplex, COVID-19, SARS, RSV, hepatitis-C and influenza, including at higher viral loads in the later course of infection where it may be too late to use other treatments effectively.
Anticancer activity by interaction with several pathways has been evidenced. The most interesting of these is by upregulation of the key tumor suppressor p53. Efficacy against myeloma, non-Hodgkin lymphoma and as a potential antitumor agent for Primary effusion lymphoma (PEL) is also indicated.
A significant reduction of inflammatory cytokines in COVID-19 patients and other in vitro studies is discussed, along with a reduction of pulmonary fibrosis in COVID-19 patients.
Evidence for the efficacy of berberine in type 2 diabetes is presented, and related positive results when used to manage obesity.
Suppression of mast cell mediated allergic responses has been demonstrated in animal trials and in vitro.
Limited but significant evidence of reduction of hypertension was found from trials involving rats and randomised control trials of humans, along with favourable blood sugar markers, but more research is needed.
Berberine is beneficial for MS sufferers too by suppressing autoimmune responses according to a humanised mouse and other studies, and attenuation of the sphingosine kinase 1 (Sphk1) signalling pathway may also be beneficial for inhibiting tumorigenesis.
Berberine or a derivative can inhibit amyloidosis by disrupting at least 2 pathways: reducing neutrophil elastase levels and by disrupting cytochrome induced ROS generation. Amyloidosis and a possible correlation with cardiovascular incidents and excess deaths is explored.
A synergistic association with Ferulic acid and with the chemotherapeutic agent cisplatin is discussed, and finally bioavailability, warnings and dosing guidance is provided.
This is just for one mighty herb and I'm only reviewing a fraction of the research conducted to date.
Abstract
This Substack is a scientific literature review of much of the research relevant to treating COVID-19 and transfection sequelae using the therapeutic herb Artemisia annua, including citations from other topic themed bibliography reviews.
Malarial treatments are discussed because the dosing techniques, toxicity and efficacy are relevant and well researched.
It explores the rational for finding effective antivirals against COVID-19 as a matter of some urgency, including a presentation of correlative anecdotal and official data on the harm being caused by currently adopted public health policy.
The botanical history of the herb Artemisia annua and its principle bioactive components and minerals are detailed.
A passage submitted by contributing author Charles Wright is featured: “THE WORLD HEALTH ORGANIZATION'S POSITION ON THE USE OF WHOLE LEAF AND CHEMICAL DERIVATIVES OF A. ANNUA”. This reports on how the stance of the WHO has changed in the last 20 or so years from supporting scientifically-proven traditional medicine to one of collaborating with social media platforms to suppress the discussion of the potential of whole leaf A. annua to treat SARS2.
A paper is reviewed that found strong anti-HIV activity with low toxicity when taken as a tea. As with malaria patients, this a very popular low cost and accessible treatment in Africa, with research studies findings of efficacy comparable to allopathic medications, although results varied according to sample sets used. No particular compound could be isolated that was responsible for this.
Research papers published into antiviral activity against COVID-19 are reviewed. One study concluded: “Results suggest that oral consumption of A. annua hot-water extracts (tea infusions), could provide a cost-effective therapy to help stave off the rapid global spread of these variants...” Another paper found via in vitro studies that later variants required greater artemisinin concentrations to achieve the same degree of viral inhibition.
Of particular note, greater efficacy than from hydroxychloroquine was indicated against mild to moderate COVID in one study. Another study concludes: “Artemisinin showed significant inhibition of 3CL protease activity but not Spike/ACE-2 binding.”
The water soluble artemisinin derivative artesunate shows particular promise as a compound which demonstrates anticancer, antimalarial and anti-amyloid properties, amongst others.
The next section further explores Artemisinin compounds and their anti-cancer properties. Research found multiple modes of action and synergistic effects for many of the therapeutic actions of A. annua.
Positive efficacy of artemisinin and its derivatives for the treatment of type 2 diabetes mellitus are reviewed. Once again, multiple modes of action are responsible.
A study by Kiss et al (2021) demonstrated that the artemisinin derivative artensuate attenuates levels of an amyloid precursor protein in an Alzheimer's disease (AD) mouse model.
A paper exploring therapeutic efficacy in the experimental model of multiple sclerosis using mice found that “The brain histology shows the absence of plaque formation in the artemisinin treated group.”
Another study found that dihydroartemisinin (DHA),an active form of artemisinin, alleviates pulmonary hypertension (PH) through the ELAVL2/miR-503/PI3K/AKT pathway (ie an autoimmune signalling pathway involving a microRNA), which might provide a basis for new therapeutic strategies.
The review concludes with dosing guidance from multiple sources, any contraindications, advice on growing, harvesting, drying and making tea infusions from A. annua and a further contribution by Charles on his recommendations for future research strategies.
Vaccine injury (COVID) and risk of severe outcome post vaccine; FLCCC program that has been devised to mitigate the risk of severe outcome, especially blood clots post COVID mRNA vaccine
Marik, Kory etc.
Dr. Paul Alexander
Management of Post-Vaccine Syndrome
Major public health authorities do not recognize post-COVID-vaccine injuries; and there is no specific ICD classification code for this disease. However, while no official definition exists, a temporal correlation between a patient receiving a COVID-19 vaccine and beginning or worsening of clinical manifestations is sufficient to diagnose as a COVID-19 vaccine-induced injury when the symptoms are unexplained by other concurrent causes.
Since there are no published reports detailing the management of vaccine-injured patients, our treatment approach is based on the postulated pathogenetic mechanism, clinical observation, and patient anecdotes. Treatment must be individualized according to each patient’s presenting symptoms and disease syndromes. It is likely that not all patients will respond equally to the same intervention; a particular intervention may be life saving for one patient and totally ineffective for another.
Early treatment is essential; it is likely that the response to treatment will be attenuated when treatment is delayed.
Program and with the input of your clinician (3 pages in order):
This Substack is a scientific literature review of research into the therapeutic benefits of three Echinacea species. A PubMed 10 year search for “Echinacea” returned 467 results. Some of the more cited research is presented here for review:
Echinacea purpurea was shown to broadly inhibit coronaviruses and SARS-CoV-2 in vitro. In 2021 Nicolussi et al used PCR testing to compare the rates of infection and viral loads in adults and children administered 2,400mg and 1,200mg respectively of Echinaforce extract tincture over 4 months vs the control with excellent results: viral loads in nasal secretions were significantly reduced by 98.5%.
For preventing and treating the common cold a controversial meta-analysis from 2014 by Karsch-Volk et al concluded there were either statistically insignificant or minor benefits.
In 2011, Hudson & Vimalanathan posted their meta analysis of reviews Echinacea—A Source of Potent Antivirals for Respiratory Virus Infections. They found that all strains of human and avian influenza viruses tested, including a Tamiflu resistant strain as well as herpes simplex, RSV and rhinoviruses (a common cold virus) were very sensitive to E purpurea preparations. Their results suggested intracellular inhibition and significant viricidal activity, including by inhibition of replication, although effects were sometimes weak at non-cytotoxic concentrations.
Fusco et al (2010) found that Echinacea-treated mice had lower systemic and pulmonary KC (human IL-8) and IL-10 levels and lower systemic IFN-γ levels following influenza infection. They suggested that E. purpurea alters the clinical course of influenza infection in mice through modulation of cytokines and not direct antiviral activity. Although aerial parts of the plant did not show antiviral activity, they found that root extracts did in fact demonstrate this.
Another finding was that “Echinaforce” inhibits mucin secretion, one of the most discomforting symptoms and the cause of coughs, sore throat or even bronchitis.
A further study by Vimananathan et al in 2017 indicated that virus-induced bacterial adhesion and cytokine storms associated with respiratory infections could be inhibited by E purpurea.
A 2009 murine study into the reduction of latent herpes simplex virus type-1 (HSV-1) reinfections demonstrated efficacy when taken as a prophylactic.
In 2007, a paper by Pillai et al further supports polysaccharides as being potent immunostimulants. Water soluble, but not fat-like extracts from all parts of the plant all produced substantial immunostimulatory activity.
Upregulation of NF-kB is a marker for infection. In 2008, Matthias et al identified 2 different alkyamides in Echinacea root extract, one of which stimulated the immune response, the other modulated it.
Prophylaxis appears important for reducing viral levels. Sharma, Schoop & Hudson (2009) used a standardised Echinacea preparation (Echinaforce) and concluded that symptoms may be reduced at any stage of infection: “under real life conditions of Echinacea consumption, the virus-induced stimulation of pro-inflammatory cytokines can be effectively reversed or alleviated.”
A study from 2007 by Zhai et al concluded that all three species promoted T-cell proliferation, anti-viral interferons and innate & adaptive immune responses, but E. angustifolia or E. pallida may have more anti-inflammatory potential.
A 2017 study by Chiou et al. (only abstract available) researched antioxidant, antidiabetic, and antihypertensive properties. They found that both chlorogenic acid and caffeic acid demonstrated high ACE-inhibitory activity. Their in vitro results suggested that E. purpurea extract and CAD have good potential for managing hyperglycemia and hypertension.
An interesting study by Tsai et al (2012) found that “cichoric acid has a strong growth-inhibitory effect against colon cancer cells, presumably resulting from the reduced telomerase activity and the induction of apoptosis.”
A human clinical trial by Yotsawimonwat et al (2010) showed an increase in overall skin hydration and a reduction in skin wrinkles by 10%-14% when using Echinacea as either a face cream or gel.
Contraindications, interactions with chemotherapeutic drugs, bioavailability and dosage recommendations are then considered.
Therapeutic properties of Gynostemma pentaphyllum (jiaogulan)
A literature review
Abstract
This Substack is a scientific literature review of research into the therapeutic properties of Gynostemma pentaphyllum, also known as the immortality herb, five-leaf ginseng, poor man's ginseng, miracle grass, fairy herb, sweet tea vine, gospel herb, and southern ginseng. A PubMed 10 year search for “Gynostemma pentaphyllum” returned 298 results. Some of the more cited research is presented here for review:
From a paper published in 2021, Rehan and Shafiullah conducted an in silico molecular docking binding analysis of 60 saponins with the COVID-19 main protease 6LU7 Mpro.
Although they found that 34 saponins were more effective than hydroxychloroquine, chloroquine or nelfinavir, as this was software based analysis the results need confirming in vitro and in vivo, but it is extremely promising research.
Okoye et al (2012) investigated the antiviral effects of extracts of G. pentaphyllum against yellow fever virus infectivity of chicken egg embryos and mice, and the percentage inhibition of viral induced hemagglutination (ie red blood cells clumping together). Results were somewhat encouraging, especially as even today there are still no specific anti-viral drugs to treat yellow fever.
From the same year, 2012, the same author Okoye worked with Nworu to study “Inhibition of HIV-1 lentiviral particles infectivity by Gynostemma pentaphyllum extracts in a viral vector- based assay”. As with the previous study they performed solvent extraction from leaf powder using ethyl ether (EG), methanol (MG) or water (AG).
Again the results from this in vitro research pointed to potential antiviral drugs that could be developed using extracts from the herb.
Sornpet et al (2017) investigated the antiviral activity of five Asian medicinal plant crude extracts against H5N1 avian influenza virus.
In 2020, Shaito et al published a comprehensive review of the ethnopharmacological therapeutic potentials and medicinal properties against cardiovascular diseases (CVDS) of four widely used plants: Ginseng, Ginkgo biloba, Ganoderma lucidum, and Gynostemma pentaphyllum.
This review is unusual, so far, in that it considers available clinical trials data as well as safety, toxicity and side effects.
(2012), Li et al extracted 2 acidic polysaccharides and tested against cancer cells in vivo and in vitro. After using alcohol to remove lipid they used water at 90°C for 2 hours, x 3, to extract from dried stem and leaf material.
Cancer types: Human chronic myeloid leukemia K-562, breast adenocarcinoma MCF-7, colon adenocarcinoma HT-29, hepatocellular carcinoma HepG2 and mouse melanoma B16 cell lines.
For in vivo studies they used tumor bearing mice and melanoma injected male rats, feeding them or injecting the polysaccharides and various statistically significant results are presented.
In 2010, Peng, Zhou and Zhang investigated the antitumor activities of dammarane triterpene saponins from a different species, Bacopa monniera.
I reference this study due to the commonality of the dammaranes with G. pentaphyllum.
This herb is also known as water hyssop, waterhyssop, brahmi, thyme-leafed gratiola, herb of grace, and Indian pennywort. Their in vivo studies in mice demonstrated tumor inhibition of up to 90%.
Moving on to 2016 and Li et al performed an in vitro study into the anticancer activity of a nonpolar fraction from G. pentaphyllum.
They provided evidence for significant anticancer activities from previously unreported, non-dammarane compounds. This provides further evidence of broad spectrum anti-tumor efficacy and the potential for developing novel anticancer agents.
Also from 2016, Li et al published a comprehensive review of the literature associated with G. pentaphyllum (GpM) and anti-cancer activities and mechanisms of action.
The most recent paper in this review of anti-cancer properties is from 2021, by Liu et al. They investigated how gypenosides of G. pentaphyllum can induce apoptosis of renal cancer tells through decreasing the phosphorylation level of Akt and mTOR in the PI3K/Akt/mTOR signaling pathway.
In 2010, Choi et al reported neuroprotective effects of ethanol extracts from G. pentaphyllum in a rat model of Parkinson’s disease.
And in 2018, Dong et al published research into how gypenosides reverse depressive behaviour by inhibiting hippocampal neuroinflammation.
Then in 2022, Wang et al conducted an in silico analysis to screen for compounds that can inhibit neurologically damaging signalling pathways associated with Alzeimer’s disease (AD).
From 2020, Wang et al conducted an in vitro investigation in to how dammarane-Type saponins from G. pentaphyllum can prevent hypoxia-induced neural injury through activation of ERK, Akt, and CREB pathways.
Hong et al (2018) conducted a biomedical investigation integrated with an in silico assay into how G. pentaphyllum can attenuate the progression of nonalcoholic liver disease in mice.
In 2017, Wong et al demonstrated how G. pentaphyllum saponins attenuate inflammation in vitro and in vivo by inhibition of NF-κB and STAT3 signaling. This is also another tumorigenic pathway and one of the key pathways mediated by cellular exposure to spike protein due to COVID-19 infection or transfection.
Back in 2006, Megalli, Davies and Roufogalis conducted an in vivo investigation using rats into how extracts of G. pentaphyllum can improve the serum ratios of cholesterols, triglyceride, blood sugar and the insulin resistance profile.
In 2020, Yin et al reported on ten new dammarane-type saponins with hypolipidemia activity from G. pentaphyllum herbal tea.
Huang et al (2022) published a review focusing on the prebiotic and therapeutic aspects of saponins and polysaccharides of jiaogulan tea, and the indirect anticancer effects of a healthy gut biome.
Bioavailability, contraindications, interactions with chemotherapeutic drugs and dosage recommendations are then considered, to conclude the review.
This is not to be taken as a prophylactic ever and always under medical supervision but is included here due its antibacterial, antiviral and anticancer properties.
Repurposing of the antibiotic Doxycycline as an antiviral and anti-cancer therapeutic
A literature review
Abstract
This review begins with a brief introduction to doxycycline as a drug: its uses, side effects, history and chemical formula with the 5-ringed structure typical of the tetracyclines.
Doxycycline and its iron chelation mechanisms and effects are then described.
In 2021, Faure et al performed in vitro experiments to investigate the synergistic interactions between five tetracyclines and tobramycin with an iron chelator (CP762) against two reference strains and nine clinical isolates of Pseudomonas aeruginosa from cystic fibrosis patients.
They found that as it binds with high affinity to iron this inhibited its antibacterial effects by competing with the magnesium binding site on the bacterial ribosome. The addition of another iron chelator, CP762, synergistically restored the magnesium bridge binding.
In 1999 Alkawash et al appeared to find lactoferrin/doxycycline antibacterial synergy, and by a large margin of 32 to 64 fold against B. cepacia.
In 2015, Wu et al investigated its effects in vitro on the replication of vesicular stomatitis virus.
Of particular note here for also treating long covid/vaccine sequalae is that doxycycline acts as both an antiviral and an anticancer therapeutic agent by the induction of expression of the key tumor suppressor p53.
Induction of p53 expression by doxycycline is then discussed in more detail. Son et al (2009) conducted an in vitro investigation and concluded that the tumor suppressive effects on pancreatic cancer cells were due to the activation of proapoptotic genes, inhibiting IL-8 expression, and suppression of antiapoptotic genes.
In 2020, Mosquera-Sulbaran and Hernández-Fonseca published a review on the use of tetracycline as an anti COVID-19 therapeutic.
2 clinical trials using doxycycline and ivermectin are then discussed. No results were available from the first of these, but from the second the only participants to die of COVID-19 were 3 from the placebo group of 200. Duration and severity of symptoms in the treatment group were also significantly reduced.
Three papers investigating iron chelation, inhibition of tumors and metastasis are reviewed. Buss et al (2003) recognized the potential of using iron chelation in cancer therapy and their possible synergistic effects.
From 2013, Richardson et al review how the iron chelator DFO can inhibit key signalling pathways which induce epithelial mesenchymal transition (EMT) in pancreatic cancer and other tumors. EMT is described.
A paper by Morales and Xue (2021) reviews the targeting of iron metabolism in cancer therapy.
Ubiquitination is described, as is evidence for the HIF inhibitory effects of both lactoferrin and ivermectin. This is important for working synergistically with doxycycline to help avoid resistance from cancer cells.
To complete this review, four papers discuss the anticancer properties of doxycycline.
In 1998, Fife et al found that, in vitro, doxycycline can significantly inhibit the growth of prostate and breast cancer tumors by the inhibition of matrix metalloproteinases (MMPs) and induction of apoptosis.
From 2016, Zhang et al conducted an in vitro study using human breast cancer cell lines.
A paper by Zhu et al (2017) conducted an in vitro investigation into how doxycycline synergizes with the chemotherapeutic drug doxorubicin to inhibit the proliferation of castration-resistant prostate cancer cells, a condition that was previously untreatable.
And from 2019, Markowska et al conducted a review into the repositioning of doxycycline, salinomycin, monensin and ivermectin as cancer drugs.
To conclude this Substack, dosing and contraindications for doxycycline monohydrate are considered.
Appendix:
A Computational Study of Ivermectin and Doxycycline Combination Drug Against SARS-CoV-2 Infection;
What’s stopping doctors repurposing generic medicines? Answer - not a lot
Dr Lynn Fynn cautions against taking this long term as it does interact with the gut biome. This may be a positive thing or a negative for some, so I have removed it from the daily prophylactic list.
But if you have completed a course of antibiotics, suffer from gut dysbiosis or leaky gut syndrome it may help restore the balance of your gut biome and I take it daily without issue:
Quercetin improves gut dysbiosis in antibiotic-treated mice (2020)
Abstract
The diversity and activity of the gut microbiota residing in humans and animals are significantly influenced by the diet. Quercetin, one of the representative polyphenols in human diets, possesses a wide range of biological properties. The aim of this study was to investigate the prebiotic effects of quercetin in antibiotic-treated mice. Gut dysbiosis was successfully induced in mice by treatment with an antibiotic cocktail. Gas chromatography and 16S rDNA high-throughput sequencing techniques were used to investigate short-chain fatty acid content and gut microbial diversity and composition. The results showed that quercetin supplementation significantly improved the diversity of the gut bacterial community in antibiotic-treated mice (P < 0.05). Meanwhile, intestinal barrier function was also recovered remarkably as indicated by a decrease in the content of serum d-lactic acid and the activity of serum diamine oxidase (P < 0.05). The length of intestinal villi and mucosal thickness were also significantly increased in response to quercetin treatment (P < 0.05). Furthermore, the production of butyrate in faeces was enhanced significantly in quercetin-treated mice (P < 0.05). In conclusion, quercetin is effective in recovering gut microbiota in mice after antibiotic treatment and may act as a prebiotic in combatting gut dysbiosis.
Quercetin modulates the gut microbiota as well as the metabolome in a rat model of osteoarthritis (2021)
Abstract
Although the mechanism of osteoarthritis (OA) has been widely studied and the use of quercetin for OA therapy is well documented, the relevant characteristics of the microbiome and metabolism remain unclear. This study reports changes in the gut microbiota and metabolism during quercetin therapy for OA in a rat model and provides an integrative analysis of the biomechanism. In this study, the rats were categorized into 3 different groups: the OA model, quercetin treatment, and control groups. The OA rats was conducted using a monoiodoacetate (MIA) injection protocol. The rats in the quercetin group received daily intragastric administration of quercetin from day 1 to day 28. Stool samples were collected, and DNA was extracted. We used an integrated approach that combined the sequencing of whole 16S rRNA, short-chain fatty acid (SCFA) measurements and metabolomics analysis by mass spectrometry (MS) to characterize the functional impact of quercetin on the gut microbiota and metabolism in a rat model of OA. The use of quercetin partially abrogated intestinal flora disorder and reversed fecal metabolite abnormalities. Compared with the control rats, the OA rats showed differences at both the class level (Clostridia, Bacteroidia, and Bacilli) and the genus level (Lactobacillus and unidentified Ruminococcaceae). Acetic acid, propionic acid and 24 metabolites were significantly altered among the three groups. However, the changes were significantly abrogated in quercetin-treated OA rats. Consequently, this study provided important evidence regarding perturbations of the gut microbiome and the function of these changes in a potential new mechanism of quercetin treatment.
Keywords: Osteoarthritis; gut microbiota; metabolome; quercetin; regulation.
Quercetin metabolism by fecal microbiota from healthy elderly human subjects (2017)
Abstract
Quercetin is a polyphenol found in food that has numerous health benefits. This study investigated the relationship between quercetin metabolism, gut microbiota composition, and dietary intake in elderly Japanese subjects. A food frequency questionnaire was used to assess dietary intake during the week prior to stool sample collection. Fecal suspensions from 56 subjects were anaerobically incubated with quercetin and fecal microbiota composition was analyzed by next-generation sequencing. Inter-individual variations in quercetin concentration and fecal microbiota composition at family level suggested differences in microbial quercetin metabolism. The abundance of Sutterellaceae (r = -0.292) and Oscillospiraceae (r = -0.334) was negatively correlated whereas that of Fusobacteriaceae (r = 0.361) and Enterobacteriaceae (r = 0.321) was positively correlated with quercetin concentration. Niacin (r = -0.313), vitamin B6 (r = -0.297), vitamin B12 (r = -0.266), vitamin D (r = -0.301), and ratio of animal protein to total protein (r = -0.27) were also negatively correlated with quercetin concentration. Bacterial abundance was positively or negatively related to intake of food components. This is the first report describing the relationship between fecal quercetin metabolism, human microbiota, and dietary intake in the elderly.
Quercetin also improves bioavailability and efficacy of berberine:
% CDR = % cumulative drug release.
From Quercetin as Natural Bioavailability Modulator: An Overview (2020):
…In conclusion, quercetin could be successfully utilized as bioenhancer to improve ex vivo permeability of berberine chloride, which would be expected to improve its bioavailability and reduce the dose resulting in improved patient compliance.
…increased permeability of berberine chloride during pre-treatment study with quercetin might have resulted from the quercetin, which inhibited the efflux pump P-gp. Briefly, inhibition of efflux pump P-gp by quercetin might be duly responsible for permeability enhancement of berberine chloride.
…Based on these data, it could be suggested that 10 mg of quercetin for 30 minutes pretreatment time was optimum to increase the permeability of poorly permeable berberine chloride up to a maximum of 90.91% ± 1.66% CDR.
Chinese Skullcap (Scutellaria baicalensis) and Baicalin
Therapeutic properties of Baicalin
A literature review
Abstract
This Substack is a scientific literature review of much of the current research into the therapeutic benefits and mode of action of baicalin and its associated flavonoids.
Zhao et al (2019) published a systematic and comprehensive overview on the traditional usages, botany, phytochemistry, pharmacology, pharmacokinetics and toxicology of Scutellaria baicalensis Georgi.
The Ukranians have known for at least 12 years that Baicalin (among other flavonoids) has furin inhibitory effects. Translated from Russian, a paper by Kibirev et al from back in 2010 is reviewed.
Four years later and in 2016 the Palladin Institute published an updated paper on the latest research into furin inhibitors, their structure and efficiency.
Nhoek et al investigated flavonoids from Scutellaria baicalensis and their inhibitory activity against PCSK9 expression in a paper from 2018.
In 2016 Bao et al conducted in vivo studies and found a strong correlation between SREBP-1 levels and breast cancer tumor differentiation and metastasis.
Mahboobnia et al performed a literature review of the pathology linked to PCSK9 in 2021. In contrast to suppressing apoptosis, PCSK9 appears to promote apoptosis of nerve cells in the cerebellum.
In 2016, Moore et al published a paper on how to optimise the extraction efficiency of baicalin, its anticancer effects, bioavailability and nanotechnology.
They found that ultrasound-assisted extraction (UAE), which uses cavitation, is an efficient way to extract the compound using a solvent of 40% ethanol at 60°C, and combing this technique with heat reflux extraction (HRE) increase the yield and efficiency further still.
They then described modes of action at inhibiting cancer cells, which is promising as an alternative to the very common side effects of radiotherapy and chemotherapy.
In 2017, Lin et al summarised which natural compounds from herbs can induce autophagy in cancer cells.
Shen et al (2013) describe how TRAF2 is an NF-κB-activating oncogene in epithelial cancers, which is why induced degradation by baicalin can provide us with another anti-cancer signalling pathway.
Hua et al (2019) describe RelB/p52 associated autophagy in detail, with reference to cervical cancer.
Some miRNAs have oncogenic or tumor suppressive properties. In 2021 Ge et al performed in vitro based microarray analysis of the effects of baicalin on miRNAs involved with breast cancer, which is another of the signalling pathways that it uses to inhibit tumorigenesis.
2016, and Liu et al conducted a review of research into the effects of baicalein on different cancer types and the possible mechanisms involved. The abstract and diagram alone are extremely informative.
In 2000, Chan et al conducted an in vitro study into the effects of baicalin on several prostate cancer cell lines. They found that the responses to baicalin were different among different cell lines, and that 50% inhibition of DU145 cells (considered a standard prostate cancer cell line) occurred at concentrations of 150μmol or above. LNCaP cells were the most resistant (androgen-sensitive human prostate adenocarcinoma cells).
Xu et al (2018) conducted in vitro and in vivo investigations into the hepatoprotective effects of silybin when co-administered with baicalein, using rats as a model. They found that baicalein improved the oral bioavailability of silybin with enhanced liver protective effects, inhibition of breast cancer resistance protein (BCRP) and suppression of multidrug resistance protein 2 (MRP2).
In 2000, Li et al performed an in vitro investigation into how baicalin flavonoids can inhibit HIV-1 infection at the level of viral entry.
They used 96-well tissue culture plates in the presence or absence of BA (Baicalin, 7-glucuronic acid,5,6-dihydroxyflavone) at designated concentrations, and repeated the experiments at least 3 times before analysing the group data using a Student’s t test, and found that baicalin can inhibit viral entry and replication, but not block binding to CD4 T-cells via glycoprotein 120 (gp120).
It has been confirmed by replicable BLAST analysis that the spike protein trimer includes HIV inserts homologous with gp41 and the cytotoxic & neurotoxic glycoprotein 120 (gp120).
It is also known that spike S1 has binding affinity for neuropilin 1 (Nrp1) receptors and nicotinic acetylcholine receptors, thus providing mechanisms to facilitate endocytosis into several cell types including neurons, much as the HIV virus does.
A paper by Lee et al also makes the connection between gp120 and amyloidosis via signalling pathways including iNOS and COX-2. All this is of potential relevance to the diagnosis and treatment of the condition and as COX-2 is linked to tumorigenesis and amyloidosis is linked to Alzheimer's disease, although cause and effect is controversial. Baicalin demonstrates neuroprotective properties, including by targeting the above iNOS and COX-2 inflammatory signalling pathways. Woo et al conducted an in vitro investigation (2006) and found that it mediates this by inhibiting COX-2 gene expression.
Alvarez et al (2007) also conducted an in vitro study of gp120 and found that it induces COX-2 promoter transcription through NF-kappaB activation in astrocytoma cells.
In 2015, Noh et al were studying the effects of baicalin on oral pharmacokinetics of caffeine in rats, specifically for interactions with CYP3A4 activity as marked by ethoxyresorufin O-deethylase (EROD), methoxyresorufin O-demethylase (MROD), benzyloxyresorufin O-debenzylase (BROD) and p-nitrophenol hydroxylase and erythromycin N-demethylase.
Baicalin was suspended in corn oil and fed to the rats with oral baicalin reaching its maximum concentration in plasma 8 hr after administration. Plasma concentration was then determined and found to be well below the concentrations used in a previous study. Plasma concentrations were in fact very low because it is converted quickly to other metabolites, meaning that certain CYP drug interactions would not be contraindicative.
A study by Yu et al in 2022 found that baicalin attenuates amyloid β oligomers induced memory deficits and mitochondria fragmentation through regulation of PDE-PKA-Drp1 signalling.
Parkinson’s disease. In 2019 Tu et al used a compound called 6-OHDA to induce the disease in rats. 6-hydroxydopamine is a kind of nerve agent that induces lesions in the brain, the resulting loss of dopamine produces Parkinson’s like symptoms which can be used as control against rats also administered baicalin.
They concluded that baicalin has significant protective effect on 6-OHDA-induced PD rats, which may play a protective role through an antioxidant, promoting the release of neurotransmitters and regulating the metabolism of N-acetyl aspartate and glutamate.
In 2012, Lu et al used mice bearing pancreatic tumor grafts which had been fed a baicalin supplemented diet. They found that some of the baicalin gets methylated to oroxylin A (OA) and its conjugates in various organs during absorption, and some of these have anti-tumor properties. In fact the anti-tumor effects in this study were so pronounced that “only 3 out of 6 mice treated with SB extract grew tumors large enough to be analyzed”. This study showed that baicalin or related metabolites may accumulate in plasma, tumor xenografts, and pancreas, liver, lung, and other tissues in vivo.
A paper by Ha et al (2012) is paywalled but also found that the breakdown product of baicalin, oroxylin A (OA) inhibits COX-2 as well as decreasing PGE2 levels in HT-29 human colon cancer cells.
In addition to the above, research by Chen, Yang & Lee (2000) added to our knowledge about the effects of oroxylin A.
Regarding antiviral properties, a patent was filed in 2009 for Baicalin as a treatment for SARS infection.
And in 2020 Su et al published a preprint of their research findings from investigating the protease inhibition of SARS-CoV-2 by baicalin and baicalein. The cell-based antiviral activity of baicalin or baicalein is superior to most of the reported compounds and that of baicalein is close to those of chloroquine (EC50: 1.13 μM; SI > 88) and remdesivir (EC50: 0.77 μM; SI > 129).
Shuanghuanglian (Chinese: 双黄连), a traditional Chinese medicine and its uses and pharmacology are then discussed.
In 2021, Ni et al published their findings from a randomized clinical trial of the effects of Shuanghuanglian against COVID-19.
They found that although the time to disease recovery was not reduced the viral load was significantly lower and pneumonia associated inflammation was significantly reduced. They do suggest that time to recovery may have been skewed due to patient transfers and waiting times before being randomly selected for trial.
In 2018 Bhattacharjee & Dey published a literature review discussing phytomelatonin or plant based sources of melatonin, and S. baicalensis is a source of the hormone.
At up to 7µg/g S. baicalensis is not a rich source of melatonin but it is worth considering as 3 grams/day could be enough to reach the physiological dose threshold for some people and synergism tends to amplify any effects.
In 1994 Zaidan et al found that only 20 micrograms was enough to have an effect.
In 2017 Jin, Huang and Zhu collected tissue samples from 6 female patients with endometriosis, cultured the endometrial stromal cells and exposed some of them to baicalein, with control cells for comparison. They found that baicalein may suppress the viability of human endometrial stromal cells through the NF-κB signaling pathway in vitro, and may induce apoptosis and promote cell cycle arrest at the G0/G1 phase. Thus, baicalein may provide a novel treatment option for endometriosis.
Liang et al (2019) induced ulcerative colitis (UC) in rats and treated it using baicalin, baicalein, or a combination of the two. They found that the high baicalin content of YSR (Young Scutellaria baicalensis ratio of baicalin and baicalein) exhibited the best treatment effects.
Treatment of ME/Chronic Fatigue Syndrome (CFS). Various sufferers of the syndrome have reported increased energy levels after taking extracts of S. baicalensis, which was attributed to baicalin.
In 2019 Ishfaq et al investigated the antagonistic effects of baicalin on infected chicken lungs by the restoration of energy metabolism and found a significant improvement.
Zhang et al (2015) found that baicalin has significant potential as an anti-inflammatory agent for the treatment of autoimmune diseases such as multiple sclerosis (MS) by preventing Th1 and Th17 cell differentiation via the STAT/NFκB signalling pathway.
Building on previous research, in 2018 another team of Chinese researchers, Xu et al, used dextran sodium sulfate (DSS) to induce colitis in mice and found that baicalein and baicalin downregulated STAT4 transcription in colon epithelial cells, thus exhibiting therapeutic effects on autoimmune diseases by regulating cell proliferation.
Moving on to 2021, and Wang et al reported on how baicalin protects the blood-brain barrier from injury mediated by lipopolysaccharide (LPS) using a mouse model.
Of particular interest for the treatment of demyelinating diseases like MS or peripheral neuropathy, in 2022 Ai et al found that, using a neonatal mouse model, baicalin promotes myelin production and regeneration by activating the PPARγ signal pathway and also confirmed that BA is an effective natural product for the treatment of demyelinating diseases.
In our final paper on autoimmunity, also from 2022, Wang et al conducted a literature review of Scutellaria baicalensis georgi as a promising candidate for the treatment of autoimmune diseases.
Dosing, contraindications and administration in a clinical setting are then considered to conclude the review.
Silybum marianum is a species of thistle. It has various common names including milk thistle, blessed milkthistle, Marian thistle, Mary thistle, Saint Mary's thistle, Mediterranean milk thistle, variegated thistle and Scotch thistle (though not to be confused with Onopordum acanthium or Cirsium vulgare). This species is an annual or biennial plant of the family Asteraceae. This fairly typical thistle has red to purple flowers and shiny pale green leaves with white veins. Originally a native of Southern Europe through to Asia, it is now found throughout the world.
Chemistry
Traditional milk thistle extract is made from the seeds, which contain approximately 4–6% silymarin. The extract consists of about 65–80% silymarin (a flavonolignan complex) and 20–35% fatty acids, including linoleic acid. Silymarin is a complex mixture of polyphenolic molecules, including seven closely related flavonolignans (silybin A, silybin B, isosilybin A, isosilybin B, silychristin, isosilychristin, silydianin) and one flavonoid (taxifolin). Silibinin, a semipurified fraction of silymarin, is primarily a mixture of 2 diastereoisomers, silybin A and silybin B, in a roughly 1:1 ratio.
Cancer Research UK putting the telescope to their blind eye:
In 2019, Cancer Research UK stated: "We need a lot more research with reliable clinical trials before we can be sure that milk thistle will play any part in treating or preventing cancers."
Some claim that it slows the growth of some types of cancer, including breast and prostate cancer.
It is possible that milk thistle may play a part in treating liver disease and some types of cancer. But we need a lot more research with larger numbers of people first. Reliable clinical trials can find out how useful milk thistle might be in preventing or treating cancer.
And no, they didn’t see fit to initiate these trials themselves.
I guess it depends who pays your bills?
From 2022 and Koltai et al give a great summary of its role in cancer treatments:
Role of Silymarin in Cancer Treatment: Facts, Hypotheses, and Questions
Abstract
The flavonoid silymarin extracted from the seeds of Sylibum marianum is a mixture of 6 flavolignan isomers. The 3 more important isomers are silybin (or silibinin), silydianin, and silychristin. Silybin is functionally the most active of these compounds. This group of flavonoids has been extensively studied and they have been used as hepato-protective substances for the mushroom Amanita phalloides intoxication and mainly chronic liver diseases such as alcoholic cirrhosis and nonalcoholic fatty liver. Hepatitis C progression is not, or slightly, modified by silymarin. Recently, it has also been proposed for SARS COVID-19 infection therapy. The biochemical and molecular mechanisms of action of these substances in cancer are subjects of ongoing research. Paradoxically, many of its identified actions such as antioxidant, promoter of ribosomal synthesis, and mitochondrial membrane stabilization, may seem protumoral at first sight, however, silymarin compounds have clear anticancer effects. Some of them are: decreasing migration through multiple targeting, decreasing hypoxia inducible factor-1α expression, inducing apoptosis in some malignant cells, and inhibiting promitotic signaling among others. Interestingly, the antitumoral activity of silymarin compounds is limited to malignant cells while the nonmalignant cells seem not to be affected. Furthermore, there is a long history of silymarin use in human diseases without toxicity after prolonged administration. The ample distribution and easy accessibility to milk thistle-the source of silymarin compounds, its over the counter availability, the fact that it is a weed, some controversial issues regarding bioavailability, and being a nutraceutical rather than a drug, has somehow led medical professionals to view its anticancer effects with skepticism. This is a fundamental reason why it never achieved bedside status in cancer treatment. However, in spite of all the antitumoral effects, silymarin actually has dual effects and in some cases such as pancreatic cancer it can promote stemness. This review deals with recent investigations to elucidate the molecular actions of this flavonoid in cancer, and to consider the possibility of repurposing it. Particular attention is dedicated to silymarin's dual role in cancer and to some controversies of its real effectiveness.
Silymarin has been investigated and proposed for the treatment of many different diseases, from Alzheimer dementia 54 to SARS 2 Covid-19, including diabetes, 55 diabetic complications,56–58 hyperlipidemia, and hypercholesterolemia,50–61 among others. However, in the last 15 years, the main focus has been cancer.
Silymarin and Cancer
The first observation of silymarin's possible benefits in cancer is the 1991 publication by Mehta and Moon. 118 They showed that silymarin could act as a preventive (antipromoter) of cancer in mouse mammary glands treated with DMBA (dimethylbenzanthracene) and TPA (tetradecanoylphorbol acetate). The treatment protocol they employed made it possible to differentiate whether the chemoprevention worked at the initiation stage of carcinogenesis (DMBA phase) or during promotion (TPA phase). A 1991 review on the advances in pharmacological studies of silymarin by Rui, 119 did not mention anticancer activities. But in 1994, Agarwal et al 120 performed a study on skin treated with TPA confirming the protective effect of this flavonoid against tumor promotion. Silymarin protected against induction of ornithine decarboxylase by TPA. Ornithine decarboxylase inhibition protects against tumor promotion. A protective effect of silymarin was also found in colon and small intestine adenocarcinoma cells induced by 1,2-dimethylhydrazine. 121 Silymarin and its components also inhibit beta-glucuronidase. 122
Valenzuela and Garrido 123 proposed 3 levels for silymarin's action in experimental animals:
(a) as an antioxidant, by scavenging prooxidant free radicals and by increasing the intracellular concentration of the tripeptide glutathione;
(b) through a regulatory action of cell membrane permeability and increase in its stability against xenobiotic injury;
(c) through nuclear expression, by increasing ribosomal RNA synthesis, by stimulating DNA polymerase I, and by exerting a steroid-like regulatory effect on DNA transcription.
Silymarin also inhibits rat liver cytosolic glutathione S-transferase, 124 although this function does not clearly hint towards anticancer activity. On the other hand, silymarin scavenges reactive oxygen species as noted above, and inhibits arachidonic acid metabolism in human cells, 125 has antiinflammatory effects similar to those of indomethacin, 126 protects skin against carcinogenic agents127,128 and ultraviolet radiation.129–131These publications strongly suggest a cancer-preventive activity and silymarin is slowly emerging as an anticancer drug. For example, Scambia et al 132 tested the antiproliferative activity of silymarin on human ovarian and breast cancer cell lines and found a growth-inhibiting effect on both. Silymarin also showed synergism with the commonly used anticancer compounds doxorubicin and cisplatin.
In DU145, prostate carcinoma cells, silymarin showed inhibition of Erb1 (eukaryotic ribosome biogenesis protein 1) signaling and G1 arrest. 133 In MDA-MB 486 breast cancer cells, G1 arrest was found due to increased p21 and decreased CDKs activity. 134 In advanced human prostate carcinoma cells, silymarin decreased ligand binding to Erb1 135 and NF-kB expression was strongly inhibited by silymarin in hepatoma cells, 136 as well as in histiocytic lymphoma, HeLa and Jurkat cells. 137
According to Zi and Agarwal, low doses of silymarin inhibited ERK1 and ERK2 Map kinases in a skin cancer cell line (human epidermoid carcinoma A431) and at higher doses activated MAPK/JNK1. This means that at lower doses the effect was antiproliferative and at higher doses proapoptotic.138
Treating prostate carcinoma cells with silymarin the levels of PSA were significantly decreased and cell growth was inhibited through decreased CDK activity and induction of Cip1/p21 and Kip1/p27.139
Silymarin has also been shown to have a variety of other protective effects in various cell types, such as anti-COX2 and anti-IL-1α activity, 140 antiangiogenic effects through inhibition of VEGF secretion, upregulation of Insulin like Growth Factor Binding Protein 3 (IGFBP3), 141 and inhibition of androgen receptors. 142In leukemia HL-60 cells, silymarin inhibited proliferation and induced differentiation into monocytes in a dose-dependent manner. 143Another important effect of silymarin in cancer is the downregulation of the STAT3 pathway which was seen in many cell models. STAT3 is active in many types of cancer and is associated with poor prognosis and resistance to treatments.144–146Telomerase activity is another important factor in promoting carcinogenesis and evading senescense, thus inducing cancer cell immortality; silymarin has the ability to decrease telomerase activity in prostate cancer cells.147
This literature review from 2021 by Palit et al provides some dosage guidance and calls for more studies. Silymarin has antiviral, immunomodulatory, antiinflammatory, antioxidant, antiplatelet, and anticoagulant properties. Not only does it inhibit viral replication, it can help prevent clotting and cytokine storm related pathologies:
Phyto‐pharmacological perspective of Silymarin: A potential prophylactic or therapeutic agent for COVID‐19, based on its promising immunomodulatory, anti‐coagulant and anti‐viral property
Abstract
Coronavirus disease 2019 (COVID‐19) triggered by a new viral pathogen, named severe acute respiratory syndrome Coronavirus‐2 (SARS‐CoV‐2), is now a global health emergency. This debilitating viral pandemic not only paralyzed the normal daily life of the global community but also spread rapidly via global travel. To date there are no effective vaccines or specific treatments against this highly contagious virus; therefore, there is an urgent need to advocate novel prophylactic or therapeutic interventions for COVID‐19. This brief opinion critically discusses the potential of Silymarin, a flavonolignan with diverse pharmacological activity having antiinflammatory, antioxidant, antiplatelet, and antiviral properties, with versatile immune‐cytokine regulatory functions, that able to bind with transmembrane protease serine 2 (TMPRSS2) and induce endogenous antiviral cytokine interferon‐stimulated gene 15, for the management of COVID‐19. Silymarin inhibits the expression of host cell surface receptor TMPRSS2 with a docking binding energy corresponding to −1,350.61 kcal/mol and a full fitness score of −8.11. The binding affinity of silymarin with an impressive virtual score exhibits significant potential to interfere with SARS‐CoV‐2 replication. We propose in‐depth pre‐clinical and clinical review studies of silymarin for the development of anti‐COVID‐19 lead, based on its clinical manifestations of COVID‐19 and multifaceted bioactivities.
Chemically silymarin is a polyphenolic flavonolignan complex of seven closely related derivatives (silybin A, silybin B, isosilybin A, isosilybin B, silychristin, isosilychristin, and silydianin) with one flavonoid taxifolin.
Contemporary literature reveals that silymarin modulates virus‐specific and nonspecific T‐cell proliferation as a potential immunomodulator (Johnson, He, Osuchowski, & Sharma, 2003), and elicits antiinflammatory effects via suppression of IFN‐γ and IL‐10 production (Adeyemo et al., 2013). Moreover, silymarin had significant antiviral potential (Liu, Jassey, Hsu, & Lin, 2019), and is a well‐known hepatoprotective, antioxidant, and anticoagulant with promising antiinflammatory activity (Delmas, 2020). Silymarin along with its derivatives, natural and chemical, have shown profound antiinflammatory activity by significant suppression of TNF‐α, IL‐6, IFN‐γ, and IL‐4 from bronchoalveolar lavage and lung macrophages in asthma and chronic obstructive pulmonary diseases (Dobiasová et al., 2020; Nasab, Saghazadeh, & Rezaei, 2020). Currently, a potential antiinflammatory drug Acalabrutinib has been recruited for the treatment of lung injury in severe COVID‐19 patients with hypoxia and fibrotic damage, caused by the massive hyper inflammation due to activation of macrophage and endothelial cells from cytokine storm (Roschewski et al., 2020). It is interesting to note that silymarin has better protection (73.29% reduction) against inflammatory cytokine IL‐1β (Toklu et al., 2008), compared to the standard antiinflammatory agents like Acalabrutinib, which demonstrates a 50% reduction of IL‐1β in the CLP mice model. Current literature reveals that the suppressive activity of silymarin and acalabrutinib against pro‐inflammatory cytokines TNF‐α and IL‐6 are interestingly comparable (O'Riordan et al., 2019). Silymarin not only suppresses the induction of TNF‐α but also reduces its serum concentration along with the IL1β, IFN‐γ, and other pro‐inflammatory cytokines (Nazemian et al., 2010). Further, it represses the mitogen‐activated protein kinase (MAPKs) ERK1/2 and P38 activities and release of Th1‐related cytokine IL‐2, associated with T‐cell proliferation, which may help in immunosuppression (Gharagozloo et al., 2013) to control the organ damage triggered by cytokine storm during acute COVID‐19 (Estrada, 2020; Robba, Battaglini, Pelosi, & Rocco, 2020).
The antiinflammatory activity of silymarin is quite analogous with the standard FDA‐approved drug Baricitinib, used for the treatment of Rheumatoid arthritis (RA) and now recommended as COVID‐19 therapy (Tong et al., 2019; Richardson et al., 2020). It is noteworthy that silymarin and one of its active constituent silibinin have been approved for the non‐randomized single‐arm clinical trial in RA patients (Shavandi et al., 2017), due to its inhibitory activity on TNF‐α and other pro‐inflammatory biomarkers of RA (Dupuis et al., 2018).
Figure 2. Multi‐facets of silymarin action. Established and probable pharmacological roles of silymarin have been depicted. A “+” indicates a stimulatory effect, whereas a “−” an inhibitory role. A down arrow indicates a reduction in expression levels. The red dash sign indicates steps where silymarin could stop a particular step in SARS‐CoV‐2 pathogenesis. Details are in the text [Colour figure can be viewed at wileyonlinelibrary.com]
Clinical trials have been conducted, some still awaiting results.
Various dosing regimes were employed:
3. CLINICAL FEATURES OF SILYMARIN
It is interesting to report that a randomized placebo‐controlled trial has been initiated to evaluate the clinical consequence in COVID‐19 pneumonia in Phase‐3, succeeding administration of silymarin. COVID‐19 patients with pneumonia have been receiving standard care as per the Ministry of Health Protocol of Treatment + Silymarin (oral 420 mg/day in three divided doses) against a placebo control. Various clinical outcomes, such as time in days the patient was intubated for discharge or death whichever came first, were assessed up to 28 days. Several days patient remained positive to RT‐PCR CoV‐2 swab test at post‐treatment, and any adverse events whether related to medication or not, have been carried out (US National Library of Medicine; ClinicalTrials.gov; Cairo University, Giza, Cairo, Egypt 12,613; Principal Investigator: Khaled Salem, MSc, First Posted: May 19, 2020. 08 pages; Last Update Posted: August 18, 2020‐Identifier: NCT04394208 Silymarin in COVID‐19 Pneumonia [SCOPE]. A randomized placebo‐controlled trial to assess the clinical outcome in COVID‐19 Pneumonia following administration of Silymarin owing to its role as a p38 MAPK pathway inhibitor and its antiviral, antiinflammatory, and antioxidant effects—May 19, 2020; Last Update Posted: August 18, 2020 Pages‐08. https://clinicaltrials.gov/ct2/show/NCT04394208).
Moreover, the interventional randomized clinical trial was successfully conducted for assessing the immunomodulatory activity in Beta‐Thalassemia patients. Treatment with 140 mg oral dose three times a day, 7 days a week showed significant proliferation of T cells with stimulation of B and NK cells, along with the upregulated IL‐2, IL‐4, and IFN‐gamma in the supernatant of activated T cells (US National Library of Medicine, Marjan Gharagozloo, Isfahan University of Medical Sciences, Sponsor: the Shiraz University of Medical Sciences‐2012, US National Library of Medicine; ClinicalTrials.gov Identifier: NCT01752153‐ Immunomodulatory Effects of Silymarin in patients with beta‐Thalassemia Major‐ December 19, 2012, 08 pages‐https://clinicaltrials.gov/ct2/show/NCT01752153).
In a randomized clinical trial (Phase‐2) of chronic hepatitis C patient's silymarin significantly prevented the associated liver disorders and reverse hepatic lesions with improved quality of life of the patients those used it as a dietary supplement (US National Library of Medicine, National Center for Complementary and Integrative Health (NCCIH)—January 31, 2002, Last Update Posted: August 18, 2006‐Identifier: NCT00030030—Evaluating Silymarin for Chronic Hepatitis C‐https://clinicaltrials.gov/ct2/show/NCT00030030). Another interventional non‐randomized study to evaluate the safety and efficacy of intravenous silibinin (iSIL), a major constituent of silymarin extract, on hepatitis C virus (HCV) load in 20 HCV‐HIV co‐infected patients demonstrated a significant decline in HCV‐RNA after 2 weeks of iSIL treatment at 20 mg/kg.(U.S. National Library of Medicine-ClinicalTrials.gov‐Information provided by University of Zurich‐March 22, 2013, Last Update Posted: March 5, 2015‐NCT01816490—THISTLE‐The HIV‐HCV Silibinin Trial (THISTLE) —March 22nd, 2013–July 15, 2015; 08 pages. https://clinicaltrials.gov/ct2/show/NCT01816490). Moreover, the IdB 1016 phytosome complex containing the active constituent of silymarin, oral silybin, and phosphatidylcholine, significantly improves liver enzyme levels in serum and viral load in chronic HCV patients in Phase‐2 randomized placebo‐controlled trial with doses of 314 mg, 624 mg, and 942 mg three times daily (tid) for different stages of fibrosis (US National Library of Medicine-ClinicalTrials.gov National Center for Complementary and Integrative Health (NCCIH)—March 4, 2003 Last Update Posted: August 18, 2006—Identifier: NCT00055445‐IdB 1016 Treatment for Hepatitis C Disease‐March 4, 2003–August, 2006–08 pages‐https://clinicaltrials.gov/ct2/show/NCT00055445).
Although the milk thistle treatment in chronic HCV infection failed as the conventional antiviral therapy but showed quite encouraging results for attenuation of viral load and liver marker enzymes in Phase‐2 randomized trial. Results on oxidative stress, apoptosis, and fibrogenesis of the patients, compared to placebo control, suggest rigorous trials of botanical products of milk thistle (US National Library of Medicine-ClinicalTrials.gov, National Center for Complementary and Integrative Health (NCCIH)—March 20, 2008; Last Update Posted: March 18, 2013—Identifier:NCT00680342‐Phase II Trial of Silymarin for Patients With Chronic Hepatitis C Who Have Failed Conventional Antiviral Treatment (SyNCH)‐March 20, 2008–February, 2012–08 pages‐https://clinicaltrials.gov/ct2/show/NCT00680342). Further, a recent review on diverse phytopharmaceutical suggests that silymarin can also be investigated for its ability to block the interaction of viral spike protein with the host cell receptors Furin, along with TMPRSS2 (Palit et al., 2020).
4. CONCLUSION
Currently, there is no promising officious treatment accessible for the highly contagious SARS CoV‐2. Thus, identifying novel and fruitful treatments is imperious and would be of great benefit to patients. However, numerous clinical trials are ongoing globally to discover active drugs for COVID‐19 treatment, and no drug has been proclaimed to be fruitful for curing COVID‐19 so far. Silymarin is appreciated for its various immune‐pharmacological and cytokine regulating effects and appears as a hopeful phytopharmaceutical for the management of COVID‐19 (Figure 2). More significantly, derivatives of silymarin like silybin, and silibinin have promising antiviral responses that might also be a good option. However, some vital points such as exact dosing and time course of therapy based on the severity of the disease manifestation need to be addressed for fixing the proper treatment modality to control viral infection. Additionally, the biological function of silymarin is consolidated from in‐vitro findings, animal experiments, and clinical data on related diseases may not correspond with clinical efficacy in humans. Therefore, the precise clinical curative or even prophylactic use, the optimal dose and course of treatment must be assessed following suitable preclinical and clinical study.
Taken with Quercetin, silymarin can improved the efficacy of other drugs, for instance as used in chemotherapy. From 2016 by Reddy et al:
Natural flavonoids silymarin and quercetin improve the brain distribution of co-administered P-gp substrate drugs
Abstract
P-glycoprotein (P-gp), a well known efflux transporter in the blood brain barrier inhibits the uptake of substrate drugs into brain. The main aim of this study is to evaluate the effect of natural product based P-gp inhibitors on brain penetration of various CNS drugs which are P-gp substrates. In this study, we have evaluated the inhibitory effects of natural bioflavonoids (quercetin and silymarin) on P-gp by using digoxin and quinidine as model P-gp model substrate drugs. In vitro inhibitory effects were evaluated in Caco-2 cell lines using digoxin as a model drug and in vivo P-gp inhibiting effect was evaluated in mice model using quinidine as model drug. The accumulation and bidirectional transport of digoxin in Caco-2 cells was determined in presence and absence of quercetin and silymarin. Elacridar was used as standard P-gp inhibitor and used to compare the inhibitory effects of test compounds. The apical to basolateral transport of digoxin was increased where as basolateral to apical transport of digoxin was decreased in concentration dependent manner in the presence of elacridar, quercetin and silymarin. After intravenous administration of P-gp inhibitors, brain levels of quinidine were estimated using LC-MS method. Increased brain uptake was observed with quercetin (2.5-fold) and silymarin (3.5-fold). Though the brain penetration potential of P-gp substrates was lower than that observed in elacridar, both quercetin and silymarin improved plasma quinidine levels. Caco-2 permeability studies and brain uptake indicate that both quercetin and silymarin can inhibit P-gp mediated efflux of drug into brain. Our results suggest that both silymarin and quercetin could potentially increase the brain distribution of co-administered drugs that are P-gp substrates.
Silymarin also works synergistically with berberine.
A meta-analysis of various trials by Fogacci et al (2019) demonstrated significantly improved blood lipid profiles.
Metabolic effect of berberine–silymarin association: A meta‐analysis of randomized, double‐blind, placebo‐controlled clinical trials
Abstract
The aim of this study is to assess the impact of a combination of berberine and silymarin on serum lipids and fasting plasma glucose (FPG) through a systematic review of literature and meta‐analysis of the available randomized, double‐blind, placebo‐controlled clinical trials (RCTs). A systematic literature search in SCOPUS, PubMed‐Medline, ISI Web of Science, and Google Scholar databases was conducted up to October 2, 2018, in order to identify RCTs assessing changes in plasma concentrations of total cholesterol (TC), triglycerides (TG), high‐density lipoprotein cholesterol (HDL‐C), low‐density lipoprotein cholesterol (LDL‐C) and FPG during treatment with berberine and silymarin in combination. Two review authors independently extracted data on study characteristics, methods, and outcomes. Quantitative data synthesis was performed using a random‐effects model. We identified five eligible RCTs, with 497 subjects overall included. Berberine and silymarin combination treatment exerted a positive effect on TC (mean difference [MD]: −25.3, 95% CI [−39.2, −11.4] mg/dl; p < 0.001), TG (MD: −28, 95% CI [−35.3, −20.6] mg/dl; p < 0.001), HDL‐C [MD: 6, 95% CI [3.2, 8.8] mg/dl; p < 0.001), LDL‐C (MD: −29.1, 95% CI [−39.7, −18.6] mg/dl; p < 0.001), and FPG (MD: −7.5, 95% CI [−13, −1.9] mg/dl; p = 0.008). The present findings suggest that the coadministration of berberine and silymarin is associated with an advantageous improvement in lipid and glucose profile, suggesting the possible use of this nutraceutical combination in order to promote the cardiometabolic health.
Figure 2. Forest plot detailing mean differences and 95% confidence intervals for the studies included in the meta‐analysis [Colour figure can be viewed at wileyonlinelibrary.com]
Finally, a clinical trial investigating the improvements to the lipid profile of patients who are intolerant of statins from 2015 by Di Pierro et al.
I could go on but then it would become a full review!
Clinical role of a fixed combination of standardized Berberis aristata and Silybum marianum extracts in diabetic and hypercholesterolemic patients intolerant to statins
Abstract
Background: Statin intolerance is a medical condition often leading patients to nonadherence to the prescribed therapy or to a relevant reduction of the statin dosage. Both situations determine a totally or partially uncontrolled lipid profile, and these conditions unquestionably increase the risk of cardiovascular events.
Methods: We enrolled hypercholesterolemic, type 2 diabetic patients complaining of intolerance to statins. Some of them had reduced the statin dose 'until the disappearance of symptoms'; others had opted for treatment with ezetimibe; and yet others were not undergoing any treatment at all. All patients of the three groups were then given a fixed combination of berberine and silymarin (Berberol(®)), known from previous papers to be able to control both lipidic and glycemic profiles.
Results: The tested product both as a single therapy and as add-on therapy to low-dose statin or to ezetimibe reduced triglycerides, low-density lipoprotein cholesterol, fasting blood glucose, and glycosylated hemoglobin in a significant manner without inducing toxicity conditions that might be somehow ascribed to a statin-intolerant condition.
Conclusion: Our study demonstrates that use of Berberol(®), administered as a single or add-on therapy in statin-intolerant subjects affected by diabetes and hypercholesterolemia is a safe and effective tool capable of improving the patients' lipidic and glycemic profiles.
Keywords: Berberol®; berberine; cholesterol; ezetimibe; silymarin; type 2 diabetes.
Side effects, interactions and dosing advice from WebMD:
Side Effects
When taken by mouth: Milk thistle extract is LIKELY SAFE for most people when taken by mouth. In some people, taking milk thistle extract can cause diarrhea, nausea, intestinal gas, fullness, loss of appetite, and possibly headache.
When applied to the skin: Milk thistle extract is POSSIBLY SAFE when applied directly to the skin for short periods of time.
Special Precautions and Warnings
When taken by mouth: Milk thistle extract is LIKELY SAFE for most people when taken by mouth. In some people, taking milk thistle extract can cause diarrhea, nausea, intestinal gas, fullness, loss of appetite, and possibly headache.
When applied to the skin: Milk thistle extract is POSSIBLY SAFE when applied directly to the skin for short periods of time. Pregnancy and breast-feeding: There isn't enough reliable information to know if milk thistle is safe to use when pregnant or breast-feeding. Stay on the safe side and avoid use.
Children: Milk thistle is POSSIBLY SAFE when taken by mouth, appropriately, for up to 9 months in children 1 year of age and older.
Allergy to ragweed and related plants: Milk thistle may cause an allergic reaction in people who are sensitive to the Asteraceae/Compositae plant family. Members of this family include ragweed, chrysanthemums, marigolds, daisies, and many others. If you have allergies, be sure to check with your healthcare provider before taking milk thistle.
Hormone-sensitive conditions such as breast cancer, uterine cancer, ovarian cancer, endometriosis, or uterine fibroids: Milk thistle extracts might act like estrogen. If you have any condition that might be made worse by exposure to estrogen, don't use these extracts.
Interactions ?
Moderate Interaction
Be cautious with this combination
Medications changed by the liver (Glucuronidated Drugs) interacts with MILK THISTLE
The body breaks down some medications to get rid of them. The liver helps break down these medications. Taking milk thistle might affect how well the liver breaks down drugs. This might increase or decrease how well some of these medications work.
Some of these medications changed by the liver include acetaminophen (Tylenol, others) and oxazepam (Serax), haloperidol (Haldol), lamotrigine (Lamictal), morphine (MS Contin, Roxanol), zidovudine (AZT, Retrovir), and others.
Tamoxifen (Nolvadex) interacts with MILK THISTLE
Milk thistle might increase how much tamoxifen is absorbed by the body. This might increase the effects and side effects of tamoxifen. Before taking milk thistle, talk to your healthcare provider if you are taking tamoxifen.
Medications for diabetes (Antidiabetes drugs) interacts with MILK THISTLE
Milk thistle can lower blood sugar levels. Taking milk thistle along with diabetes medications might cause your blood sugar to be too low. Monitor your blood sugar closely. The dose of your diabetes medication might need to be changed.
Some medications used for diabetes include glimepiride (Amaryl), glyburide (DiaBeta, Glynase PresTab, Micronase), insulin, metformin (Glucophage), pioglitazone (Actos), rosiglitazone (Avandia), and others.
Sirolimus (Rapamune) interacts with MILK THISTLE
Taking milk thistle might decrease how well the liver breaks down sirolimus. This might increase the effects and side effects of sirolimus. Before taking milk thistle, talk to your healthcare provider if you are taking sirolimus.
Raloxifene (Evista) interacts with MILK THISTLE
Taking milk thistle might decrease how well the body breaks down raloxifene in the intestines. This might increase the effects and side effects of raloxifene. Before taking milk thistle, talk to your healthcare provider if you are taking raloxifene.
Medications moved by pumps in cells (P-Glycoprotein Substrates) interacts with MILK THISTLE
Some medications are moved by pumps in cells. Milk thistle might make these pumps less active and increase how much of some medications get absorbed by the body. This might cause more side effects from some medications.
Some medications that are moved by these pumps include etoposide, paclitaxel, vinblastine, vincristine, vindesine, ketoconazole, itraconazole, amprenavir, indinavir, nelfinavir, saquinavir, cimetidine, ranitidine, diltiazem, verapamil, digoxin, corticosteroids, erythromycin, cisapride (Propulsid), fexofenadine (Allegra), cyclosporine, loperamide (Imodium), quinidine, and others.
Morphine interacts with MILK THISTLE
Milk thistle might affect levels of morphine in the blood. This might increase or decrease the effects of morphine. Before taking milk thistle, talk to your healthcare provider if you are taking morphine.
Warfarin (Coumadin) interacts with MILK THISTLE
Warfarin (Coumadin) is used to slow blood clotting. Taking milk thistle might make warfarin too effective, which could increase the risk of bleeding. Before taking milk thistle, talk to your healthcare provider if you are taking warfarin.
Minor Interaction
Be watchful with this combination
Estrogens interacts with MILK THISTLE
Milk thistle might increase how fast the body breaks down estrogen pills to get rid of them. Taking milk thistle along with estrogens might decrease the effectiveness of estrogen pills. Milk thistle contains a chemical called silymarin. Silymarin might be the part of milk thistle that helps the body break down estrogens.
Some estrogen pills include conjugated equine estrogens (Premarin), ethinyl estradiol, estradiol, and others.
Medications changed by the liver (Cytochrome P450 2C9 (CYP2C9) substrates) interacts with MILK THISTLE
Some medications are changed and broken down by the liver. Milk thistle might decrease how quickly the liver breaks down some medications. Taking milk thistle along with some medications that are broken down by the liver might increase the effects and side effects of these medications. Before taking milk thistle, talk to your healthcare provider if you take any medications that are changed by the liver.
Some medications that are changed by the liver include amitriptyline (Elavil), diazepam (Valium), zileuton (Zyflo), celecoxib (Celebrex), diclofenac (Voltaren), fluvastatin (Lescol), glipizide (Glucotrol), ibuprofen (Advil, Motrin), irbesartan (Avapro), losartan (Cozaar), phenytoin (Dilantin), piroxicam (Feldene), tamoxifen (Nolvadex), tolbutamide (Tolinase), torsemide (Demadex), warfarin (Coumadin), and others.
Medications used for lowering cholesterol (Statins) interacts with MILK THISTLE
Theoretically, milk thistle might change the levels of some medications used for lowering cholesterol (statins). This might decrease how well these medications work. Some medications used for lowering cholesterol include atorvastatin (Lipitor), fluvastatin (Lescol), lovastatin (Mevacor), pravastatin (Pravachol), and rosuvastatin (Crestor).
Medications changed by the liver (Cytochrome P450 3A4 (CYP3A4) substrates) interacts with MILK THISTLE
Some medications are changed and broken down by the liver. Milk thistle might affect how quickly the liver breaks down some medications. Taking milk thistle along with some medications that are broken down by the liver might increase or decrease the effects of these medications. Before taking milk thistle, talk to your healthcare provider if you take any medications that are changed by the liver.
Some medications changed by the liver include lovastatin (Mevacor), ketoconazole (Nizoral), itraconazole (Sporanox), fexofenadine (Allegra), triazolam (Halcion), alprazolam (Xanax), amlodipine (Norvasc), clarithromycin (Biaxin), cyclosporine (Sandimmune), erythromycin, verapamil (Calan, Isoptin) and many others.
Indinavir (Crixivan) interacts with MILK THISTLE
Indinavir is a drug that is changed and broken down by the liver. Milk thistle might increase how quickly the liver breaks down some medications. But milk thistle does not seem to affect how quickly the body breaks down indinavir.
Dosing
The following doses have been studied in scientific research:
ADULTS BY MOUTH:
For diabetes: Milk thistle extract 210-600 mg has been used daily for up to 6 months. 200 mg of milk thistle extract has been taken once daily or three times daily for 4 months to one year. A specific product (Berberol, PharmExtracta) containing 210 mg of milk thistle extract and 1176 mg of tree turmeric extract has been taken daily for 3-12 months.
Media disinformation: Is it Long COVID or a Vaccine Injury?
Hat tip to Eugyppius. It was paywalled so I had to do my own investigations. And it was quite revealing, we see it so often with young people dropping dead. The V word is almost never allowed to be mentioned, it's always the elephant in the room, absence=confirmation.
This sort of sham article, whether accidental or deliberately pro narrative, serves to help no-one avoid or control their condition. A complicit medical profession, incompetent or just plain misinformed it's hard to tell?
The lack of a positive PCR, ever, rules out LC. No viral mRNA, no LC. The End.
You must call something what it is or you are wasting your efforts on the wrong treatments, misleading others and blaming government policy or Omicron when, as in this case, it's not that at all.
It was most likely complicated by an opportunistic infection at a time of induced immunosuppression.
What Rose and her GP appear to be wilfully blind to is that all these issues arose commensurate with the administering of the “Gulf War Syndrome” type jab combo.
These symptoms are identical to the now well known vaccine-associated adverse events.
Published May 1st:
I was a marathon runner with killer biceps – long Covid has stopped me in my tracks
Rose George
Endurance athletes have been left using wheelchairs or barely able to walk. But the government acts like Covid is beaten
One of the mysteries of Covid is how it hits the fit. Before January, I was one of those people. I ran 30 miles a week. I could turn up to a 20-mile fell race on inadequate training and run it, thoughtlessly. I did yoga, weight training and cycling. I had a low resting heart rate and strong biceps. For a 52-year-old menopausal woman, I was in extremely good shape.
But then on 3 January I fell ill with a sore throat, then flu-like weakness, a cough that hasn’t left me since, and a constant and persistent headache that is resistant to every painkiller. In the months since, I have been not ill, but not well. I have days of feeling fine, and then I don’t. As a runner, I can say that long Covid feels like the wall at mile 18 in a marathon, when suddenly your energy has gone, and you feel like a different person and you don’t know why.
It’s appropriate to use a running analogy, because it seems that runners, triathletes, cyclists and other formerly fit people populate the long Covid forums in far greater numbers than you’d expect if, like me, you assumed that fitness and health were the perfect shield. My long Covid is suspected by my GP, since I never actually tested positive, but many on the forums had only mild infections and are still suffering. Some are now in wheelchairs, or confined to bed, or disabled, or dysfunctional, and they post on social media groups that can be wonderfully precise: Long Covid for Endurance Athletes is one group I found extremely helpful (a name that caused a Crohn’s-afflicted friend to say wistfully: “Is there a group for former TV writers with a poo bag?”).
I suppose I am lucky that I have long Covid now, when science believes in it and there are long Covid clinics. The NHS Covid recovery site must be helpful for many, and it discusses PEM (post-exertional malaise) which is the delayed-onset crash after exercise and is one of the most frustrating mysteries about any post-viral condition: you exercise and feel fine, and two days later you suddenly don’t. But the NHS site and most others seem meant for people who can’t walk upstairs, not ones who wonder whether they will be able to run in heart zone 3 again, or ever do more than three miles without fearing the consequences; the ones who are not disabled but not themselves.
I turned, of course, to Google. I learned that people with chronic fatigue syndrome (CFS), or myalgic encephalomyelitis (ME), have been floored by PEM for decades and only now are they being believed. I learned that perhaps Covid is lurking in my gut, or making my mast cells fire when they shouldn’t, and that I should be careful of my heart because doing too much can give me myocarditis. But my heart is fine, along with my X-rayed lungs and my blood, once a drop in my infection-fighting white blood cells had recovered. Whatever Covid is doing to me, it is doing it quietly and sneakily.
It is stealth that characterises long Covid’s baffling array of symptoms and sufferers’ equally baffling tendency to get better, then relapse, sometimes for no reason. A Lancetstudy found that long Covid sufferers reported on average more than 50 symptoms during their illness, across an average of 9.1 organ systems.
Yet Covid, according to our government, is no longer a concern. Never mind that everyone I talk to about long Covid knows someone with it, that more than a million Britons have it, and almost two-thirds of those say it has significantly limited their daily activities. One in 16 people now have Covid, according to Imperial College London’s April React study, 40% more than at Omicron’s “peak” in January, and the highest number ever.
Sometimes I feel as though I am gaslighting myself. I can walk around so I can’t be ill. I can work, so I can’t be ill. Sometimes I can run, so I can’t be ill. But then I remember: once there was a time when I didn’t always have a headache. I used to be able to laugh without coughing. I used to walk to the shops half a mile away without wondering how I would find the strength to walk home again.
I am so much better off than most, the ones who have debilitating brain fog, who cannot work or walk. But still I mourn the thoughtlessness of good health, the time when, to borrow a phrase from the writer Sinéad Gleeson, my body was an afterthought. I trusted it. Now I can’t rely on my body because I don’t know what’s happening to it, and neither does anyone else. “I’m so sorry,” said my lovely GP, phoning me from her home because she had Covid. “We’re in the dark.” As are employment lawyers, still struggling to understand whether workers missing with long Covid have a disability or an occupational health condition. What is certain is that long Covid is costing us hugely, and not just in money.
It's a sham article and it needs retracting. Here’s why, the backstory:
Nov'15th:
March 10th:
We know spike protein can persist for months in the lymph node germinal centres & monocytes, about ROS inactivated T cells & lymphopenia or even lymphoma, type 1 interferon reduction, TLR disruption, autoimmune disease, neurological cytotoxicity, endothelial damage, reverse transcription etc otherwise known as VAIDS:
Such disinformation and gaslighting by the “experts” helps no-one to properly diagnose and treat their complex of symptoms.
Published June 11th:
Living with long Covid: ‘This is not a fake illness – on bad days all I can do is drag myself to the bathroom’
Sophie Raudnitz, 48, is a teacher and lives Northamptonshire, with her husband and their three children. Dr Raudnitz developed long Covid after contracting Covid over Christmas and has been unable to return to work since. She tells Katie Grant how, in addition to experiencing crippling fatigue and a host of other symptoms, she has also had to deal with long Covid-deniers who refuse to believe the illness even exists.
“I had Covid over Christmas really mildly – it was just a cold. But as the cold symptoms lifted the fatigue came down. I went back to work for two days when I’d had it for three weeks – I thought, ‘I can do this’. I was totally wiped out. I just knew I couldn’t go back.
The fatigue that comes with Long Covid is like no tiredness I’ve ever experienced before. It’s total. On the days that are really bad all I can do is lie in bed, look at the sky and drag myself to the bathroom.
When my fatigue is bad I get a raft of other symptoms, and my body is coming up with new ones all the time. They include breathing problems, gastrointenstinal issues and postural tachycardia syndrome (PoTS), which causes your heart to beat abnormally fast after sitting up or standing. For people with PoTS, rather than recovering from that after 20 seconds or so, their heartbeat continues to speed up and they can become lightheaded, experience breathing difficulties or faint. It is frightening.
I’ve got two dogs and I used to go out with them for an hour and a half. When I was really bad I couldn’t walk at all. Now I’ve just built it up to 25 minutes but I’m really exhausted from that.
The only things that have got me through with any kind of sanity are a yoga instructor I discovered on YouTube who had long Covid herself, and a colleague who also developed it.
Completely by chance, someone recommended I do a type of restorative yoga and I discovered the instructor, Suzy Bolt. She teaches live classes online targeted at people with long Covid and there is a whole community of fans on Facebook. It’s been a lifesaver for me. The group is so empathetic and kind.
With my colleague, it’s just so useful to have someone else going through exactly the same thing who gets it, because part of what is so destabilising about this illness is that recovery is so uneven. You might be fine one day and then crash the next and you don’t know why.
Where professional healthcare workers are concerned I think that body of knowledge is developing but it hasn’t really been disseminated in a very effective way to healthcare providers. I went to the GP quite early on, had blood tests and an ECG – everything came back normal, which is the usual story with long Covid. I fought very hard to be referred to a long Covid clinic.
When I finally got an appointment a couple of weeks ago, I’d really been hoping for a conversation about the various weird symptoms I get. But it became obvious really quickly that, with the best will in the world, this occupational therapist just didn’t have the detailed expertise to be able to go into this in any detail.
Having just had a conversation about how I get out of breath and my heart sky rockets when climbing the stairs, she said, ‘Pace yourself – if you usually run 5K, start with 3K.’ I was thinking, ‘I can’t even walk down the road, let alone run.’ I wanted to know, what is this illness I have? It’s really difficult living with an illness about which so little is known and for which there is so little help.
My family and friends have been fantastic and my work has also been really supportive. I attempted to have a return to work in late April but I had a relapse and couldn’t do it. I’m just in negotiations now about another return.
Long Covid returns are different from other illnesses – they have to be done so slowly and so carefully and the situation is really fragile. I am going back into it knowing I could relapse at any point.
Different people experience long Covid differently, which is partly why there has been so much scepticism around it I think, and why even in the medical community people are struggling to get to grips with it.
I’ve had some flack on Twitter from people who think long Covid is just a fake illness invented by skivers. I haven’t tried to battle trolls because I know they aren’t really open to logical argument. Their minds are made up and my energy has been so frayed I need to save it for things that are more important.
Often, people with long Covid don’t ‘look’ ill. Close friends and family can tell with me when the symptoms are biting hard but to people who don’t know me well, I probably look fine. I think this makes it far easier for people to dismiss this as a fake illness. It also makes it harder for people who don’t know much about the illness to understand it – it doesn’t look like you expect illness to look like.
Part of the growing body of medical knowledge about long Covid is that there are very real physical causes for our symptoms. Many medical practitioners are still approaching Long Covid as if it’s a mental issue but it’s a real, physical illness, and not in our heads.”
This isn’t to poke fun and humiliate but to get to the facts, which is a post transfection COVID-19 Omicron infection which should have been mild instead leading to a chronic condition with multiple symptoms including for cardiovascular and neurological damage.
And the “experts” should have right on top of that after 2+ years of research & clinical data in abundance.
Publishing only half the facts in a national newspaper, a very public forum, opens you up to public scrutiny and with good reason.
This site is strictly an information website about potential therapeutic agents and a review of the current state of research. It does not advertise anything, provide medical advice, diagnosis or treatment. This site is not promoting any of these as potential treatments or offers any claims for efficacy. Its content is aimed at researchers, registered medical practitioners, nurses or pharmacists. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website. Always consult a qualified health provider before introducing or stopping any medications as any possible drug interactions or effects will need to be considered.
DoorlessCarp’s Scientific Literature Reviews is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
It already seems like I’m taking a load of supplements. Which ones should I definitely add? Any I should stop taking? Thank you for this excellent article. Following is my daily prevention supplement cocktail. I haven’t been sick since I started it a year ago after a nasty bout with Delta.
Tri-Magnesium
NAC
Krill Oil
D3
Vitamin K-Complex
Choline
Glutathione
Quercetin-Bromelain Complex
Niacin
Black Cumin Seed Oil and Curcumin Elite
Lutein
CoQ10
Zinc
Selenium
Methyl B12 Plus
Vitamin C
Glucosamine+Chondroitin
Collagen Peptides
Melatonin
Low-dose Aspirin if needed, occasionally
Regular exposure to sunshine (I have a pretty decent tan, not too much 🙂)







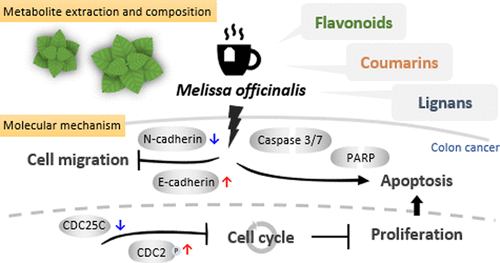






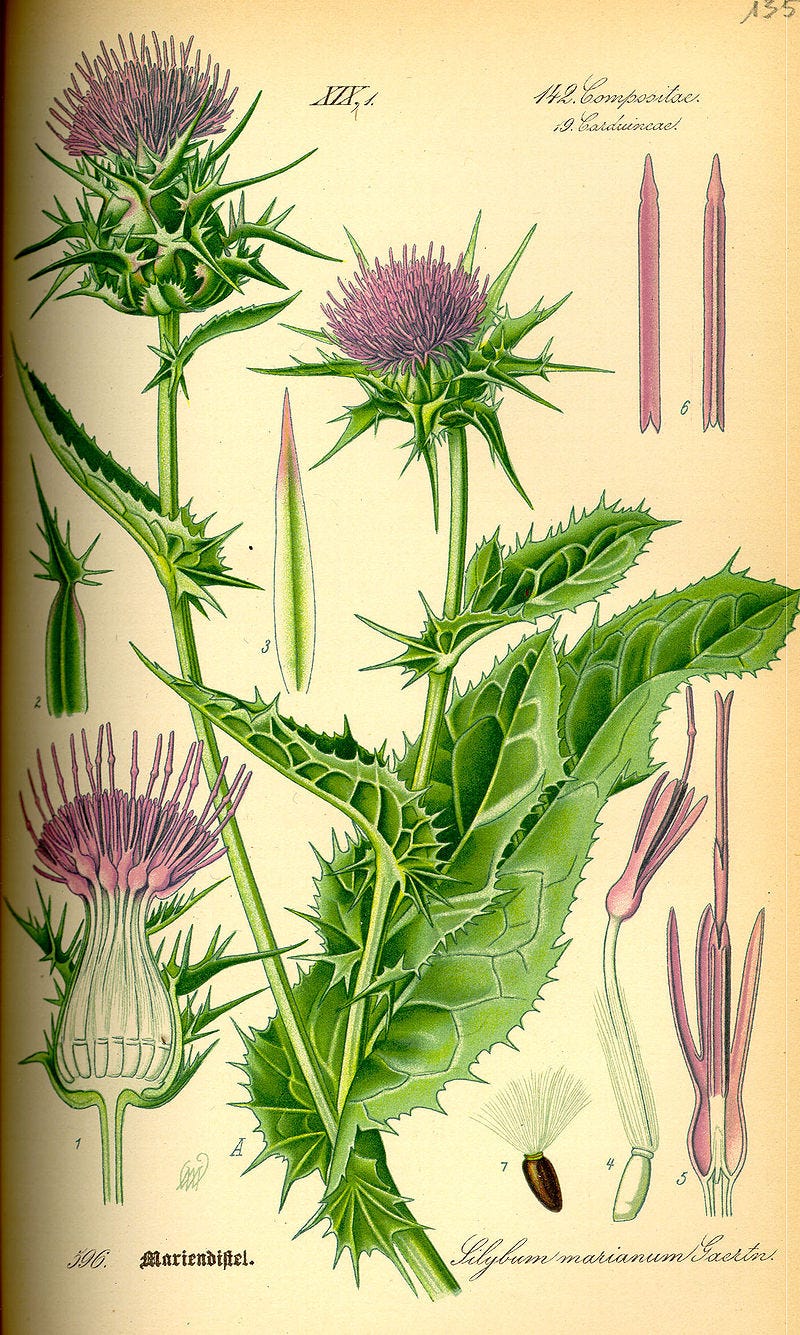











It already seems like I’m taking a load of supplements. Which ones should I definitely add? Any I should stop taking? Thank you for this excellent article. Following is my daily prevention supplement cocktail. I haven’t been sick since I started it a year ago after a nasty bout with Delta.
Tri-Magnesium
NAC
Krill Oil
D3
Vitamin K-Complex
Choline
Glutathione
Quercetin-Bromelain Complex
Niacin
Black Cumin Seed Oil and Curcumin Elite
Lutein
CoQ10
Zinc
Selenium
Methyl B12 Plus
Vitamin C
Glucosamine+Chondroitin
Collagen Peptides
Melatonin
Low-dose Aspirin if needed, occasionally
Regular exposure to sunshine (I have a pretty decent tan, not too much 🙂)
There was a study in South Korea about Sea Buckthorn Berries.