Any extracts used in the following article are for non-commercial research and educational purposes only and may be subject to copyright from their respective owners.
I’m writing this at the request of Dr “Maples”, who wishes to remain anonymous but is seeing the carnage that its misuse is causing, along with many other misguided anti-COVID measures.
Chlorine dioxide, (hereafter ClO2), is a powerful neutraliser of SARS-CoV-2 viruses when applied as a water based solution. In fact, it is many times more effective than sodium hypochlorite based bleach at the same concentration of 24 ppm1.
When used as directed with short term exposure as a nasal rinse2 or a mouthwash3 before dental work it may be a useful surface sterilant that can reduce viral loads on mucosal surfaces. But there is no sound experimental evidence of effectiveness when taken internally - there is no evidence that it can reduce SARS-CoV-2 viral loads or act as a prophylactic against infection4.
In some countries safe proven antivirals such as ivermectin or quercetin are unfortunately not readily available due to import restrictions or cost.
It's especially an issue in Central-South America. Misinformed individuals, perhaps unduly scared due to propaganda that they are at high risk of death due to COVID-19, have been misusing ClO2, even to this day. They have been taking it as a systemic antiviral, not as a surface sterilant, seeing it as some sort of miracle cure and preventative of disease.
According to Maples, some individuals have even been drinking litres of it, daily.
As the solution is weak in comparison to bleach it may appear to be quite safe with no immediate ill effects at first, but this couldn't be more wrong unless the dose is tightly controlled and is kept very low.
Either way its a completely pointless risk to take, other than for sterilizing unsafe drinking water in an emergency via low dose water purifying tablets.
The purpose of this Substack is to explore the pharmacotoxicity of ClO2 and cite related case studies which give examples of what damage you can do to yourself.
I've created a regularly updated list of safer and more effective alternatives, some of which you can grow yourself in most parts of the world and unlike ClO2 these have a lot of research and sometimes thousands of years of use behind them:
First, a little background about its physical properties and pharmacology:
ClO2 is a small, volatile and very strong molecule that exists as a free radical in dilute solutions. It is a gas at normal temperatures and pressures, with a melting point of -59°C, a boiling point of 11°C, is yellowish/green in colour and has a smell similar to chlorine.
It is explosive when mixed in air at concentrations above 10%, so it is normally generated in situ within an aqueous solution at <0.2%5.
I agree with their conclusions on toxicology but caution that this paper does class ivermectin in a similar light!
Chlorine dioxide is a reactive greenish-yellow gas often obtained by reacting sodium chlorite and/or chlorate with acids and reducing agents. This chemical is a strong and effective water-soluble oxidizer [5,11]. These properties make it ideal for use as a biocide and bleaching agent. It acts by oxidizing and disrupting cellular and viral components such as membranes and proteins [5]. Although it oxidizes a wide range of biological molecules, eukaryotic cells seem to be less susceptible to this damage [12]. It is mostly encountered by the general population at low concentrations as a disinfectant in municipal water, where its concentration is controlled, and as an antiseptic in hospitals [5,13,14]. Additionally, it has been evaluated as a food and dental disinfectant and mouthwash with mixed results [11,12]. When ingested, it is rapidly absorbed through the digestive tract, reaching peak concentration about one hour after dosing. It is slowly absorbed through the skin and can cause severe lung damage if inhaled at high concentration [5,15]. It is metabolized into chlorite, chlorate, and chloride ions and eliminated in the urine and feces [5,15].
The ingestion of chlorine dioxide can produce serious adverse effects, including acute liver failure, hemolytic anemia, respiratory failure due to methemoglobinemia, hydroelectrolytic imbalance (hypotension), prolongation of the QT interval that causes arrhythmias, eye irritation, and severe diarrhea and vomiting [25,26]. Other adverse effects include nausea [25,26], esophagitis [5], bronchospasm [26], pruritus [26], and chemical pneumonitis [25].
Reference "25" is from a 7 page Chilean PDF which has been cited by several studies7:
In 1982, Bercz et al investigated the subchronic toxicity of ClO2 and its related compounds when given to African Green monkeys over a period of 30-60 days using rising dose protocols.
Subchronic systemic toxicity is defined as adverse effects occurring after the repeated or continuous administration of a test sample for up to 90 days or not exceeding 10% of the animal's lifespan.
The only unexpected and significant toxic effect was induced by ClO2 and not by the other compounds they tested, which included NaClO2 and NaClO3 at up to 60 mg /kg/day.
In a human weighing 70kg this equates to a total of 4.2g of ClO2 per day, if the ED50’s (effective dose rates) are comparable.
The principle effect was a reversible, statistically significant decrease of serum thyroxine, which occurred after the fourth week of exposure at 100 mg/l8:
The selective thyroid effect of ClO2 was unexplained and it appeared to be paradoxical since ClO2 was rapidly reduced by the oral and gastric secretions to nonoxidizing species (presumably Cl-). No evidence of thyroid effects were detected in the serum of human volunteers who ingested approximately 1 mg/l. of ClO2 in drinking water as a result of routine use in the community water treatment process.
Key takes from the a toxicological review of ClO2 and chlorite, prepared by the U.S. Environmental Protection Agency (EPA) in 20009:
Chlorine dioxide and chlorite are characterized together in this report because studies conducted with chlorite, the predominant degradation product of chlorine dioxide, are likely relevant to characterizing the toxicity of chlorine dioxide. In addition, studies conducted with chlorine dioxide may be relevant to characterizing the toxicity of chlorite. Chlorine dioxide is fairly unstable and rapidly dissociates, predominantly into chlorite and chloride, and to a lesser extent, chlorate. There is a ready interconversion among these species in water (before administration to animals) and in the gut (after ingestion) (U.S. EPA, 1994d). Therefore, what exists in water or the stomach is a mixture of these chemical species (i.e., chlorine dioxide, chlorite, chlorate) and possibly their reaction products with the gastrointestinal contents.
3.1.1. Gastrointestinal Absorption
3.1.1.1. Chlorine Dioxide
After ingestion, chlorine dioxide is rapidly absorbed from the gastrointestinal tract. Levels of radioactive chlorine in plasma peaked 1 hour after Sprague-Dawley rats were administered a single gavage dose of 100 mg/L 36ClO2 (approximately 1.4 mg/kg) (Abdel-Rahman et al., 1979a). Peak plasma levels were achieved 2 hours after Sprague-Dawley rats received a gavage dose of 300 mg/L 36ClO2 after a 15-day exposure to 100 mg/L chlorine dioxide in drinking water (Abdel-Rahman et al., 1979a). Approximately 30% of the 100 mg/L single gavage dose was excreted in the urine after 72 hours, indicating that at least 30% of the dose was absorbed (Abdel-Rahman et al., 1979a); the absorption rate constant and half time were 3.77/hour and 0.18 hours, respectively (Abdel-Rahman et al., 1982). Since total radioactivity was measured rather than identification of individual chemical entities, it was not clear from these reports whether the parent chlorine dioxide itself or the chlorite, chlorate, or chloride ion degradation products were absorbed.
3.1.1.2. Chlorite
Chlorite is also rapidly absorbed from the gastrointestinal tract. Peak plasma levels of radiolabeled chlorine were reached 2 hours after administration of a single gavage dose of 10 - mg/L 36ClO2 (approximately 0.13 mg/kg) to Sprague-Dawley rats. Using 72-hour urinary 3 excretion data, it can be assumed that at least 35% of the initial dose was absorbed (Abdel-Rahman et al., 1984a). The absorption rate constant and half-time were 0.198/hour and 3.5 hours, respectively (Abdel-Rahman et al., 1982). Since total radioactivity was measured rather than identification of individual chemical entities, it was not clear from these reports whether the parent chlorine dioxide itself or the chlorite, chlorate, or chloride ion degradation products were absorbed.
3.3. METABOLISM
3.3.1. Chlorine Dioxide
Chloride ion is the ultimate metabolite of chlorine dioxide. Approximately 87% and 80% of radiolabeled chlorine in the urine (collected 0–72 hours after administration) and plasma (collected 72 hours after administration), respectively, are in the form of chloride ion following administration of a single gavage dose of 100 mg/L 36ClO2 in rats (Abdel-Rahman et al., 1979b). Chlorite was a major metabolite, accounting for approximately 11% and 21% of urine and plasma 36Cl, respectively; approximately 2% of the urinary 36Cl was in the form of chlorate. An in vivo recovery study by Bercz et al. (1982) suggests that ingested chlorine dioxide is rapidly reduced in the stomach to nonoxidizing species (presumably chloride). Five minutes after chlorine dioxide was instilled into the stomach of a monkey, only 8% of the total oxidizing capacity equivalents of chlorine dioxide was recovered. Bercz et al. (1982) also reported that in vitro chlorine dioxide was rapidly reduced to chloride ion by saliva obtained from anesthetized monkeys.
3.3.2. Chlorite
Although fewer data are available on metabolism of chlorite, it is likely that metabolism of chlorite is similar to that of chlorine dioxide. Approximately 85% of the 36Cl recovered in the urine of Sprague-Dawley rats 0–72 hours after administration of a single gavage of 10 mg/L 36 - ClO2 was in the form of chloride; the remaining 15% was present as chlorite (Abdel-Rahman et al., 1984a).
When administered orally at low concentrations per kg it is of relatively low toxicity:
4.1. STUDIES IN HUMANS—EPIDEMIOLOGY, CASE REPORTS, CLINICAL CONTROLS
4.1.1. Oral Exposure
4.1.1.1. Chlorine Dioxide
The short-term toxicity of chlorine dioxide was assessed in two human studies conducted by Lubbers and associates (Lubbers et al., 1981, 1982, 1984a; Bianchine et al., 1981). In the first study (Lubbers et al., 1981; also published as Lubbers et al., 1982), a group of 10 healthy male adults drank 1,000 mL (divided into two 500 mL portions, separated by 4 hours) of a 0 or 24 mg/L chlorine dioxide solution (0.34 mg/kg, assuming a 70 kg reference body weight). In the second study (Lubbers et al., 1984a), groups of 10 adult males were given 500 mL distilled water containing 0 or 5 mg/L chlorine dioxide (0.04 mg/kg-day assuming a reference body weight of 70 kg) for 12 weeks. Neither study found any physiologically relevant alterations in general health (observations and physical examination), vital signs (blood pressure, pulse rate, respiration rate, and body temperature), serum clinical chemistry parameters (including glucose, urea nitrogen, phosphorus, alkaline phosphatase, and aspartate and alanine aminotransferases), serum triiodothyronine (T3) and thyroxine (T4) levels, or hematologic parameters.
4.1.1.2. Chlorite
Lubbers et al. (1981, 1982, 1984a) also examined the toxicity of chlorite in normal healthy adults in studies that were run concurrently with the chlorine dioxide studies. In the single exposure study (Lubbers et al., 1981, 1982), 10 male adults consumed two 500 mL (separated by 4 hours) solutions containing 2.4 mg/L chlorite (0.034 mg/kg assuming a reference body weight of 70 kg). In a 12-week study (Lubbers et al., 1984a), groups of 10 men drank 500 mL solutions of 0 or 5 mg/L chlorite (0.04 mg/kg-day assuming a 70 kg body weight). No physiologically relevant alterations in general health (observations and physical examination), vital signs, hematologic (including erythrocyte and total and differential leukocyte counts, hemoglobin, hematocrit, and methemoglobin) or serum clinical chemistry (including glucose, electrolytes, calcium, urea nitrogen, enzyme levels, and cholesterol) parameters, or serum T3 or T4 levels were found in either study. In a companion study, three healthy glucose-6-phosphate dehydrogenase deficient male subjects were given deionized water containing 5 mg/L chlorite (0.04 mg/kg-day assuming a reference body weight of 70 kg) for 12 weeks (Lubbers et al., 1984b). Compared with the 6 control group in Lubbers et al. (1984a), the chlorite exposure did not alter general health, vital signs, hematologic parameters (including erythrocyte and total and differential leukocyte counts, hemoglobin, hematocrit, and methemoglobin) or serum clinical chemistry (including glucose, electrolytes, calcium, urea nitrogen, enzyme levels, and cholesterol) parameters.
Results were the same when they analysed those taking it in low dose treated drinking water over long periods. In contrast, exposure by inhalation on the gas has proved fatal at only 19ppm (52 mg/m3).
Several studies of in vivo toxicity when taken orally were reviewed, but definitive dose thresholds have been difficult to determine:
Daniel et al. (1990) exposed groups of 10 male and 10 female Sprague-Dawley rats to chlorine dioxide in drinking water for 90 days at concentrations of 0, 25, 50, 100, or 200 mg/L. These concentrations correspond to administered doses of 0, 2, 4, 6, or 12 mg/kg-day chlorine dioxide for males and 0, 2, 5, 8, or 15 mg/kg-day chlorine dioxide for females (calculated by the study authors using water consumption and body weight data). No exposure-related deaths were reported. Exposure to 200 mg/L resulted in significant reductions in terminal body weights and body weight gain (26%–29% lower than controls). Significant reductions in water consumption were observed in the males exposed to 50 mg/L and in females exposed to 25 mg/L; decreases in food consumption were also observed in the 200 mg/L males. Absolute liver weights were decreased in males at 50 mg/L, and absolute spleen weights were decreased in females at 25 mg/L. No consistent alterations in hematologic parameters (erythrocyte and total and differential leukocyte counts, hemoglobin levels, hematocrit, and mean corpuscular volume measured) were observed. Serum lactate dehydrogenase and aspartate aminotransferase levels were decreased and serum creatinine levels were increased in the males exposed to 100 or 200 mg/L; no other alterations in serum chemistry parameters were consistently found. A significant increase in incidence of nasal lesions (goblet cell hyperplasia and inflammation of nasal turbinates) was found in males exposed to 25 mg/L and in females at 100 mg/L. The study authors postulated that these lesions were likely caused by inhalation of chlorine dioxide vapors at the drinking water sipper tube or from off-gassing of the vapors after drinking rather than ingestion of the drinking water. Thus, 25 mg/L (2 mg/kg-day) can be described as a lowest-observed-adverse-effect level (LOAEL), but the toxicological significance of the nasal lesions is not known. Respiratory tract pathologies have not been reported in other oral studies and the effect may possibly be an artifact of treatment.
Effects on the liver:
NOAEL: No-observed-adverse-effect-level.
Glucose-6-phosphate is the first intermediate of glucose metabolism and plays a central role in the energy metabolism of the liver. It acts as a hub to metabolically connect glycolysis, the pentose phosphate pathway, glycogen synthesis, de novo lipogenesis, and the hexosamine pathway.
Moore and Calabrese (1982) also examined the hematotoxicity of chlorite. In this study, groups of 11–23 A/J or C57L/J mice (sex not specified) were exposed to 0, 1, 10, or 100 ppm sodium chlorite (0, 0.75, 7.5, or 75 ppm chlorite) in drinking water for 30 days. Significant increases in mean corpuscular volume, osmotic fragility, and glucose-6-phosphate activity were observed in both strains of mice exposed to 100 ppm; no other alterations in hematologic parameters were observed.This study identifies a NOAEL of 10 ppm sodium chlorite (1.9 mg/kg-day chlorite using a reference body weight of 0.0316 kg and water intake of 0.0078 L/day) 14 and a LOAEL of 100 ppm sodium chlorite (19 mg/kg-day) for hematologic effects in mice exposed to chlorite in drinking water for 30 days.
Research data on ClO2 induced carcinogenicity is lacking and findings in this study are somewhat conflicted.
Regarding tumours, it would be interesting to independently confirm baseline incident rates in the control animals they used as selective use of baseline data may mask the signalling of adverse events, whether by accident or design10.
For mice, daily doses of 0, 48, and 95 mg sodium chlorite/kg-day (0, 36, and 71 mg chlorite/kg-day) were calculated by EPA (1994d). In the mice, there were no significant chlorite-related alterations in survival or body weight gain; increased mortality was observed in the male control group, which was attributed to severe fighting. Significant increases in liver and lung tumors were observed in the male mice. Incidence of hyperplastic nodules in the liver was significantly increased in the low- and high-dose groups relative to controls (3/35 [reported as 6/35 in Yokose et al., 1987], 14/47, 11/43, in the control, low-, and high-dose groups, respectively) and combined incidence of liver hyperplastic nodules and hepatocellular carcinoma was increased in the low-dose group (7/35, 22/47, and 17/43, respectively). Incidence of lung adenoma (0/35, 2/47, and 5/43, respectively) and combined incidence for lung adenoma and adenocarcinoma (0/35, 3/47, and 7/43, respectively) were significantly increased in the high-dose group compared with controls. The study authors noted that incidences of liver hyperplastic nodules and lung adenomas in the treated animals were within the range of historical controls in their laboratory and in the National Toxicology Program laboratories. The high mortality in the control males because of fighting may have contributed to the low tumor incidence in the concurrent control group, making statistical comparisons between concurrent controls and treated animals difficult to interpret. In the female mice, the only significant alteration in tumor incidence was a significantly lower incidence of malignant lymphoma/leukemia in the high-dose group (7/47, 5/50, 1/50, respectively). This study is considered inadequate for assessing carcinogenicity because of the relatively short exposure duration (80 weeks) and the high incidence of early mortality in the concurrent control males from excessive fighting.
Oral effects of ClO2 on reproduction and development. For the other studies and for brevity please refer to the source pdf:
Taylor and Pfohl (1985) exposed groups of 13–16 female Sprague-Dawley rats to 0 or 100 ppm chlorine dioxide in drinking water (0 or 14 mg/kg-day calculated using a reference body weight of 0.35 kg and water intake of 0.046 L/day) for 14 days prior to breeding and throughout gestation and lactation. Groups of male pups from unexposed dams were administered 0 or 14 mg/kg chlorine dioxide via gavage from postnatal days 5 to 20. No significant alterations in maternal or pup body weights were observed in the group receiving 100 ppm in the drinking water. A significant decrease in whole brain weight, primarily because of a decrease in cerebellar weight, was observed in the 21-day-old offspring of dams receiving 100 ppm in the drinking water. A decrease in cerebellar total DNA content also was observed; the difference was caused by a decrease in total number of cells rather than in cell density. A nonsignificant decrease in locomotor activity (assessed at 10–20 days of age) was observed in the 100 ppm offspring. A significant decrease in exploratory behavior was observed in the 100 ppm offspring at 60 days of age. In the pups receiving gavage doses of chlorine dioxide, significant decreases in body weight, absolute and relative whole brain and forebrain weights, and forebrain DNA content and total cell number were observed in the 21-day-old pups; cerebellum and forebrain DNA content and total cell number were also significantly decreased in the 11-day-old pups. Significant decreases in home cage and wheel-running activity at ages 18–19 and 10 days, respectively, also were observed in the pups receiving gavage doses of chlorine dioxide. Thus, the LOAEL for neurobehavioral effects, decreased brain weight, and cell number in the offspring of rats exposed to chlorine dioxide in drinking water and in rats postnatally exposed to chlorine dioxide via gavage is 14 mg/kg-day.
Caution is warranted here due to a potential conflict of interest, and several flaws in the methods and statistical analysis used were noted:
4.3.2. Chlorite
The Chemical Manufacturers Association (CMA) conducted a two-generation study to examine reproductive, developmental neurotoxicity, and hematologic endpoints in rats exposed to sodium chlorite (CMA, 1996). Thirty male and 30 female Sprague-Dawley rats of the OFA(SD)IOPS-Caw strain (F0) generation received drinking water containing 35, 70, or 300 ppm sodium chlorite (concentrations of sodium chlorite in the drinking water were apparently adjusted to compensate for the 81.4% purity of the test material) for 10 weeks and were then paired (1M:1F) for mating. A similar group received purified water and served as controls. Males were exposed throughout mating and then were sacrificed. Exposure for the females continued through mating, pregnancy, and lactation until necropsy following weaning of their litters. Sodium chlorite concentrations were adjusted downward during lactation to offset increases in the volume of water consumed so that a constant intake (mg/kg-day) could be maintained. Twenty-five males and females from each of the first 25 litters to be weaned in a treatment group were chosen to produce the F1 generation. The F1 pups were continued on the same treatment regimen as their parents. At approximately 14 weeks of age, they were mated to produce the F2a generation. Because of a reduced number of litters in the 70 ppm F1-F2a generation, the F1 animals were remated following weaning of the F2a to produce the F2b generation. Pregnant F1 females were allowed to litter and rear the F2a and F2b generations until weaning at postnatal day 21.
…There were reductions in water consumption, food consumption, and body weight gain in both sexes in all generations at various times throughout the experiment (e.g., during premating, pregnancy, gestation, postweaning), primarily in the 70 and 300 ppm groups. The authors attributed these reductions to lack of palatability of the drinking water solution, but did not show data to support this contention. Significant alterations related to treatment at 300 ppm include reduced absolute and relative liver weight in F0 females and F1 males and females, reduced pup survival (increase in number of pups found dead and/or killed prematurely during lactation) and reduced body weight at birth and throughout lactation in F1 and F2 rats, lower thymus and spleen weight in both generations, lowered incidence of pups exhibiting normal righting reflex and with eyes open on postnatal day 15, alteration in clinical condition in F2 animals chosen for neurotoxicity, decrease in absolute brain weight for F1 males and F2 females, delay in sexual development in males (preputial separation) and females (vaginal opening) in F1 and F2 rats, and lower red blood cell parameters in F1 rats. The reported alterations in pup sexual maturation measures might be due to reduced pup body weight, but a definitive conclusion cannot be drawn. In the 70 ppm groups, reduced absolute and relative liver weight in F0 females and F1 males was observed.
…The CMA (1996) study is adequate in that it was conducted with sufficient numbers of animals of both sexes and examined numerous endpoints. The study is acceptable and consistent with EPA testing guidelines that were in effect at the time of the study (U.S. EPA, 1991). However, there are several limitations to this study. Lack of pair-watered and pair-fed control animals confounds the results and precludes definitive conclusions as to whether the alterations in food and water consumption and body weight are related to water palatability or a direct toxic effect of the agent. Developmental landmarks (e.g., vaginal opening in F2a group) were not reported for all groups. Grip strength and landing foot splay were not included in the FOB. Discontinuation of exposure for the animals undergoing neurotoxicity testing minimizes the likelihood of finding a positive effect and precludes comparison of the data with those of other rats with continued exposure. Although the study employed an exposure regimen consistent with testing guidelines and should potentially detect adverse effects on the developing nervous system, discontinuation of exposure after weaning reduces the opportunity to detect neurological effects from continuous or lifetime exposures similar to those expected from lifetime drinking water exposure in humans. Interpretation of the neurobehavioral tests is limited. The report lacks detailed descriptions of experimental methods (e.g., size of the arena, length of observations) and positive control data (including estimates of variability) for the FOB. Positive control studies for the motor activity and E-maze studies used high doses of the validation chemicals, were not adequate to show the sensitivity of the methods, and showed only that effects of the chemicals at maximally toxic doses could be recognized. Variability in the startle response data was high. The high variability and problems in calibrating and operating the automated startle apparatus (as presented in the report) would tend to decrease the sensitivity of the test to detect a difference between control and treated groups, because differences in startle amplitude would have to be larger to attain statistical significance. In some cases, inappropriate statistical analyses were applied. For example, repeated-measures techniques were apparently not used to account for the fact that the rats were tested repeatedly, and it is not clear how nonparametric rank data were analyzed or why a log transformation was applied to the learning data. The NOAEL for this study is 35 ppm (2.9 mg/kg-day chlorite) and the LOAEL is 70 ppm (5.9 mg/kg-day chlorite) based on lowered auditory startle amplitude and altered liver weights in two generations.
Other studies into carcinogenicity do give indications of cellular proliferation being induced, but again the data is mixed:
4.4.1.1. Chlorine Dioxide
The potential for chlorine dioxide to induce proliferative epidermal hyperplasia was examined by Robinson et al. (1986). Groups of five dorsally shaved female SENCAR mice were placed in chambers filled with 0, 1, 10, 100, 300, or 1,000 ppm liquid chlorine dioxide; the chambers were designed to prevent the head from getting wet and to prevent inhalation of vapors. The animals were exposed 10 minutes/day for 4 days. A significant increase in interfollicular epidermal thickness was observed in the 1,000 ppm group, but not at the lower concentrations. Increases in total cell numbers and basal cell numbers in skin sections were observed in both the 300 and 1,000 ppm groups. In a second study, groups of 40 mice were immersed in 0 or 1,000 ppm chlorine dioxide for 10 minutes; animals (5/group) were killed 1, 2, 3, 4, 5, 8, 10, or 12 days postexposure. A significant increase in interfollicular epidermis thickness was observed at all time periods, with the highest values at 10 and 12 days postexposure. The authors concluded that even short-term dermal exposure to high concentrations of chlorine dioxide is capable of inducing hyperplastic responses in the mouse skin.
Miller et al. (1986) tested the carcinogenic potential of drinking water disinfected with chlorine dioxide using three short-term assays. Following disinfection with chlorine dioxide, the water samples (containing 0.5 mg/L chlorine dioxide residue) were concentrated 2,000× or 4,000× using a macroreticular resin process. In a mouse initiation-promotion assay, groups of 14–34 SENCAR mice (sex not specified) were orally administered 0.5 mL of the 4000× concentrate in 2% emulphor 3 times/week for 2 weeks followed by topical exposure to 1.0 :g 12- tetradecanylphorbal-13-acetate (TPA) in acetone applied to the dorsal skin 3 times/week for 20 weeks and then sacrificed. No significant increases, compared with vehicle controls, in the number of skin tumors or the number of tumors per animal were observed.
In a lung adenoma assay (Miller et al., 1986), groups of 20 male and 20 female Strain A mice received 0.25 mL gavage doses of 2000× or 4000× concentrates in 2% emulphor 3 times/week for 8 weeks followed by a 16-week observation period. The number of animals with lung adenomas and the number of adenomas per animal were not significantly altered compared with vehicle controls. Miller et al. (1986) also examined the development of liver foci in rats in a short-term assay. In this study, groups of partially hepatectomized rats received a single dose of concentrated water (chlorine dioxide concentration not reported) in 2% emulphor followed 1 week later by administration of 500 ppm sodium phenobarbital in drinking water for 56 days; 26 animals were sacrificed on day 70. A control group received nondisinfected water. No significant increases in incidence of (-glutamyltranspeptidase foci were observed.
Tumour incidences of 30% and 25% “were not statistically significant”? I would want to see confirmation of this as out of 20 replicants it requires further explanation:
4.4.1.2. Chlorite
Kurokawa et al. (1984) also conducted dermal carcinogenicity studies. In a study to assess the ability of chlorite to act as a complete carcinogen, groups of 20 female SENCAR mice were exposed twice weekly for 51 weeks to 20 mg/mL sodium chlorite in acetone. The solution (0.2 mL; 100 mg/kg sodium chlorite per application) was applied to the shaved backs of the mice. The sodium chlorite exposure did not result in increased tumor incidence. To test the ability of chlorite to act as a tumor promoter, a single initiating dose of 20 :mol of dimethylbenzanthracene (DMBA) was applied to the skin of 20 SENCAR mice. The DMBA application was followed by a 51-week exposure to sodium chlorite (as described for the complete carcinogen study). Tumor incidence was 6/20 (30%) compared with 0/20 in mice that received DMBA followed by acetone treatments for 51 weeks. Squamous cell carcinomas were observed in 5/20 animals in the chlorite group. However, the results were not statistically significant.
Binding to dietary iodine & consequential deficiency may explain effects on the thyroid and metabolism:
4.4.3. Mechanistic Studies
EPA (1994d) has extensively discussed the mechanism of action whereby chlorine dioxide and chlorite produce hematologic and systemic effects. The mechanisms are still incompletely understood. Oxidative damage to the erythrocyte and production of methemoglobin are most likely related to their properties as oxidants (U.S. EPA, 1994d). Chlorite is thought to be the intermediate species responsible in many of the hematologic effects of chlorine dioxide because of its more efficient production of methemoglobin, depletion of red blood cell (RBC) glutathione, and alteration of erythrocyte fragility.
In a series of experiments, Bercz and co-workers (1982, 1986); and Harrington et al. (1986) suggested that chlorine dioxide increases binding of dietary iodide to gastrointestinal tissue and contents, producing a functional iodide deficiency. Bercz et al. (1982) found decreased levels of circulating thyroxine in monkeys drinking water containing > 9.5 mg/kg-day chlorine dioxide, but not 44 mg/kg-day chlorite, for 4–6 weeks. In a follow-up study, Harrington et al. (1986) demonstrated increases in thyroid iodide uptake and a rebound in thyroxine levels in monkeys 1 year after an 8-week exposure to approximately 5 mg/kg-day chlorine dioxide in drinking water. Unlike monkeys, rats showed dose-related declines in thyroxine levels and no alteration in thyroid iodide uptake following an 8-week exposure to 10 mg/kg-day chlorine dioxide in drinking water.
Whether either or both of these mechanisms are operable in inducing reproductive, developmental, and neurodevelopmental effects is not known. One could also speculate that hypothyroidism, induced by chlorine dioxide alteration of iodide uptake in the gastrointestinal tract, might contribute to alterations in maternal or neonatal behavior. Alternative, as yet unknown mechanisms are also plausible because few definitive mechanistic data are available. Additional research is needed to understand whether the parent chlorine dioxide and/or its oxychlorine degradation products induce delays and alterations in fetal/neonatal neurodevelopment and behavior through disturbance in maternal thyroid function or directly within the embryo itself.
Official classifications as carcinogenic substances:
Lack of data does not exclude the possibility, and reverse mutations have been associated with cancer development.
These findings suggest that developing cancer cells undergo sequential changes that enable the "nontumor" cells to acquire a wide range of forward mutations including ones that are essential for oncogenicity, followed by revertant mutations in the "paratumor" cells to avoid growth retardation by excessive mutation load. Such utilization of forward-reverse mutation cycles as an adaptive mechanism was also observed in cultured HeLa cells upon successive replatings.
Under the current guidelines (U.S. EPA, 1986a), chlorine dioxide is classified as Group D, not classifiable as to human carcinogenicity because of inadequate data in humans and animals. Under the draft Carcinogen Assessment Guidelines (U.S. EPA, 1996a), the human carcinogenicity of chlorine dioxide cannot be determined because no satisfactory human or animal studies assessing the chronic carcinogenic potential of chlorine dioxide were located.
No human or animal studies assessing the carcinogenic potential of chlorine dioxide were located. The carcinogenic potential of concentrates prepared from drinking water treated with chlorine dioxide was tested by Miller et al. (1986). The concentrates did not increase incidence of lung adenomas in Strain A mice, skin tumor frequency in mice, or incidence of gamma-glutamyl transpeptidase positive foci (a measure of preneoplastic changes) in rat livers. Robinson et al. (1986) found significant increases in skin thickness in SENCAR mice immersed in chlorine dioxide, suggesting that high concentrations of chlorine dioxide are capable of inducing hyperplastic responses in the mouse skin. Both positive and negative results have been found in genotoxicity studies of chlorine dioxide. Exposure to chlorine dioxide did not induce chromosomal aberrations in vitro, but it did increase occurrence of reverse mutations (Ishidate et al., 1984). In vivo assays did not find increases in micronucleus induction, chromosomal aberrations, or sperm-head abnormalities following oral exposure (Meier et al., 1985), but they did find increases in micronuclei induction after intraperitoneal injection (Hayashi et al., 1988).
4.6.2. Chlorite
Under the current guidelines (U.S. EPA, 1986a), chlorite is classified as Group D, not classifiable as to human carcinogenicity because of inadequate data in humans and animals. Under the draft Carcinogen Assessment Guidelines (U.S. EPA, 1996a), the human carcinogenicity of chlorite cannot be determined because of a lack of human data and limitations in animal studies. No human studies assessing the carcinogenic potential of chlorite were located.
…Chlorite has been shown to be mutagenic in in vitro assays for reverse mutations and chromosome aberrations (Ishidate et al., 1984) and in an in vivo assay of micronucleus induction in which mice received an intraperitoneal injection of sodium chlorite (Hayashi et al., 1988). In vivo assays for micronucleus induction, chromosome aberrations, and sperm-head abnormalities were negative in mice receiving gavage doses of chlorite for 5 days (Meier et al., 1985; Hayashi et al., 1988).
Other dose-response assessments:
5.1. ORAL REFERENCE DOSE (RfD)
5.1.1. Choice of Principal Study and Critical Effect—With Rationale and Justification
In general, human studies have not found adverse effects in individuals consuming low concentrations (0.04–0.15 mg/kg-day) of chlorine dioxide or chlorite in experimental studies (Lubbers et al., 1981, 1982, 1984a) or consuming drinking water disinfected with chlorine dioxide (Michael et al., 1981; Tuthill et al., 1982). An epidemiology study by Kanitz et al. (1996) found increases in the risk of several developmental effects (neonatal jaundice, small cranial circumference, and shorter body length) in a community with chlorine dioxide-disinfected drinking water. However, the Kanitz et al. (1996) study has numerous limitations (including multiple chemical exposures; lack of exposure data; lack of control for smoking, age, and nutritional habits; and atypical control data), making it difficult to interpret the study findings.
In animals, the most sensitive effect following oral exposure to chlorine dioxide or chlorite is neurodevelopmental delay. In utero exposure to chlorine dioxide or postnatal gavage administration of chlorine dioxide has resulted in altered brain development (decreases in brain weight, protein content, and cell number) (Taylor and Pfohl, 1985; Toth et al., 1990) and decreased locomotor or exploratory activity (Orme et al., 1985; Taylor and Pfohl, 1985; Mobley et al., 1990). The LOAEL for these effects is 14 mg/kg-day chlorine dioxide (Orme et al., 1985; Taylor and Pfohl, 1985; Mobley et al., 1990; Toth et al., 1980); Orme et al. (1985) identified a NOAEL of 3 mg/kg-day. Neurobehavioral effects (lowered auditory startle amplitude, decreased brain weight, and decreased exploratory activity) are also the most sensitive endpoints following oral exposure to chlorite (Mobley et al., 1990; CMA, 1996). The LOAEL identified in the Mobley et al. (1990) developmental toxicity study and the CMA (1996) two-generation developmental toxicity study is 6 mg/kg-day chlorite; Mobley et al. (1990) also found significant decreases in exploratory activity at 3 mg/kg-day, but the difference between activity in this group and the controls was small. Thus, the NOAEL for neurobehavioral effects is 3 mg/kg-day chlorite. At higher concentrations (22–28 mg/kg-day chlorite), decreases in fetal/pup body weight have also been observed in mice and rabbits (Moore and Calabrese, 1982; Moore et al., 1980; Harrington et al., 1995b).
Human hazard potential:
In general, human ingestion studies have found no adverse effects in adults and neonates living in areas with chlorine dioxide-disinfected water. However, these studies are fraught with methodological problems, such as lack of characterization of exposure to other agents in the drinking water and control of potential confounding factors. These studies do little to confirm a possible association between exposure to chlorine dioxide and chlorite and adverse reproductive or developmental outcome in humans. Inhalation exposure to chlorine dioxide results in 38 respiratory irritation in humans. However, these studies also poorly characterize exposure, and the occupational exposure studies involve concomitant exposure to chlorine and/or sulfur dioxide.
Animal toxicity databases for chlorine dioxide and chlorite is fairly comprehensive, composed of subchronic and chronic studies, reproductive and developmental studies, and toxicokinetic and mechanistic information. Multiple animal studies have shown similar alterations in neurodevelopmental endpoints, such as brain weight and behavioral measures. The majority of these studies have used sufficient numbers of animals and employed routes of exposure (gavage and drinking water) relevant to human exposure. The majority of the developmental studies have utilized rats and have shown a fairly consistent definition of the NOAEL/LOAEL. Reproductive studies in male animals are not consistent in demonstrating alterations in spermatogenic indices, that is, abnormal morphology or motility; however, reported effects seem to appear at doses higher than the adverse developmental effects. Similarly, clinically or toxicologically significant alterations in hematologic parameters occur at higher doses. The mode of action for induction of adverse neurodevelopmental effects is not known. It is also not known whether the rat is an adequate model for toxicity of chlorine dioxide and chlorite in humans. However, this species is widely used to characterize reproductive and developmental effects in humans.
…Areas of scientific uncertainty in this assessment include the mode of action of chlorine dioxide and chlorite in producing adverse effects on multiple organ systems, including reproductive, developmental, and hematologic effects. Inherent in the uncertainty over the mode of action is identification of the susceptible populations or subgroups, and additional research in this area would help to better quantify the additional risk to these groups. Well-designed and conducted epidemiologic studies in communities with drinking water disinfected with these chemicals would decrease uncertainty in the utilization of animal models for determination of human health effects.
Case Studies
So we know from many in vivo studies that comparatively low doses of ClO2 administered orally may be associated with adverse effects on development, liver function and neurological function, as assessed using several endpoints. And there are significant pointers towards hyperplasia and tumours, which the researchers have explained away as being at normal levels or not significant.
Objectives: Individual epidemiological investigations into the association between chlorination by-products in drinking water and cancer have been suggestive but inconclusive. Enough studies exist to provide the basis for a meaningful meta-analysis.
Methods: An extensive literature search was performed to identify pertinent case-control studies and cohort studies. Consumption of chlorinated water, surface water, or water with high levels of chloroform was used as a surrogate for exposure to chlorination by-products. Relative risk estimates were abstracted from the individual studies and pooled.
Results: A simple meta-analysis of all cancer sites yielded a relative risk estimate for exposure to chlorination by-products of 1.15 (95% CI: 1.09, 1.20). Pooled relative risk estimates for organ-specific neoplasms were 1.21 (95% CI: 1.09, 1.34) for bladder cancer and 1.38 (95% CI: 1.01, 1.87) for rectal cancer. When studies that adjusted for potential confounders were pooled separately, estimates of relative risks did not change substantially.
Conclusions: The results of this meta-analysis suggest a positive association between consumption of chlorination by-products in drinking water and bladder and rectal cancer in humans.
Iodine deficiency may well make a significant contribution to some of the observed pathologies via thyroxine deficiency and further endocrine effects. However, more studies are needed, especially with humans.
So what outcomes have been observed?
In this report from 2021 by Arellano-Gutiérrez et al an adult experienced intestinal perforation after ingesting ClO2 daily over a prolonged period as a prophylactic12.
10ml of ClO2 in 1000ml of water is a concentration of 1%, or 10 grams. We don’t know the patients’ weight but using the previous figure of 70kg this equates to 143mg/kg, far above the identified NOAEL/LOAEL thresholds seen in the in vivo studies discussed previously.
Unfortunately the damage was too severe to avoid the eventual death of the patient:
Case presentation
We present the case of a 65-year-old male patient, who sought medical care in our institution with a 1-week history of abdominal pain, nausea, vomiting, and melena on two occasions in the last 24 h. The patient denied chronic degenerative diseases. Surgical history of hemorrhoidectomy 28 years ago. Tobacco smoking history of 6 pack-year and denied having suffered COVID-19 disease. Also, the patient referred ingestion of chlorine dioxide in the last 9 months as a preventive therapy for coronavirus disease, with a gradual increase in the dose until reaching the consumption of 10 ml per day, diluted in 1 L of water and ingested in a period of 8 h. The exact chlorine dioxide solution concentration was unknown, although it was referred as high.
Physical examination at the time of admission revealed a bad general condition, with drowsiness, hypotension and tachycardia, and abdominal examination with data of peritoneal irritation, distention, and absent peristalsis. The patient was found to have a blood pressure of 75/40 mmHg, a pulse rate of 120 beats/min and a respiratory rate of 23 breaths/min, mildly pyrexial at 37.5 °C. The blood examination reported hemoglobin 12.2 g/dL, leukocytes 14.10 (10 *3 µL), platelets 241.9 (10 *3 µL), electrolyte imbalance with potassium 6.1 mEq/L and sodium 126 mEq/L, liver function tests in normal parameters.
Abdominopelvic computed tomography was performed, which revealed abundant free fluid in the abdominal cavity, peri-pancreatic space, in both paracolic gutters and pelvic hollow with densities of 10 HU. The presence of pneumoperitoneum secondary to hollow viscus rupture was also evident (Fig. 1).
Surgical approach was conducted with exploratory laparotomy, finding free fluid in the abdominal cavity (approximately 2.5 L), with jejunum perforation adjacent to the fixed loop. Intestinal resection was performed 80 cm from the jejunum with bowel loop closure; gastrostomy and jejunostomy were performed (Fig. 2). Pathological examination of the specimen revealed ulceration and denudation of the epithelium with severe changes due to tissue necrosis in the mucosa, in addition to acute and severe chronic inflammation with areas of transmural extension (Fig. 3). The clinical status of the patient was critical after surgery, with presence of septic shock, SOFA score 13 points (mortality > 95.2%), APACHE score 21 points (mortality of 30%), developing liver and kidney failure, as well as neurological deterioration requiring orotracheal intubation. Hemodiafiltration was indicated by the hemodialysis service, nevertheless, the patient was not in optimal clinical conditions. 48 h after the surgery, he presented cardiorespiratory arrest. Unfortunately, despite early cardiopulmonary resuscitation in the intensive care unit, and due to multiple organ failure and poor clinical condition, irreversible systemic deterioration led to the patient’s death.
Fig 2. Small bowel resected segment (jejunum) measuring 40.0 cm. Full thickness necrosis and perforation in the anti-mesenteric area is evident (A). Jejunal perforation with regular edges measuring 1.0 × 1.0 cm (B)https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8522852/figure/Fig2/
Fig 3. Histopathological findings. Ulceration and denudation of the epithelium, with the presence of conserved epithelial cells. Serous layer with destruction of the parenchyma (A). Chronic inflammation of the serous layer with neutrophilic infiltrate. Inflammation and severe changes due to tissue necrosis in the mucosa are present (B). Muscle layers with chemical destruction and neutrophilic infiltration in the serous layer (C)https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8522852/figure/Fig3/
In the next report by Medina-Avitia et al, also from 2021, a 55 year old male patient developed acute kidney injury (AKI) and disseminated intravascular coagulation (abnormal blood clotting throughout the body's blood vessels) after prophylactic ingestion of ClO2.
He needed kidney dialysis 48 hours after admission, despite initial therapy with IV fluids and diuretics as these failed to improve markers of kidney function13.
What is anuria? Anuria literally means no urine, or without urine. In practical terms, it means that your kidneys aren't producing urine (pee) or that you aren't peeing (anuresis). Anuria's the most severe form of oliguria, which means that your kidneys aren't producing enough urine.
A 55‐year‐old male with a clinical history of hypertension and type 2 diabetes attended the emergency department after consumption of chlorine dioxide.The patient decided ingestion of a nonspecified dilution as prevention for COVID‐19 and after 5 days he developed nausea, vomiting, and altered mental state; no fever, dyspnea, or other symptoms were referred. Initial examination showed dehydration and inattention. No edema was found. Initial work‐up reported glucose of 640 mg/dl serum creatinine of 4.6 mg/dl, blood urea of 236 mg/dl, hemoglobin of 12.3 g/dl, total leucocyte counts 4100/mm3, and platelet count 36,000/mm3, elevated prothrombin time (PT), INR (1.4), and d‐dimer (15.43 mg/L), consistent with the diagnosis of disseminated intravascular coagulation (DIC). Peripheral smear was normal, methemoglobin levels were not available. Metabolic acidosis with secondary respiratory alkalosis was found. Hepatic function was remarkable. Chest X‐ray and brain CT‐scan were normal. No infectious etiologies were identified. The patient persisted with disorientation and progressed to anuria despite intravenous fluids and diuretic therapy after 48 h. He received one session of hemodialysis (HD) with decreased serum creatinine to 1 mg/dl and blood urea to 73 mg/dl, as well as notable improvement in alertness and uresis. Last platelet count was 100,000/mm3. No more HD sessions were offered, and he was discharged after 6 days of hospitalization (Figure 1).
Thus, emerging side effects are expected and physicians must be aware of these complications.
The next case study is from 2020. Andrés Aguilar Silva reports on how a patient with severe COVID-19 presented with respiratory failure secondary to oral and intravenous use of ClO214:
Pneumonitis is literally inflammation of lung tissue, and pneumonia is a type of pneumonitis. When described as such it generally means that the type of inflammation is non-infectious15.
Abstract
In the context of the COVID 19 pandemic, chlorine dioxide treatment has been promoted as a treatment, however health authorities in several countries including Mexico have warned of serious adverse reactions that put the lives of people at risk. they consume it. We report the case of a patient with COVID 19 infection who presents with respiratory failure secondary to oral and intravenous use of chlorine dioxide, requiring intubation, with multiple organ failure and ended with the death of the patient 5 days later.
…Chlorine dioxide and sodium chlorite react rapidly in human tissues and, if ingested, can cause irritation of the mouth, esophagus and stomach, with a severe irritative digestive picture, with the presence of nausea, vomiting and diarrhea, in addition of serious hematological disorders (methemoglobinemia, hemolysis, etc.), cardiovascular and kidney. The decrease in blood pressure can lead to serious symptoms such as respiratory complications due to the modification of the blood's ability to transport O2. Additionally, inhalation through nebulizers can cause pulmonary edema, bronchospasm, chemical pneumonitis and glottis edema, and even cause death if exposures are above the occupational exposure limit value. Long-term exposure can lead to chronic bronchitis and dental erosions.
Websites that sell chlorine dioxide products generally describe the product as a liquid that contains 28% sodium chlorite in distilled water. Product instructions instruct consumers to mix sodium chlorite solution with citric acid, such as lemon or lime juice, or another acid, such as hydrochloric acid, before drinking. In many cases, sodium chlorite is sold as part of a kit with a citric acid "activator". When the acid is added, the mixture turns into chlorine dioxide, a powerful bleaching agent that has caused serious and life-threatening side effects [3-5].
An example of one of these kits. To be fair in this case it does make it quite clear that it is not suitable for human consumption.
However, from one of the reviews (translated from Spanish):
"Preventive of all kinds of diseases. I've been using it for 10 years and it works."
Another said:
“This makes the perfect MMS, most people will want to know this.”
Related to ClO2, MMS refers to “Miracle Mineral Solution”, “Miracle Mineral Supplement” or “Master Mineral Solution”. MMS generally contains a high concentration of sodium chlorite and "are promoted as effective destroyers of pathogens, fungi, disease, bacteria and viruses, and more recently, COVID-19".
The name was coined by former Scientologist[9] Jim Humble in his 2006 self-published book, The Miracle Mineral Solution of the 21st Century.[10] Humble claims that the chemical can cure HIV, malaria, hepatitis viruses, the H1N1 flu virus, common colds, autism, acne, cancer and other illnesses. There have been no clinical trials to test these claims, and they come only from anecdotal reports and Humble's book.[11][12] In January 2010, The Sydney Morning Herald reported that one vendor admitted that they do not repeat any of Humble's claims in writing to circumvent regulations against using it as a medicine.[13] Sellers sometimes describe MMS as a water purifier to circumvent medical regulations.[14] The International Federation of Red Cross and Red Crescent Societies rejected "in the strongest terms" reports by promoters of MMS that they had used the product to fight malaria.[15] In 2016, Humble said that MMS "cures nothing".[16] In August 2019, the Food and Drug Administration repeated a 2010 warning against using MMS products, describing it as "the same as drinking bleach".[2]
58-year-old female, hypertensive for 15 years, began a current condition approximately 14 days ago with general symptoms, asthenia, adynamia, non-productive cough, quantified thermal rises up to 39 degrees, for which she goes to a private physician who begins treatment for oseltamivir base + dexamethasone + azithromycin + ceftriaxone + enoxoparin + colchicine without referring specified time. RT PCR was performed for SARS COV2 on August 18, 2020, which was reported positive, as well as a private chest tomography with ground-glass image suggestive of atypical pneumonia with severe CORADS 5 disease (Figure 1), so continued treatment. On August 20, 2020, she presented dyspnea on exertion, which was exacerbating, for which she went to the emergency room of the General Hospital of Boca del Rio, Mexico where she received unspecified in-hospital treatment requesting voluntary discharge one day after hospitalization [4,5]. Maintaining established treatment at home and oxygen saturation greater than 90% to be referred by relatives. On August 24, 2020, due to persistence of dyspnea and hypoxemia despite the use of supplemental oxygen at home, he decided to manage with complementary therapy of the type of carbon dioxide ingested orally and intravenously (it is unknown who administered the drug and under indication of which personnel of health) refers to oral intake of 1000 ml of chlorine dioxide solution plus intravenous administration of 500 ml of 0.9% saline solution with 28% sodium chlorite, presenting sudden respiratory deterioration, decreasing oxygen saturation up to 60% [5-8]. She was transferred to the emergency room where hypertensive uncontrol was documented with TA 183/88, tachypnea with 38 bpm, tachycardia of 121 bpm, with SatO2 of 60%, being intubated on the second attempt by means of direct video laryngoscopy initiating invasive mechanical ventilation after sedation, her SOFA of Admission was 13 points, APACHE II 26 points, NEWS 2 11 points, with blood gas reporting PH 7.28, PCO2 58, PO2 136, HCO3 24.4, FIO2 100. Within the physical examination, excoriations at the level of the lips, diffuse bilateral rales, with dullness to percussion, hippocratic fingers, the patient developed within the first hours fluid-refractory hypotension for which norepinephrine was started. anticoagulation, broad spectrum antibiotic, steroid with hydrocortisone 50 mg IV every 6 hours, as well as data of acute liver failure with elevation in total bilirubin, and transaminases and DHL, with marked leukocytosis, a chest tomography was performed after ingestion of carbon dioxide [8,9]. chlorine reporting diffuse bilateral alveolar pattern (Figure 2) suspecting secondary aspiration pneumonitis, likewise airway injury generating pneumomediastinum (Figures 3 and 4), there was an increase in fluid intake, however the patient presented acute kidney injury AKIN III, renal replacement therapy was requested, however due to the severity of the patient, was reported no candidate (Table 1). Death presented 5 days after the ingestion of chlorine dioxide.
To conclude this Substack and hopefully act as warning to others is this bizarre case report, from January 202117.
The question here is just what clinical trials data was the patient's doctor using as a reference to indicate the IV administration of ClO2? And the family still do not question the use of ClO2:
Man dies after judge forces clinic to use unproven COVID treatment
Buenos Aires — An Argentinian judge compelled a private clinic to administer chlorine dioxide, used as a powerful disinfectant, to a coronavirus patient who died Monday in a case medical doctors have labelled "a scandal." The U.S. Food and Drug Administration (FDA) and other agencies warn that chlorine dioxide, touted as a "miracle cure" online, can be hazardous to human health if consumed.
In the wake of President Trump suggesting that disinfectants might be injected to treat COVID-19, a number of Americans were hospitalized for ingesting cleaning agents, and at least three people were charged with criminal offenses for selling chlorine-based products as remedies for the disease.
The stepson of the patient brought a legal bid last Thursday, the day after his mother died of COVID-19, for the compound to be given to her critically ill husband.
A judge granted the request the same day and ordered the Otamendi y Miroli clinic in Buenos Aires to administer the substance, prescribed by the patient's doctor.
The clinic unsuccessfully appealed against the ruling, and gave the man the substance while stressing it would not bear responsibility for any negative outcome.
The patient, a 92-year-old man who was in critical condition from the virus, died Monday, the family's lawyer confirmed.
The FDA has warned that consumption of chlorine dioxide products can "jeopardize a person's health," have no proven effectiveness against COVID-19, and have been known to cause respiratory and liver failure among other ill effects.
The Pan American Health Organization, the Argentine Society of Infectology and the country's National Administration of Drugs, Foods and Medical Devices have also issued warnings against the use of chlorine products to treat COVID-19.
The judge ruled that giving the treatment threatened no "serious harm" to the clinic, but could, conversely, "avoid the worsening" of the patient's condition.
Medical doctors have lambasted the decision.
"Judicial aberration and a scandal"
"For a judge to decide that a doctor has to administer a substance for which there is no scientific evidence is really worrying, especially when it is in intravenous form," said Omar Sued, president of the Argentine Society of Infectology.
"It is not the decision of a judge to administer a medication he does not know to a patient. It is not his role."
Ignacio Maglio, a lawyer for the Argentinian health NGO Fundacion Huesped, said the case amounted to judicial overreach, a "judicial aberration and a scandal."
Chlorine dioxide is used to disinfect medical and laboratory equipment, to treat water at low concentrations, or as a bleach.
The family's lawyer told the television channel C5N that his client will sue the Otamendi clinic as they consider it responsible for the patient's death, because it "delayed the treatment."
"The man died of an in-hospital infection and because of the delay in treatment," the lawyer said.
As to why IV administration has been used, there is a paper from 2022 by Miller et al that has been cited from a phase 2B clinical study that used a formulation of pH stabilized, purified chlorite called “NP001”18. But it did not investigate antiviral properties, it was looking for effectiveness against ALS, amyotrophic lateral sclerosis.
This is also known as motor neurone disease or Lou Gehrig's disease. There is no cure and it always proves fatal. Primary endpoints were not met in the study of 138 participants, apart from in a subgroup and even then more research was recommended by the authors.
They theorised that chlorite from NP001 combined with a non-proteinogenic amino acid called taurine to form taurine chloramine (TauCl), which can downregulate monocytes. A result of this that the monocytes are deactivated and produce less NF-kB and inflammatory cytokines.
Unfortunately this symptomatic effect is purely down to chemically induced brute force immunosuppression, not due to antiviral effects and the last thing you would need to fight a viral infection. It could potentially turn an infection into a silent killer with unpredictable sequalae due to higher viral loads.
A few conflicts of interest statements were also provided:
Conflict of interest statement
R.G. Miller, the author reports no conflict of interest. R. Zhang, the author reports no conflict of interest. P.M. Bracci, the author reports no conflict of interest. A. Azhir, CEO of Neuvivo Inc. R. Barohn has received research grants from NIH and consulting support from NuFactor. R. Bedlack has received research support from ALSA, Healey Center, MediciNova. He has received consulting support from AB Science, ALSA, Alexion, Amylyx, Apellis, Biogen, Biohaven, Brainstorm, Clene, Corcept, Cytokinetics, GenieUS, Guidepoint, ITF Pharma, Mallinkrodt, Orphazyme, Shinkei, Woolsey Pharma. M. Benatar, the author reports no conflict of interest. J.D. Berry, the author reports no conflict of interest. M. Cudkowicz, the author reports no conflict of interest. E.J. Kasarskis, the author reports no conflict of interest. H. Mitsumoto has received research funding from NIH, ALS Association, SPF, MDA Wings, Tsumura & Co, Mitsubishi‐Tanabe Pharma. He has participated in advisory boards for Amylyx, PTC Bio (one time). G. Manousakis, the author reports no conflict of interest, D. Walk, the author reports no conflict of interest. B. Oskarsson the author, reports no conflict of interest. J. Shefner has received grant/research/clinical trial support from Amylyx, Biogen, Cytokinetics Incorporated, Mitsubishi Tanabe Pharma America, Sanofi, Novartis, Annexon, Jannsen. Alexion, Medicinova, Ionis, and Alector. He has received personal compensation from Amylyx, Apic Biosciences, Neurosense, Cytokinetics, Denal, GSK, Mitsubishi Tanabe Pharma America, RRD, Swanbio, Helixsmith, Novartis, Sanofi, and Sawei. M.S. McGrath, Founder and Chief scientific officer of Neuvivo Inc. Did not personally access the Neuvivo database for the primary analysis described in this manuscript.
The NP001 formulation of sodium chlorite acts through a plausible mechanism and preliminary data suggest that it is safe and may slow ALS progression in some PALS. The WF10 formulation of SC appears to act through this same mechanism. Although WF10 is available for off-label use, it is very expensive, may have more side-effects than NP001, and at this time has only scant anecdotal evidence for efficacy in PALS. ALSUntangled supports further carefully monitored studies of NP001 and WF10 in PALS. In contrast, oral sodium chlorite has potentially dangerous and toxic side-effects may hasten disease progression, and is not clearly absorbed from the gut. We do not recommend further use of oral sodium chlorite unless it can at least be shown to be safe and to act on mechanisms in humans that are relevant to ALS.
Returning to taurine chloramine, why is this potentially disastrous for some patients?
In a 2013 study by Dall’Igna et al male rats were divided into two groups, one a sham group as control, the other had sepsis induced by cecal ligation and perforation (CLP), and of these cultured lymphocytes were exposed to Tau and TauCl at concentrations of 0.1, 0.2, 0.3, 0.4 and 0.5 mM for 1 hour19:
Figure 7. Effect of TauCl on production of anti-inflammatory mediator IL-10 by Th2 lymphocytes. Activated lymphocytes (1 × 106 cells/ml) were preincubated with TauCl (0.1 or 0.5 mM) for 1 hour. After this, supernatants were collected and IL-10 was measured by ELISA. (A) blood; (B) spleen. Results are expressed as means ± SD. *Compared with sham control 24 hours; #compared with Clp control 24 hours; &compared with sham control 120 hours; $compared with Clp control 120 hours, all with P < 0.05 significant (n = 5). https://ccforum.biomedcentral.com/articles/10.1186/cc12975/figures/
These findings show a possible impairment in lymphocyte function promoted by TauCl, correlated with immunosuppression and cell death characteristic of the late stages of sepsis.
If immunosuppression was the desired outcome it would be much safer systemically and more effective to instead administer short term corticosteroids20 and then follow the FLCCC antiviral protocols to bring the viral infection under control.
…On the human side, several case reports described mild and severe intoxications with ClO2 and related compounds at different doses in healthy and comorbid individuals. Clinical studies revealed no conclusive evidence on ClO2 as an effective systemic treatment.
Conclusions. The principle of precaution should be called upon until quality evidence is provided; new and more comprehensive pre-clinical studies are needed before carrying out human trials. Meanwhile, tighter regulations on this substance could prevent adverse toxicological events.
A newly published paper links taurine deficiency to accelerated aging21:
Editor’s summary
Aging is associated with physiological changes that range in scale from organelles to organ systems, but we are still working to understand the molecular basis for these changes. Studying various animals, Singh et al. found that the amount of the semi-essential amino acid taurine in circulation decreased with age (see the Perspective by McGaunn and Baur). Supplementation with taurine slowed key markers of aging such as increased DNA damage, telomerase deficiency, impaired mitochondrial function, and cellular senescence. Loss of taurine in humans was associated with aging-related diseases, and concentrations of taurine and its metabolites increased in response to exercise. Taurine supplementation improved life span in mice and health span in monkeys. —L. Bryan Ray
Structured Abstract
INTRODUCTION
Aging is an inevitable multifactorial process. Aging-related changes manifest as the “hallmarks of aging,” cause organ functions to decline, and increase the risk of disease and death. Aging is associated with systemic changes in the concentrations of molecules such as metabolites. However, whether such changes are merely the consequence of aging or whether these molecules are drivers of aging remains largely unexplored. If these were blood-based drivers of aging, then restoring their concentration or functions to “youthful” levels could serve as an antiaging intervention.
RATIONALE
Taurine, a semiessential micronutrient, is one of the most abundant amino acids in humans and other eukaryotes. Earlier studies have shown that the concentration of taurine in blood correlates with health, but it is unknown whether blood taurine concentrations affect aging. To address this gap in knowledge, we measured the blood concentration of taurine during aging and investigated the effect of taurine supplementation on health span and life span in several species.
RESULTS
Blood concentration of taurine declines with age in mice, monkeys, and humans. To investigate whether this decline contributes to aging, we orally fed taurine or a control solution once daily to middle-aged wild-type female and male C57Bl/6J mice until the end of life. Taurine-fed mice of both sexes survived longer than the control mice. The median life span of taurine-treated mice increased by 10 to 12%, and life expectancy at 28 months increased by about 18 to 25%. A meaningful antiaging therapy should not only improve life span but also health span, the period of healthy living. We, therefore, investigated the health of taurine-fed middle-aged mice and found an improved functioning of bone, muscle, pancreas, brain, fat, gut, and immune system, indicating an overall increase in health span. We observed similar effects in monkeys. To check whether the observed effects of taurine transcended the species boundary, we investigated whether taurine supplementation increased life span in worms and yeast. Although taurine did not affect the replicative life span of unicellular yeast, it increased life span in multicellular worms. Investigations into the mechanism or mechanisms through which taurine supplementation improved the health span and life span revealed that taurine positively affected several hallmarks of aging. Taurine reduced cellular senescence, protected against telomerase deficiency, suppressed mitochondrial dysfunction, decreased DNA damage, and attenuated inflammation. An association analysis of metabolite clinical risk factors in humans showed that lower taurine, hypotaurine, and N-acetyltaurine concentrations were associated with adverse health, such as increased abdominal obesity, hypertension, inflammation, and prevalence of type 2 diabetes. Moreover, we found that a bout of exercise increased the concentrations of taurine metabolites in blood, which might partially underlie the antiaging effects of exercise.
CONCLUSION
Taurine abundance decreases during aging. A reversal of this decline through taurine supplementation increases health span and life span in mice and worms and health span in monkeys. This identifies taurine deficiency as a driver of aging in these species. To test whether taurine deficiency is a driver of aging in humans as well, long-term, well-controlled taurine supplementation trials that measure health span and life span as outcomes are required.
Taurine deficiency as a driver of aging. Taurine concentration in blood declines with aging (top left). A reversal of this drop through taurine supplementation increased healthy life span in mice and worms but not in yeast (bottom left and top middle). Taurine supplementation affected several hallmarks of aging (middle). In humans, lower taurine concentrations were associated with multiple diseases (top right). A randomized controlled clinical trial in humans is warranted to assess the antiaging effects of taurine (bottom right). BMI, body mass index.
And this paper from 1997 (paywalled) researched how chlorite ions combine with taurine, contributing to deficiencies22:
Abstract
The reaction between chlorite and the aminosulfonic acid, taurine, has been studied in neutral to acidic pH. The stoichiometry of the reaction was deduced as 3ClO2- + H2NCH2CH2SO3H + 3H+ → Cl(H)NCH2CH2SO3H + 2ClO2 + 2H2O. The formation of chlorotaurine is rapid and is followed by a slower accumulation of chlorine dioxide. The chlorotaurine disproportionates at low pH to give dichlorotaurine and taurine. There is no appreciable reaction between chlorine dioxide and any of the amine species in solution. The reaction is characterized by an induction period during which the reactive species HOCl and H(OH)NCH2CH2SO3H are formed. This is followed by the autocatalytic production of chlorotaurine and chlorine dioxide. The autocatalysis is mediated through the formation of the intermediate Cl2O2, which is typical of the reactions of chlorite. One notable result obtained in this study was that the C−S bond in taurine does not cleave even when subjected to a strong oxidizing agent, HOCl.
If I come across papers with potential therapeutic properties I’m happy to add them here, and anti-tumour action always gets my attention, especially as this kind of research may be buried by conflicted parties.
This was from 1982 and explored how neutrophils can chlorinate taurine to generate hypochlorous acid, “an important role in the inflammatory response and host defense.23”. Caution applies in that limiting factors are involved with the chemical reactants:
Abstract
The model hydrogen peroxide-myeloperoxidase-chloride system is capable of generating the powerful oxidant hypochlorous acid, which can be quantitated by trapping the generated species with the beta-amino acid, taurine. The resultant stable product, taurine chloramine, can be quantitated by its ability to oxidize the sulfhydryl compound, 5-thio-2-nitro-benzoic acid to the disulfide, 5,5'-dithiobis(2-nitroben-zoic acid) or to oxidize iodide to iodine. Using this system, purified myeloperoxidase in the presence of chloride and taurine converted stoichiometric quantities of hydrogen peroxide to taurine chloramine. Chloramine generation was absolutely dependent on hydrogen peroxide, myeloperoxidase, and chloride and could be inhibited by catalase, myeloperoxidase inhibitors, or chloride-free conditions. In the presence of taurine, intact human neutrophils stimulated with either phorbol myristate acetate or opsonized zymosan particles generated a stable species capable of oxidizing 5-thio-2-nitrobenzoic acid or iodide. Resting cells did not form this species. The oxidant formed by the stimulated neutrophils was identified as taurine chloramine by both ultraviolet spectrophotometry and electrophoresis. Taurine chloramine formation by the neutrophil was dependent on the taurine concentration, time, and cell number. Neutrophil-dependent chloramine generation was inhibited by catalase, the myeloperoxidase inhibitors, azide, cyanide, or aminotriazole and by chloride-free conditions, but not by superoxide dismutase or hydroxyl radical scavengers. Thus, it appears that stimulated human neutrophils can utilize the hydrogen peroxide-myeloperoxidase-chloride system to generate taurine chloramine. Based on the demonstrated ability of the myeloperoxidase system to generate free hypochlorous acid we conclude that neutrophils chlorinate taurine by producing this powerful oxidant. The biologic reactivity and cytotoxic potential of hypochlorous acid and its chloramine derivatives suggest that these oxidants play an important role in the inflammatory response and host defense.
HOC1 is a powerful oxidant capable of reacting with a host of biologically important molecules (30-32). We have previously shown that a human tumor cell line is sensitive to low concentrations of HOC1 (8) and Thomas (17) has demonstrated its strong bactericidal potential. Indeed, neutrophils are capable of incorporating chloride into insoluble fractions of phagocytosed bacteria (35). The reactivity of HOC1 also suggests potential control mechanisms for limiting its production. HOCI generation by neutrophils would be dependent on the quantity of H202 produced, the rate of H202 catabolism by endogenous catalase or the glutathione redox system, the amount of myeloperoxidase released, and the availability of potential substrates for HOCI. If sufficient myeloperoxidase is released but there are no available substrates for HOCI, either myeloperoxidase (6, 10) or possibly NADPH oxidase itself (36) could be rapidly inactivated.
Analysis of the oxidant distribution in the supernatant and cell button revealed that the majority of the chloramine was in the extracellular milieu, but we cannot be certain that this necessarily reflects extracellular chloramine generation. Either the chloride peroxidation products or the chloramine itself might be generated within the vacuole and then diffuse out of the cell. At present, the amounts of taurine available within the vacuolar space to scavenge the oxidant are unknown. Alternatively, neutrophils do release H202 and myeloperoxidase extracellularly (1, 4), and we might be detecting only those chloramines generated outside the cell. In other studies, myeloperoxidase-mediated iodination products generated by neutrophils are also preferentially localized in the extracellular rather than the intracellular environment (1, 16).
Reference (8):
Slivka A, LoBuglio AF, Weiss SJ. A potential role for hypochlorous acid in granulocyte-mediated tumor cell cytotoxicity. Blood. 1980;55(2):347-350.
To conclude, from 2010 Gottardi and Nadl described the properties of N-chlorotaurine, and how it can be used as a “natural antiseptic with outstanding tolerability”24.
It is important to note that this does not imply or preclude antibacterial or anti-tumour properties to CDS, this is not being ingested here and the previously cited pathologies still apply, especially where sodium chlorite solution is used:
Abstract
N-chlorotaurine, the N-chloro derivative of the amino acid taurine, is a long-lived oxidant produced by activated human granulocytes and monocytes. Supported by a high number of in vitro studies, it has mainly anti-inflammatory properties and seems to be involved in the termination of inflammation. The successful synthesis of the crystalline sodium salt (Cl-HN-CH(2)-CH(2)-SO(3)Na, NCT) facilitated its development as an endogenous antiseptic. NCT can be stored long-term at low temperatures, and it has killing activity against bacteria, fungi, viruses and parasites. Transfer of the active chlorine to amino groups of molecules of both the pathogens and the human body (transhalogenation) enhances rather than decreases its activity, mainly because of the formation of monochloramine. Furthermore, surface chlorination after sublethal incubation times in NCT leads to a post-antibiotic effect and loss of virulence of pathogens, as demonstrated for bacteria and yeasts. Being a mild oxidant, NCT proved to be very well tolerated by human tissue in Phase I and II clinical studies. A 1% aqueous solution can be applied to the eye, skin ulcerations, outer ear canal, nasal and paranasal sinuses, oral cavity and urinary bladder, and can probably be used for inhalation. Therapeutic efficacy in Phase II studies has been shown in external otitis, purulently coated crural ulcerations and keratoconjunctivitis, so far. Based upon all presently available data, NCT seems to be an antiseptic with a very good relation between tolerability and activity. Recently, C-methylated derivatives of NCT have been invented, which are of interest because of improved stability at room temperature.
Thank you for reading DoorlessCarp’s Scientific Literature Reviews. This post is public so feel free to share it.
Hatanaka, N., et al. "Chlorine Dioxide Is a More Potent Antiviral Agent against Sars-Cov-2 Than Sodium Hypochlorite." J Hosp Infect 118 (2021): 20-26. Print.
Cao, J., et al. "Can Nasal Irrigation with Chlorine Dioxide Be Considered as a Potential Alternative Therapy for Respiratory Infectious Diseases? The Example of Covid-19." Biosci Trends 16.6 (2022): 447-50. Print.
Burela, A., et al. "Chlorine Dioxide and Chlorine Derivatives for the Prevention or Treatment of Covid-19: A Systematic Review." Rev Peru Med Exp Salud Publica 37.4 (2020): 605-10. Print.
Farfán-Castillo, A. L. M., et al. "Use of Ivermectin and Chlorine Dioxide for Covid-19 Treatment and Prophylaxis in Peru: A Narrative Review." Cureus 14.11 (2022): e31836. Print.
Bercz, J. P., et al. "Subchronic Toxicity of Chlorine Dioxide and Related Compounds in Drinking Water in the Nonhuman Primate." Environ Health Perspect 46 (1982): 47-55. Print.
“TOXICOLOGICAL REVIEW OF CHLORINE DIOXIDE AND CHLORITE”. (CAS Nos. 10049-04-4 and 7758-19-2) In Support of Summary Information on the Integrated Risk Information System (IRIS) September 2000 U.S. Environmental Protection Agency Washington, DC.
Moser, M. “Out of Control? Managing Baseline Variability in Experimental Studies with Control Groups”. Good Research Practice in Non-Clinical Pharmacology and Biomedicine, 2020, Volume 257. ISBN : 978-3-030-33655-4.
Arellano-Gutiérrez, G., E. H. Aldana-Zaragoza, and A. Pérez-Fabián. "Intestinal Perforation Associated with Chlorine Dioxide Ingestion: An Adult Chronic Consumer During Covid-19 Pandemic." Clin J Gastroenterol 14.6 (2021): 1655-60. Print.
Medina-Avitia, E., P. Tella-Vega, and C. García-Estrada. "Acute Kidney Injury Secondary to Chlorine Dioxide Use for Covid-19 Prevention." Hemodial Int 25.4 (2021): E40-e43. Print.
Andres AS, Luis Del CO, Karen O´Nelly GE, Francisco SPP and Angela BJ, et al. (2020). “Chemical pneumonitis secondary to chlorine dioxide consumption in a patient with severe Covid 19”. Clin Case Rep Rev, 6: DOI: 10.15761/CCRR.1000488.
Miller, R. G., et al. "Phase 2b Randomized Controlled Trial of Np001 in Amyotrophic Lateral Sclerosis: Pre-Specified and Post Hoc Analyses." Muscle Nerve 66.1 (2022): 39-49. Print.
Dall'Igna, Dhébora Mozena, et al. "Taurine Chloramine Decreases Cell Viability and Cytokine Production in Blood and Spleen Lymphocytes from Septic Rats Submitted to Sepsis." Critical Care 17.4 (2013): P76. Print.
Chinake* CR, Reuben H. Simoyi* †. Oxyhalogen−Sulfur Chemistry: Oxidation of Taurine by Chlorite in Acidic Medium1. ACS Publications. doi:10.1021/jp963067a
1. Weiss SJ, Klein R, Slivka A, Wei M. Chlorination of taurine by human neutrophils. Evidence for hypochlorous acid generation. J Clin Invest. 1982;70(3):598-607. doi:10.1172/jci110652










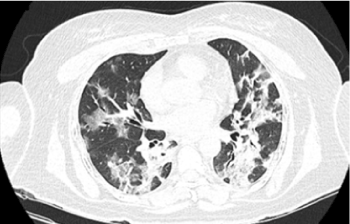
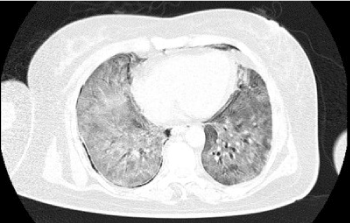

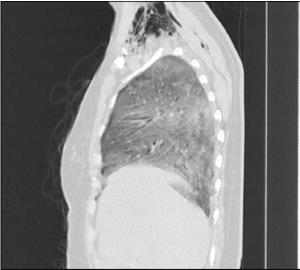

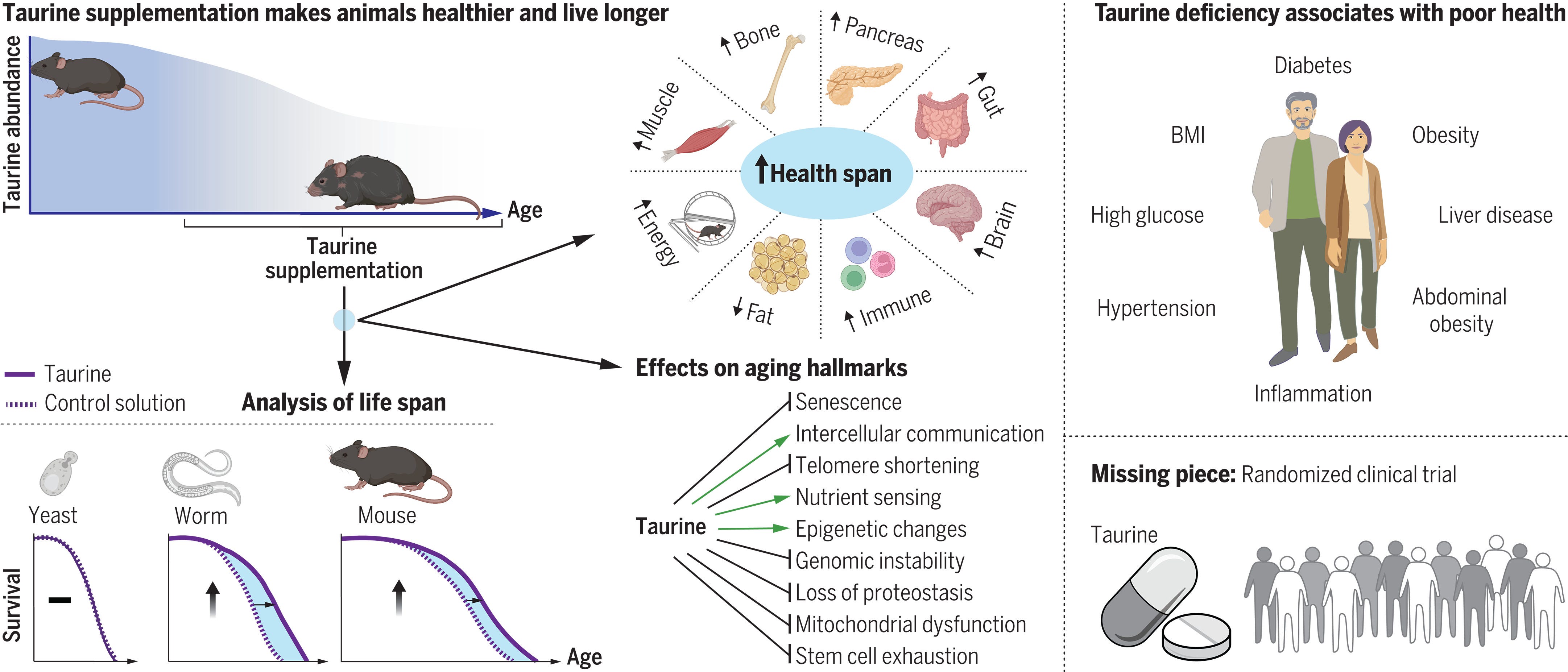

interesting video from dr campbell ... thought it might be of interest
https://www.youtube.com/watch?v=kEE5OfiVS7o
Thanks DC. Tragic that the most needy folk misunderstood the surface disinfectant & the dilute solution for nasal rinsing & throat gargling only.