Any extracts used in the following article are for non-commercial research and educational purposes only and may be subject to copyright from their respective owners.
The main role of the Cellular, Tissue, and Gene Therapies Advisory Committee(CTGTAC) is to provide advice and recommendations to the FDA on regulatory issues.
An important meeting took place in September 2021 and it was open to the public. Under discussion were the toxicity AND oncological risks of adeno-associated virus (AAV) vector-based gene therapy (GT) products.1
mRNA COVID-19 “vaccines” were not under discussion, even though they clearly meet the FDA’s definition of gene therapy products.
Two criteria clearly satisfied include the introduction of a new gene to express an unnatural protein using LNP’s and introduction of plasmid DNA (albeit due to contamination or by design):2
From: “Gene therapy products are biological products regulated by the FDA’s Center for Biologics Evaluation and Research (CBER). Clinical studies in humans require the submission of an investigational new drug application (IND) prior to initiating clinical studies in the United States. Marketing a gene therapy product requires submission and approval of a biologics license application (BLA).” Source: https://www.fda.gov/vaccines-blood-biologics/cellular-gene-therapy-products/what-gene-therapy
GT products cited in the key notes included Zolgensma and Luxturna.
This is what the manufacturers say about them:
ZOLGENSMA® (onasemnogene abeparvovec-xioi) is an essential one-time treatment option that targets the genetic root cause of spinal muscular atrophy (SMA) by replacing the function of the missing or nonworking SMN1 gene—stopping progression of SMA.
ZOLGENSMA is a prescription gene therapy for the treatment of SMA in children less than 2 years old.
Go to their webpage and you are met with over a page of “Important Safety Information” that you cannot miss, and part of which includes the risk of acute liver failure and death. Not good, but at least everyone knows the risks and most importantly can give informed consent.
LUXTURNA (voretigene neparvovec-rzyl) is a prescription gene therapy product used for the treatment of patients with inherited retinal disease due to mutations in both copies of the RPE65 gene, which can only be confirmed through genetic testing.
Again, you cannot miss the “Important Safety Information for LUXTURNA”. This time death isn’t stated as an inconvenient side effect, but it could make you go blind…
Of interest to this Substack are the CTGTAC notes on oncogenicity risks (ie the capability of inducing tumor formation) due to vector integration.
This is particularly relevant due to multiple labs and independent researchers confirming illegally high levels of contamination of LNP/mRNA gene therapy COVID-19 agents with both DNA fragments and Simian Virus 40 (SV40) promoter-enhancer-ori.
So what are promoter-enhancers?
“Enhancers and promoters are gene-regulatory elements. They are stretches of DNA that help in both eukaryotic and prokaryotic transcription. The promoters are known to initiate transcription, and the enhancers increase the level of transcription.”3
From: “Figure 2. Pfizer bivalent vaccine assembly of the RNA-seq library. Annotated with SEB/FCS, spike insert (red), bacterial origin of replication (yellow), Neo/Kan resistance gene (green), F1 origin (yellow) and an SV40 promoter (yellow and white).” Source: https://osf.io/preprints/osf/b9t7m
As you will see from the keynotes later, although the nuclear translocation vector is different (endocytosed LNPs adulterated with plasmid DNA vs using non-replicating genetically modified adenoviruses) there are significant parallels.
However, if you search for an equivalent meeting by the CTGTAC to discuss the oncogenicity risk of contaminated LNP/mRNA COVID-19 gene therapies you will not find any such meeting, even with recent findings, and none are scheduled.
Expression vector dsDNA and DNA fragment contamination of mRNA COVID-19 gene therapy agents
Abstracts of papers by McKernan et al. for context (emphasis mine).
The first of two game changing papers by Dr Kev and his colleagues. Most importantly I understand it was an accidental discovery that led to their further research.
From “Sequencing of bivalent Moderna and Pfizer mRNA vaccines reveals nanogram to microgram quantities of expression vector dsDNA per dose“4 (April 2023).
Abstract
Several methods were deployed to assess the nucleic acid composition of four vials of the Moderna and Pfizer bivalent mRNA vaccines. Two vials from each vendor were evaluated with Illumina sequencing, qPCR, RT-qPCR, Qubit™ 3 fluorometry and Agilent Tape Station™ electrophoresis. Multiple assays support DNA contamination that exceeds the European Medicines Agency (EMA) 330ng/mg requirement and the FDAs 10ng/dose requirements. These data may impact the surveillance of vaccine mRNA in breast milk or plasma as RT-qPCR assays targeting the vaccine mRNA cannot discern DNA from RNA without RNase or DNase nuclease treatments. Likewise, studies evaluating the reverse transcriptase activity of LINE-1 and vaccine mRNA will need to account for the high levels of DNA contamination in the vaccines. The exact ratio of linear fragmented DNA versus intact circular plasmid DNA is still being investigated. Quantitative PCR assays used to track the DNA contamination are described.
From the second paper “DNA fragments detected in monovalent and bivalent Pfizer/BioNTech and Moderna modRNA COVID-19 vaccines from Ontario, Canada: Exploratory dose response relationship with serious adverse events.“5 (October 2023).
Note that with Pfizer a different manufacturing process was used for mass production than the one the regulators approved. Its the classic bait-and-switcheroo. The box you took home turned out to be full of rocks, not fine china. The difference is that the paid off regulators just let this one go instead of going back to the seller with your 6’ tall cousin called Bob who doesn’t take any sh##:
Abstract
Background: In vitro transcription (IVT) reactions used to generate nucleoside modified RNA (modRNA) for SARS-CoV-2 vaccines currently rely on an RNA polymerase transcribing from a DNA template. Production of modRNA used in the original Pfizer randomized clinical trial (RCT) utilized aPCR-generated DNA template (Process 1). To generate billions of vaccine doses, this DNA was cloned into a bacterial plasmid vector for amplification in Escherichia coli before linearization (Process 2), expanding the size and complexity of potential residual DNA and introducing sequences not present in the Process 1 template. It appears that Moderna used a similar plasmid-based process for both clinical trial and post-trial use vaccines. Recently, DNA sequencing studies have revealed this plasmid DNA at significant levels in both Pfizer-BioNTech and Moderna modRNA vaccines. These studies surveyed a limited number of lots and questions remain regarding the variance in residual DNA observed internationally.
Methods: Using previously published primer and probe sequences, quantitative polymerase chain reaction (qPCR) and Qubit® fluorometry was performed on an additional 27 mRNA vials obtained in Canada and drawn from 12 unique lots (5 lots of Moderna child/adult monovalent, 1 lot of Moderna adult bivalent BA.4/5, 1 lot of Moderna child/adult bivalent BA.1, 1 lot of Moderna XBB.1.5 monovalent, 3 lots of Pfizer adult monovalent, and 1 lot of Pfizer adult bivalent BA.4/5). The Vaccine Adverse Events Reporting System (VAERS) database was queried for the number and categorization of adverse events (AEs) reported for each of the lots tested. The content of one previously studied vial of Pfizer COVID-19 vaccine was examined by Oxford Nanopore sequencing to determine the size distribution of DNA fragments. This sample was also used to determine if the residual DNA is packaged in the lipid nanoparticles (LNPs) and thus resistant to DNaseI or if the DNA resides outside of the LNP and is DNaseI labile.
Results: Quantification cycle (Cq) values (1:10 dilution) for the plasmid origin of replication (ori) and spike sequences ranged from 18.44 - 24.87 and 18.03 - 23.83 and for Pfizer, and 22.52 – 24.53 and 25.24 – 30.10 for Moderna, respectively. These values correspond to 0.28 – 4.27 ng/dose and 0.22 - 2.43 ng/dose (Pfizer), and 0.01 -0.34 ng/dose and 0.25 – 0.78 ng/dose (Moderna), for ori and spike respectively measured by qPCR, and 1,896 – 3,720 ng/dose and 3,270 – 5,100 ng/dose measured by Qubit® fluorometry for Pfizer and Moderna, respectfully. The SV40 promoter-enhancer-ori was only detected in Pfizer vials with Cq scores ranging from 16.64 – 22.59. In an exploratory analysis, we found preliminary evidence of a dose response relationship of the amount of DNA per dose and the frequency of serious adverse events (SAEs). This relationship was different for the Pfizer and Moderna products. Size distribution analysis found mean and maximum DNA fragment lengths of 214 base pairs (bp) and 3.5 kb, respectively. The plasmid DNA is likely inside the LNPs and is protected from nucleases.
Conclusion:These data demonstrate the presence of billions to hundreds of billions of DNA molecules per dose in these vaccines. Using fluorometry, all vaccines exceed the guidelines for residual DNA set by FDA and WHO of 10 ng/dose by 188 – 509-fold. However, qPCR residual DNA content in all vaccines were below these guidelines emphasizing the importance of methodological clarity and consistency when interpreting quantitative guidelines. The preliminary evidence of a dose-response effect of residual DNA measured with qPCR and SAEs warrant confirmation and further investigation. Our findings extend existing concerns about vaccine safety and call into question the relevance of guidelines conceived before the introduction of efficient transfection using LNPs. With several obvious limitations, we urge that our work is replicated under forensic conditions and that guidelines be revised to account for highly efficient DNA transfection and cumulative dosing.
Health Canada confirm the findings
In October ‘23 Health Canada confirmed the presence of SV40 promoter DNA sequence in Pfizer’s BNT162b2 COVID-19 “vaccine” to the Epoch Times.6
They quickly attempted to back-track and the “fact checkers” (narrative checkers) were all over it. Both raised more questions than they answered or tried to use straw man rebuttals, such as saying that full length SV40 virus was not found, even though no-one ever stated that it was…
Health Canada later said that concerns about the SV40 promoter-enhancer sequence being linked to increased cancer risk are “unfounded,” adding there was no evidence to support such a claim. “The fragment is inactive, has no functional role, and was measured to be consistently below the limit required by Health Canada and other international regulators,” the agency told The Epoch Times.
But when asked by this publication in November to provide its risk assessment to support such a statement—as well as examples of studies performed to assess the risk of cancer in vaccines and the SV40 sequence—Health Canada declined.
Health Canada also did not respond to questions about what evidence it has that the SV40 fragment is inactive, whether the SV40 has no “functional role” in the plasmid or if transfected into humans, why it is present if it has no role, and what the specific limit is for the SV40 promoter-enhancer and what measurements were obtained and techniques used to acquire them.
“In the case of the Pfizer-BioNTech COVID-19 vaccine, the full DNA sequence of the Pfizer plasmid was provided at the time of initial filing, though it did not specifically identify the SV40 promoter enhancer sequence. The SV40 promoter enhancer sequence was found to be a residual DNA fragment in Pfizer-BioNTech COVID-19 vaccine,” Health Canada said in response to the questions.
…Health Canada did not answer most of the questions, responding that Pfizer’s submission provided “information that process 1 was used for clinical trials and process 2 was used for commercial scale-ups.”
…When The Epoch Times asked Health Canada to comment on the ORF present in the plasmid, why it was present, and if it had been identified by Pfizer-BioNTech, the agency did not provide an answer.
Health Canada said it would not provide further information when asked to give specific and detailed responses to questions.
Pfizer has not responded to multiple previous inquiries.
From “SV40 DNA in Pfizer-BioNTech Shot: Health Canada Leaves Many Unanswered Questions” (December 22, 2023)
Doing the usual fact-free angry arm waving, “AFP Fact Check” first attacked Epoch Times as a disinformation spreader, state that the “narrative that Covid-19 vaccines contain harmful DNA particles that could alter recipients' genetics” is “debunked” (a word they like to use) and include lots of quotes from “experts”.
What you won’t find is clinical trials data or an objective balance of links to relevant research papers.
What you will find is comedic in irony. Admitting to cancer risks from other mass administered vaccines is perhaps not the best fact check you could use:
Messenger ribonucleic acid (mRNA) Covid-19 vaccines are developed using plasmid -- a small, circular piece of DNA, according to a fact sheet (archived here) from the US National Human Genome Research Institute (NHGRI). One such piece of DNA comes from SV40, a pathogen in monkeys used to prepare polio vaccines in the 1950s (archived here and here).
While the virus itself is associated with cancer, there is no conclusive evidence that tumors in humans were caused by the polio shots -- and the pathogen itself has not been present in any vaccines since 1963, according to Children's Hospital of Philadelphia (archived here).
From “Posts misrepresent Health Canada statement on DNA in Covid vaccines“ (2023)
Unfortunately its “turtles all the way down” with their narrative control. To deny there being any “conclusive evidence” of SV40 induced cancer cases at all in nearly 100 million vaccinated children amounts to saying that SV40 does not cause cancer in humans.
“Immunization Safety Review: SV40 Contamination of Polio Vaccine and Cancer”7 (2003) gives some useful facts (emphasis mine).
IPV: Inactivated polio vaccine.
OPV: Live attenuated polio vaccine.
SV40 is a polyomavirus that commonly infects certain species of Asian macaques, especially the rhesus monkey. Other polyomaviruses, which are generally species-specific, include the BK and JC viruses of humans. Polyomaviruses are a genus of the papovavirus family of DNA viruses. This family also includes the papillomaviruses, of which one—human papillomavirus (HPV)—is causally associated with cervical cancer.
In fact, the presence of SV40 in polio vaccine produced from macaque kidney cell cultures was originally identified because of the cytopathological effects of the contaminated vaccine in African green monkey kidney cell cultures (Sweet and Hilleman, 1960). As another example, the JC virus is known to cause progressive multifocal leukoencephalopathy in immunocompromised humans.
With continuing controversy about the role of SV40 in human cancers (Brown and Lewis, 1998; Klein et al., 2002), the Interagency Vaccine Group asked the Immunization Safety Review Committee to address the question of whether exposure to the SV40-contaminated polio vaccine causes cancer in humans.
The very abundance of new and emerging literature on the oncogenic potential of SV40 and its association with certain cancers suggests that it is not too late to try to resolve the question of whether SV40 contamination of polio vaccines could cause cancers in humans. Four forms of human cancer— mesothelioma, osteosarcoma, ependymoma, and non-Hodgkin's lymphoma (NHL)—have been linked to SV40 in animal studies.
IPV administered between 1955 and 1963 to about 98 million children and adults is assumed to be the primary source of human exposure to SV40 in the United States.4 In addition, experimental lots of OPV contaminated with SV40 was administered to about 10,000 people participating in clinical trials between 1959 and 1961.
Recipients of the oral vaccine, in contrast to those receiving contaminated IPV, did not develop an antibody response to SV40 (as reviewed in Shah and Nathanson, 1976). This suggests that IPV, not OPV, resulted in the infection of humans with SV40. Nonetheless, concerns about the validity, and in particular the specificity for SV40, of the serologic testing create some uncertainty about this conclusion.
Your findings depend on where you look:
Details of the level and extent of the contamination of IPV are unavailable. Because the process used to inactivate the poliovirus was less effective against SV40, IPV could have included killed or live SV40. Furthermore, manufacturers used different types of cell cultures, and some were less vulnerable to contamination (Shah and Nathanson, 1976).
Tests of stored samples of the vaccine that had been administered in the United States from May through July in 1955 found various levels of SV40 contamination, with some vaccine showing no contamination (Fraumeni et al., 1963). From these data, Shah and Nathanson (1976) estimated that 10% to 30% of IPV contained live SV40 and that similar percentages of the approximately 98 million Americans who had been vaccinated by 1961 were exposed to live SV40.
From “Cancer risk associated with simian virus 40 contaminated polio vaccine“8 (1999) by Fisher et al. (emphasis mine):
…Recently, investigators have provided persuasive evidence that SV40 is present in human ependymomas, choroid plexus tumors, bone tumors, and mesotheliomas, however, the etiologic role of the virus in tumorigenesis has not been established.
Materials and methods: Using data from SEER, we analyzed the incidence of brain tumors, bone tumors, and mesotheliomas from 1973-1993 and the possible relationship of these tumors with the administration of the SV40 contaminated vaccine.
Results: Our analysis indicates increased rates of ependymomas (37%), osteogenic sarcomas (26%), other bone tumors (34%) and mesothelioma (90%) among those in the exposed as compared to the unexposed birth cohort.
Conclusions: These data suggest that there may be an increased incidence of certain cancers among the 98 million persons exposed to contaminated polio vaccine in the U.S.; further investigations are clearly justified.
I always associated mesothelioma with asbestos exposure, not polio vaccination. The latency period due to asbestos commonly ranges from 10 - 50 years, 70 at the extreme.9 Its not one of the turbocancers and those responsible are probably retired long before cases spike and victims have no chance at getting justice.
Moving on to blood cancers and NHL. From “Association between SV40 and non-Hodgkin's lymphoma“10 (2003) by Butel et al. (emphasis mine):
Millions of people worldwide were inadvertently exposed to live simian virus 40 (SV40) between 1955 and 1963 through immunization with SV40-contaminated polio vaccines. Although the prevalence of SV40 infections in humans is not known, numerous studies suggest that SV40 is a pathogen resident in the human population today.
“Potent” is not a word the narrative checkers would like you to associate with contaminated vaccines.
Nb. Secondary brain cancers are fairly common with stage IV breast cancer, especially with HER2-positive or triple-negative BC.11 We will return to HER2 later.
SV40 is a potent DNA tumor virus that is known to induce primary brain cancers, bone cancers, mesotheliomas, and lymphomas in laboratory animals. SV40 oncogenesis is mediated by the viral large tumor antigen (T-ag), which inactivates the tumor suppressor proteins p53 and pRb.
During the last decade, independent studies using different molecular biology techniques have shown the presence of SV40 DNA, T-ag, or other viral markers in primary human brain and bone cancers and malignant mesotheliomas.
In our study, we analyzed systemic NHL from 76 HIV-1-positive and 78 HIV-1-negative patients, and nonmalignant lymphoid samples from 79 HIV-1-positive and 107 HIV-1-negative patients without tumors; 54 colon and breast carcinoma samples served as cancer controls.
SV40-specific DNA sequences were detected in 64 (42%) of 154 NHL, none of 186 nonmalignant lymphoid samples, and none of 54 control cancers.For NHL from HIV-1-positive patients, 33% contained SV40 DNA and 39% Epstein Barr virus (EBV) DNA, whereas NHLs from HIV-1-negative patients were 50% positive for SV40 and 15% positive for EBV. Few tumors were positive for both SV40 and EBV. Human herpesvirus type 8 was not detected.
This is awkward:
SV40 sequences were found most frequently in diffuse large B cell and follicular-type lymphomas. We conclude that SV40 is significantly associated with some types of NHL and that lymphomas should be added to the types of human cancers associated with SV40.
Martini et al. go into more detail about SV40 induced oncogenicity.
Nb. There is no evidence that COVID-19 gene therapy agents express the oncoprotein large T antigen (T-ag), but the SV40 promoter itself and DNA integration is enough to potentially either activate oncogenes or suppress tumour suppressor expressing genes.
The lack of T-ag (or TAG) is actually not necessarily a good thing, as it turns out.1213
By analogy with viruses that integrate into the host genome, a second mechanism for DNA-induced oncogenesis has been proposed, viz., through the integration of DNA. There are several ways that the integration of DNA could have oncogenic consequences. If DNA integrated next to a dominant proto-oncogene such as c-myc and increased its expression level or activated its expression inappropriately, then this could result in the oncogenic conversion of a normal cell to one with a neoplastic phenotype. If DNA integration occurred in a tumor-suppressor gene, such as the p53 gene or the RB gene, resulting in the functional inactivation of that gene, then this cell might, over time, become neoplastic through loss of heterozygosity by acquiring additional inactivating mutations in the other allele.
From: “Issues associated with residual cell-substrate DNA in viral vaccines“ (2009)
In any case none of this is particularly relevant to safety discussions as Spike protein itself is also an oncoprotein.
Nuclear translocation of Spike mRNA due to the novelnuclear localization signal (NLS) "PRRARSV," also leads downstream not just to impeded tumour suppressor p53, but of BRCA-1 too.14
Although later retracted no-one has been able to dispute this.
In fact, later studies confirmed the findings.
From: “Figure 3. Severe acute respiratory syndrome coronavirus 2 (SARS–CoV–2) spike protein impedes the recruitment of DNA damage repair checkpoint proteins. (A) Membrane fraction (MF), cytosolic fraction (CF), soluble nuclear fraction (SNF), and chromatin-bound fraction (CBF) from HEK293T cells transfected with SARS–CoV–2 spike protein were immunoblotted for His-tag spike and indicated proteins. (B) Left: Immunoblots of DNA damage marker γH2AX in empty vector (E.V)– and spike protein–expressing HEK293T cells after 10 Gy γ-irradiation. Right: corresponding quantification of immunoblots in left. The values represent the mean ± SD (n = 3). Statistical significance was determined using Student’s t-test. **** p < 0.0001. (C) Immunoblots of DNA damage repair related proteins in spike protein–expressing HEK293T cells.(D) Representative images of 53BP1 foci formation in E.V– and spike protein-expressing HEK293 cells exposed to 10 Gy γ–irradiation. Scale bar: 10 µm. (E) Quantitative analysis of 53BP1 foci per nucleus. The values represent the mean ± SEM, n = 50. (F) BRCA1 foci formation in empty vector- and spike protein-expressing HEK293 cells exposed to 10 Gy γ–irradiation. Scale bar: 10 µm. (G). Quantitative analysis of BRCA1 foci per nucleus. The values represent the mean ± SEM, n = 50. Statistical significance was determined using Student’s t-test. **** p < 0.0001.” Source:https://www.mdpi.com/1999-4915/13/10/2056
Thus the relevance of posting these studies as the outcomes are likely to be similar - p53 associated cancers and others, helped along by galectin-3 mimicry, class switching to igG4 and inhibition of DNA damage repair (DDR) via multiple mechanisms:
There are some differences in that Spike itself is not a live, replicating virus but persistent expression for at least 6 months and in some cases 3 years renders this a mute point. Either way its long enough for neoplasm seeding in the susceptible.
From “Simian virus 40 in humans“15 (2007), (emphasis mine):
Simian virus 40 (SV40) is a monkey virus which was accidentally administered to humans, in the years 1955-'63, through contaminated poliovirus vaccines. The subsequent findings of the transforming and oncogenity activities of the SV40 viral large T (Tag) and small t (tag) antigens, have prompted investigations into the potential of SV40 to induce cancer in humans.
More recently, SV40 has been considered a Polyomavirus, together with the human BK (BKV) and JC (JCV) Polyomaviruses.
SV40 is phylogenetically closely related to the human JCV and BKV. They evidence similarity with respect to size (~5.2 Kb), genome organization and DNA sequence. The Tags of SV40, BKV and JCV strongly cross-react with the same antisera [6, 7].
The greatest homology is found in the early region coding for the Tags and tags, whereas a lower homology is detected in the regulatory region.
Tag is a nuclear phosphoprotein of 94 kD and it is an essential factor for viral DNA replication. It binds to the viral origin of replication (ori) where it promotes unwinding of the double helix and recruitment of cellular proteins that are required for DNA synthesis, including DNA polymerase-α and replication protein A [15–18].
SV40 relies on cellular enzymes and cofactors for DNA replication and these proteins are expressed in S phase. Tag modulates cellular signaling pathways to induce cells to enter S phase and this accounts for the ability of Tag to transform cells.
Large Tagis thought to stimulate the cell cycle through its ability to bind to several cellular proteins that are involved in crucial signal transduction pathways that controlcell cycle progression and apoptosis [19].
The “fact checkers” themselves have posted “debunked” disinformation.
Are they going to retract their articles?
Transformation of rodent and human cells by SV40 is induced by the two oncoproteins, the large Tag and the small tag, which display multiple functions. The main activity of Tag for cell transformation and tumorigenesis is to target key cellular proteins, such as the tumor suppressor p53 and pRB family proteins, inactivating their functions [13, 19, 33–40].
SV40 Tag may also lead to transformation by inducing mutations to the cellular genome [41] or numerical and structural alterations of chromosomes [42, 43], such as gaps, breaks, dicentric and ring chromosomes, chromatid exchanges, deletions, duplications and translocations [44].
Natural infection with SV40 is a rare event associated with monkeys. A bit like other viruses such as HIV, RSV, monkeypox…
SV40 natural infection in humans is considered a rare event, restricted to people living in contact with monkeys, the natural hosts of the virus, such as inhabitants of Indian villages located close to the jungle, and workers attending to monkeys in zoos and animal facilities [61, 62].
A source of human exposure to SV40 occurred between 1955 and 1963, when inactivated and live anti-polio vaccines, prepared from polioviruses grown in naturally SV40-infected simian cell cultures, were administered to hundreds of millions of people in the United States, Canada, Europe, Asia and Africa [63].
Soon it was shown that children vaccinated with contaminated oral polio vaccines (OPV) shed infectious SV40 in stools for at least 5 weeks after vaccination [64].
Remember the homology with human polyoma viruses?
Shah et al., [72] detected antibodies to SV40 in children born after 1964, when IPV was free of SV40, as well as in people born before 1954. These studies suggest that humans may become infected by SV40 independently from poliovirus vaccine exposure.
They didn’t have advanced PCR back then:
However, most of these early serologic studies were carried out before the discovery of the two human polyomaviruses, BK and JC, which are close related to SV40 and are ubiquitous in human populations. It is possible that the early serologic evidence of SV40 antibody detection in human sera represents some degree of cross reactivity with antibodies against the highly related BK and JC viruses [73–75].
In rodents, the injection of SV40 has been associated primarily with four types of cancer: mesothelioma, osteosarcoma, ependymoma, and lymphomas.Investigators have also detected SV40 DNA in human forms of these cancers. All but NHL are very rare…
Causality Argument
All of the studies that the committee reviewed concerning cancer incidence or cancer mortality and exposure to polio vaccine containing SV40 have substantial limitations. Many of these studies were ecologic in design. In previous reports, the committee included only controlled observational studies in tables summarizing the evidence. Ecologic studies were excluded based on their inherent limitations in assessing causality. In general, it is difficult to make causal inferences from ecologic studies, mainly because: 1) exposure and outcome data are based on measurements averaged over a population, 2) exposure information is based on proxy measures (e.g., SV40 exposure based on birth cohort), and 3) data to control for confounding are unavailable (Morgenstern, 1998).
Most of the epidemiologic studies on polio vaccine containing SV40 and cancer are subject to misclassification bias because they rely on year of birth to designate exposure status. Even though polio vaccine known to contain SV40 was in use from 1955 to 1963, it is difficult to accurately determine which individuals received the vaccine without individual vaccination records. The studies may also be subject to misclassification bias because of lack of detailed and specific information about the presence of SV40 in individual vaccine doses.
If we take the hypothesis that any tissue that can sustain SV40 is more likely to promote p53 associated tumours then it must be associated with many more cancers than those listed. You “only” need to biopsy enough patients to look for associations.
Its not in Pharma’s interest to sponsor such research though, but it has been confirmed in breast cancer too.
From “Evidence for a role of the Simian Virus 40 in human breast carcinomas”16 (2009) by Hachana et al. (emphasis mine):
Aims of the study: The aim of this study was to investigate whether the Simian Virus 40 (SV40) is implicated in human breast carcinomas (BC).
Experimental design: SV40 presence was investigated by PCR assays targeting the Tag, the regulatory, and the VP1 regions in 109 invasive breast ductal carcinomas from Tunisian women. We also examined the relationship between the presence of SV40 and promoter methylation status of 15 tumor-related genes. Immunohistochemistry was used to investigate the expression of Tag, estrogen and progesterone receptors, HER2, and P53.
Results: SV40 DNA sequences were detected in 22% of tumors and in only 1.8% of the matched non-tumoral tissues.Using immunohistochemistry, SV40 was detected in the tumor cells.
Hypermethylation causes gene silencing and is a recognised component in cancer development. Theseall have tumour suppressor properties:
Hypermethylation frequencies were 78% for RASSF1A, 66% for SHP1, 61% for HIN1 and BRCA1, 47% for P16 and ER, 42% for CDH1 and APC, 40% for BLU, 35% for DAPK, 34% for RARbeta2, 27% for GSTP1, 17% for TIMP3, 14% for CCND2, and 8% for hMLH1.
SV40 and human epidermal growth factor receptor 2 (HER2-low)
HER2-low is frequently associated with tumours17 and TAG from SV40 paradoxically acts as tumour suppressor of HER2 associated carcinomas.
Interestingly, the frequencies of RASSF1A, SHP1, BRCA1, and TIMP3 methylation, and the mean of the methylation index (MI) were significantly higher in SV40-positive than in SV40-negative cases (P-values ranging from 0.043 to 0.003). Moreover, SV40 presence correlates with P53 protein accumulation (32.7% vs. 13.3%; P=0.015) and HER2 low expression (3.7% vs. 28%; P=0.008).We also found SV40 more frequently in patients over 50 years than in younger patients (34.8% vs. 12.3%; P=0.006).
Conclusions: This study is the first to demonstrate the presence of SV40 in human BC and provides data supporting a role for this virus in the pathogenesis of these tumors.
Several observations point towards a possible similar link between SV40 and human BC. In transgenic mouse models of BC, such the C3(1)/SV40 Tag mouse model, the SV40 Tag is expressed under the regulatory control of the rat prostatic steroid binding protein C3(1) promoter.
This promoter targets expression in both the prostate in male mice and mammary gland in female mice. The inactivation of P53 and Rb by SV40 Tag in this model results in spontaneous development of mammary carcinomas, resembling human breast cancers, in 100% of female mice carrying the transgene [20]. In cell culture models, the introduction of three genes encoding for: the SV40 Tag, the telomerase catalytic subunit, and the H-RAS oncoprotein into primary human mammary epithelial cells induces a full oncogenic transformation [21].
From: “Fig 4. “Representative examples of immunohistochemical staining for the detection of the SV40 T and t antigens using the Pab108 antibody in breast carcinomas. Panels a–d represent positive cases. Panels e and f represent a negative case. Panels g and h represent positive control (transgenic adenocarcinoma of mouse prostate). Scale bar: 100 μm”, source: https://link.springer.com/article/10.1007/s10549-008-9901-z
Note the BRCA1 tumour suppressor hypermethylation too. From: “Fig. 7. Histogram of frequencies of aberrant promoter hypermethylation of RASSF1A, SHP1, HIN1, BRCA1, P16, ER, CDH1, APC, BLU, DAPK, RARβ2, GSTP1, TIMP3, CCND2, and hMLH1 genes in a series of 109 breast carcinomas from Tunisia analyzed by methylation-specific PCR”, source: https://link.springer.com/article/10.1007/s10549-008-9901-z
In the current study we found that the presence of SV40 in BC correlates inversely with HER2 overexpression (P = 0.008). Our study is the first to demonstrate such correlation in human clinical cancer trials. HER2 (also named C-erbB-2, neu) is a protooncogene known to be overexpressed in ∼30–50% of human breast cancers [63].
HER2 overexpression plays an important role in human BC development and metastasis; it is also associated with therapeutic resistance and poor prognosis, and represents an important target for recent cancer therapies [64]. An interesting in vitro study has shown recently that SV40 large T antigen can act as a transforming suppressor of HER2 overexpressing in human breast tumor cell lines by negatively regulating the HER2 promoter activity [65].
Effects of TAG on ovarian cancer:
Human epidermal growth factor receptor 2 (HER2) is frequently overexpressed in human ovarian cancers and its overexpression is associated with increased angiogenesis, increased metastasis and reduced survival. Inhibition of HER2 in HER2-overexpressing cancers can lead to reduced angiogenesis and improved survival. Previously, we reported that SV40 T/t-common polypeptide has transcriptional repression activity and can inhibit HER2 expression. In this study, we investigated the effect of T/t-common on the angiogenesis-inducing activity of HER2-overexpressing human SK-OV-3 ovarian cancer cells. We found that compared to conditioned medium from control SK-OV-3 cancer cells, conditioned medium from T/t-common-expressing SK-OV-3 cells had a reduced ability to induce endothelial cell migration and tube formation in vitro and microvessel formation in vivo. These data indicate that T/t-common can inhibit the ability of SK-OV-3 cancer cells to induce angiogenesis.
From: “SV40 T/t-common polypeptide inhibits angiogenesis and growth of HER2-overexpressing human ovarian cancer“ (2011)
At this point I need to do a literature search for Spike protein associations with HER2. Spike is the gift that keeps on giving.
EFGR: Epidermal Growth Factor Receptor, a protein on cells that can stimulate their growth and is a factor in tumorigenesis and metastases.
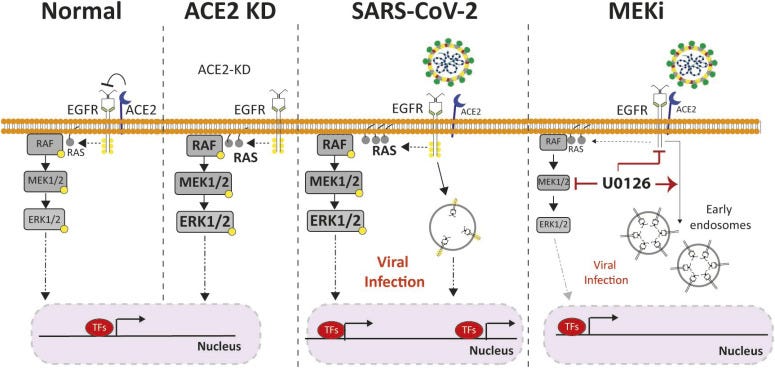
“Here, we demonstrate the activation of EGFR–MAPK signaling axis by the SARS-CoV-2 spike protein and we identify a yet unknown cross talk between ACE2 and EGFR that regulated ACE2 abundance and EGFR activation and subcellular localization, respectively.“ Source: “ACE2-EGFR-MAPK signaling contributes to SARS-CoV-2 infection“ (2023), https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10320016/
Although normally considered to act as a tumour suppressor, ACE2 after binding to Spike can, in the presence of growth factors, cause it to promote aggressive HER2 enriched breast cancer, a subtype associated with elevated ACE2 expression:
…The general level of expression of ACE2 is rather low in breast cancer subtypes except for the HER2-enriched and Basal-like subtypes. ACE2 expression was highest in HER2-enriched samples (n = 236; Table 1) when compared to the other subtypes in the METABRIC cohort (p<0.0001) (Fig. 1.a).
…ACE is equally expressed in apical and basolateral surfaces whereas, ACE2 is expressed on the apical surface of polarized cells [3]. Under normal conditions, the ACE2 does not internalize into the cell. However, binding of the spike protein of SARS-CoV and Cov2 to ACE2 triggers internalization reducing its activity on the cell surface.
…Further analysis of gene expression data from metastatic breast cancer samples from the translational component of the Swedish Multicenter TEX trial, showed that the basal-like (n = 30) and HER2-enriched (n = 38) metastatic lesions continued to show the highest mean expression of ACE2 compared to the other PAM50 subtypes (p<0.0001) and there was a positive correlation between EGFR and ACE2 expression in the HER2-enriched metastatic lesions [pcc= 0.36; (p = 0.024)].
…in the tumors with high ACE2 expression we did not find any positive correlation with proliferation associated genes like BCl2, CCNE1, CCND1 and BIRC5. Neither were high ACE2 levels correlated with tumor size (data not shown). These data argue against any synergistic role for ACE2 in further enhancing rates of proliferation in these tumor types. But high ACE2 expression was positively associated with EMT associated genes like Integrin β1 and Vimentin.
This observation coupled with the fact that metastatic lesions of both HER2-enriched and Basal-like breast cancer examined in the Swedish TEX trial continue to have high levels of ACE2 suggests, that in conjunction with over expressed receptor tyrosine kinase (RTK) growth factors, ACE2 a carboxy peptidase, capable of promoting internalization upon binding as demonstrated by SARS-Cov-2, might help promote signaling mechanisms that enhance metastatic behavior.
The fact that ACE2 had a positive association with EGFR in all the datasets further supports the conjecture that its metastasis promoting role may only be in the context of growth factor RTKs.
…Moreover, since centrally active ACE2 inhibitors like captopril and fosinopril can cross the blood brain barrier [25], they may be used in conjugation with HER2 targeting drugs for the treatment of brain metastasis; the most common site of metastasis for HER2 subtype of breast cancer.
From “High expression of ACE2 in HER2 subtype of breast cancer is a marker of poor prognosis“ (2021)
Reading round the literature, Spike binding to ACE2 causes in increase in epithelial-to-mesenchymal transition (EMT) through upregulation of EMT associated genes, as above, such as integrin β1, Vimentin, ZEB1 and AXL.
EMT is associated with acute respiratory distress syndrome (ARDS), cancer cell mobility, invasion, metastases and tumour resistance to apoptotic factors.18
Put another way, Spike is more oncogenic than TAG. Research shows that pro-cancer EMT pathways are a consequence of Spike downregulating (ie internalising) ACE2. In a positive feedback loop, EMT associated genes then further repress ACE2:
We find that ACE2 expression is restricted to a select population of epithelial cells. Notably, infection with SARS-CoV-2 in cancer cell lines, bronchial organoids, and patient nasal epithelium induces metabolic and transcriptional changes consistent with epithelial-to-mesenchymal transition (EMT), including up-regulation of ZEB1 and AXL, resulting in an increased EMT score. In addition, a transcriptional loss of genes associated with tight junction function occurs with SARS-CoV-2 infection. The SARS-CoV-2 receptor, ACE2, is repressed by EMT through the transforming growth factor-β, ZEB1 overexpression, and onset of EGFR tyrosine kinase inhibitor resistance.This suggests a novel model of SARS-CoV-2 pathogenesis in which infected cells shift toward an increasingly mesenchymal state, associated with a loss of tight junction components with acute respiratory distress syndrome-protective effects. AXL inhibition and ZEB1 reduction, as with bemcentinib, offer a potential strategy to reverse this effect.
From: “Lung Cancer Models Reveal Severe Acute Respiratory Syndrome Coronavirus 2–Induced Epithelial-to-Mesenchymal Transition Contributes to Coronavirus Disease 2019 Pathophysiology“ (2021)
Apart from SV40 promoter & dsDNA adulterated boosters, we need to try to reduce SARS-CoV-2 viral loads where possible too, even the “milder strains”:
In the present study, we investigated the impact of SARS-CoV-2 proteins on breast cancer cells (BCC). The results suggested that SARS-CoV-2 M protein induced the mobility, proliferation, stemness and in vivo metastasis of a triple-negative breast cancer (TNBC) cell line, MDA-MB-231, which are involved in the upregulation of NFκB and STAT3 pathways.
From: “SARS-CoV-2 M Protein Facilitates Malignant Transformation of Breast Cancer Cells“ (2022)
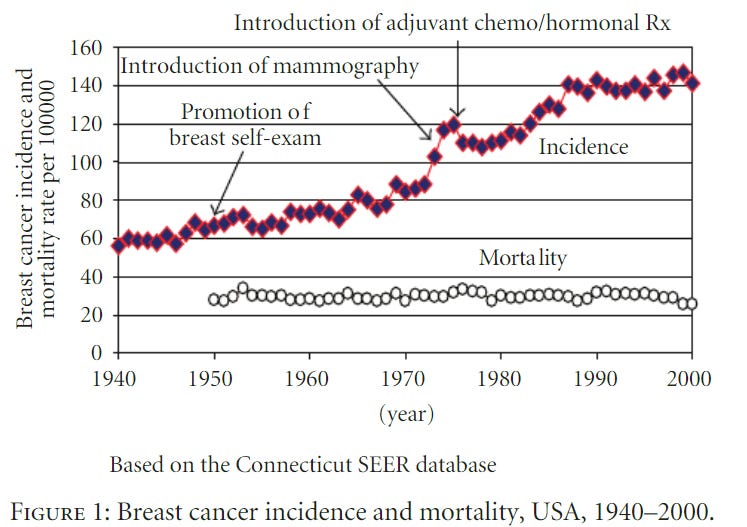
Breast cancer incidence after mass administration of SV40 contaminated polio vaccines
Next question: was mass inoculation of the population with live SV40 in the 50’s and 60’s associated with increased breast cancer incidence rates?
Correlation isn’t causation and introduction of screening may be a factor, but even with exposure to other carcinogens and poor lifestyle a 2-3 fold increase in 50 years takes some explaining.
Nb. Allow a latency time of 7-30 years after initiation.
Another consideration is that carcinogenic effects aren’t mutually exclusive. COVID-19 “vaccines” may have cumulative, if not synergistic effects. And the Pharma boys sure like to “rough up” your p53 at every opportunity, including by long term overprescribed corticosteroids. Must be good for business.
“According to the “multi-hit model of carcinogenesis” proposed by Sutherland and Bailer [248], it takes multiple different hits or insults to cells and their genetic machinery to cause a normal cell to become cancerous”.1920
Anyone harbouring or acquiring live SV40 as well as being administered flu vaccines and LNP/mRNA boosters may well be contributing to these curves surging upwards again in the next few years.
And after the disastrous polio vax rollout even now SV40 prevalence is in the range 1.3% - 25.6%, depending on which study you use. The more recent of these put it in the 2-12% range, with higher values detected in the USA.21
Key notes from the CTGTAC meeting with the FDA and 100 day vaccines
These need little comment from myself. The same questions that needed to be raised in 2020 about experimental mRNA COVID-19 gene therapy agents still need to be raised.
This is doubly important now due to the reckless abandonment of the precautionary principle and total regulatory capture, together with a culture of censorship and cover-ups. No better example of this is the “100 days mission”.22
The risk of doubling down on this sort of nonsense is that it further undermines the public’s trust in all interventions, including those that may be beneficial.
Once trust is lost it will be difficult to regain, and quite understandably too as a self defence mechanism:
From: “What will it take for the world to develop, and enable access to safe and effective vaccines against new pathogens in 100 days? And why is it crucial that the world achieves this 100 Days Mission?”, source: https://100days.cepi.net/
Keynotes from “FDA Cellular, Tissue, and Gene Therapies Advisory Committee (CTGTAC) Meeting #70, September 2-3, 2021, Toxicity Risks of Adeno-associated Virus (AAV) Vectors for Gene Therapy (GT)”23 (emphasis mine):
Outline
• Introduction
• Hepatotoxicity
• Thrombotic microangiopathy (TMA)
• Neurotoxicity
Dorsal root ganglia (DRG) toxicity
Brain magnetic resonance imaging (MRI) findings
• Oncogenicity
• Summary
Adeno-associated Virus (AAV) and AAV Vectors
• AAV is a small DNA virus (20 - 25 nm diameter, ~ 5 kb genome)
Widespread in humans and animals
More than 100 serotypes, with tropisms for different cell types
Only replicates in the presence of a helper virus (e.g., adenovirus, HSV-1, HHV-6, EBV)
No known disease association
• AAV vectors
Do not replicate
Are engineered to express a therapeutic gene
The public assessment report of the LNP/mRNA COVID-19 gene therapy agent BNT162b2 detailed findings of liver damage in healthy rats, but these findings were dismissed as being temporary. So that’s OK then.24
And dosing was something you only consider when worming your pet dog.
Scooby Couey is better treated than you
Discussion Questions for the Committee:
Hepatotoxicity
4. What factors (e.g., level of disease severity) other than weight should be considered to determine the vector dose for systemic administration?
5. Considering the risk of toxicities observed in clinical trials with high doses of AAV vectors,
a. Please discuss whether an upper limit should be set for the total vector genome dose per subject.
b. Given that many AAV products contain significant amounts of empty capsids, please discuss whether an upper limit should be set on the total capsid dose.
HCC: Hepatocellular carcinoma:
AAV Vector Integration and Oncogenicity Risk
• AAV vector genomes can integrate into host genomic DNA
Tendency to integrate near active genes
Vector integration has been seen in both animals and humans.
• HCC observed in several mouse models
Vector genome integration into Rian locus that encodes numerous regulatory RNAs
• Hepatic clonal expansion in canine model of hemophilia A
Integration into genes associated with cell growth and / or transformation
No liver nodules or oncogenesis
• HCC incidence may be influenced by multiple factors such as vector components, animal species / disease model, timing of administration and duration of follow-up after vector administration.
• One case report of HCC in clinical trial
HOPE-B trial (NCT03569891): AAV5 vector for treatment of hemophilia B
Unlikely that AAV vector contributed to HCC
• Risk-based approach for determining duration of long-term follow-up protocol
FDA guidance document Long Term Follow-up After Administration of Human Gene Therapy Products (January 2020)
Recommended follow-up duration up to 5 years for AAV vectors
Up to 15 years recommended for retroviral vectors or vectors that carry genome editing components
1. Please discuss the merits and limitations of animal studies to characterize the risk of AAV vector-mediated oncogenicity, and provide recommendations on specific preclinical study design elements, to include:
a. Animal species,healthy vs. disease models, and animal age
b. In-life and post-mortem assessments, including methods for integration analysis
c. Duration of follow-up, post-dose
2. Current literature suggests that various factors may affect AAV-mediated vector genome persistence, vector integration, and the risk of oncogenesis. Please discuss benefit-risk considerations for AAV vector-mediated oncogenesis, such as patient age at the time of treatment, pre-existing liver conditions (e.g., infection with hepatitis B or C virus), and high vector dose.
3. Considering the risk of oncogenesis,
a. Please provide recommendations on safety monitoring measures that should be included in clinical trials.
b. Please provide recommendations on duration, frequency, and method of long-term follow-up (LTFU) for recipients of AAV vectors.
4. Please discuss whether some vector designs may enhance the frequency of vector-mediated integration and the risk of oncogenesis. For example,how is the risk affected by promoter-enhancer elements, genome-targeted nucleases, or novel AAV vector designs for which there is limited clinical experience. Because AAV vectors can carry significant levels of co-packaged DNA impurities from the manufacturing process, is the risk of oncogenesis increased due to potential integration of non-vector DNA, and what types of studies should be performed to assess this risk?
Its enough to give you a functional neurological disorder (FND) if you try to rationalise the precautionary principle being advocated for gene therapy agents benefitting a relatively small number of patients each year vs those used as non-live “vaccines” after only 60 day trials (if at all) and 100 day approvals before potential administration to billions.
100 day vaccines. 100 days isn’t anywhere near long enough to assess for igG4 class switching, let alone cancer, immunosuppression, immune escape, cardiovascular disease, autoimmune or degenerative neurological disorders.
And a recent review by Rubio-Casillas et al. (2023) discusses how most non-live vaccines are associated with increased net mortality vs controls, whereas the reverse is true for many live vaccines such as BCG, likely due to beneficial non-specific effects (NSE’s).25
This makes the committees’ points even more pertinent to these and in effect they are total non-starters by these standards, unless perhaps you are facing near certain death soon and have nothing to lose.
Even then the risk of a virus will not be your main concern, the disease that is killing you or its symptoms will be the focus.
100 day bulsh!t. Out with the trash, where a lot of Pharma’s unsafe and ineffective junk belongs
Outcomes
Cancers with the shortest latencies after initiation include recurrences and soft tissue & blood cancers such as lymphomas at around 3-7 years. If there is going to be significant increase in new COVID-19 LNP/mRNA initiated cancers from this point forwards is where the bell curve starts to steepen.
The curve will have a long tail of incidence stretching out decades, and that’s without taking integration into the genome into consideration i.e. passing on into offspring who may have a higher risk.
Minimum latencies for edge cases are shorter still, and turbocancers due to impaired immune immunity are more likely to develop over shorter timescales:
The WTC Program Administrator has determined minimum latencies for the following five types or categories of cancer eligible for coverage in the WTC Health Program:
(1) Mesothelioma—11 years, based on direct observation after exposure to mixed forms of asbestos;
(2) All solid cancers (other than mesothelioma, lymphoproliferative, thyroid, and childhood cancers)—4 years, based on low estimates used for lifetime risk modeling of low-level ionizing radiation studies;
(3) Lymphoproliferative and hematopoietic cancers (including all types of leukemia and lymphoma)—0.4 years (equivalent to 146 days), based on low estimates used for lifetime risk modeling of low-level ionizing radiation studies;
(4) Thyroid cancer—2.5 years, based on low estimates used for lifetime risk modeling of low-level ionizing radiation studies; and
(5) Childhood cancers (other than lymphoproliferative and hematopoietic cancers)—1 year, based on the National Academy of Sciences findings.
From: “Minimum Latency & Types or Categories of Cancer“ (2015)
In response to my DMED data sent to the DHS subcommittee on investigations in January 2023, @DoD_USD_PR addressed non-cancerous injury/disease by saying it "was likely caused by the COVID-19 virus". Below is what he had to say about cancers. So basically the DoD is aware of an increase in cancer, buuuut, they're not going to investigate as to why.
I just received Cancer Sales Data for 2023 from industry sources.
Shocking spike in cancer drug sales, across all cancers but most notably Brain cancer. Look at Temodal sales below!
Temodal(generic name temozolomide) is an oral chemotherapy drug that is widely recognized as the most frequently used medication for treating certain types of brain cancer.
The drug is more than 20 years in the market and suddenly tripled in a span of two years from 2020 to 2022. I've never seen a 20 year old generic drug spike like this in my pharma career!
Most of us have seen this meme before, but as with the best comedy it is based on truth.
Despite all the clinical case and VAERS reports, years of medical training and thousands of research papers many doctors are still totally baffled! Really.
The pathophysiology and biochemistry behind turbo-atherosclerosis
DoorlessCarp’s Scientific Literature Reviews is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber. I do not receive any departmental funding, grants for software, online services or equipment etc. It’s your paid subscriptions that make these reviews possible, thank you all!
Thank you for reading DoorlessCarp’s Scientific Literature Reviews. This post is public so feel free to share it.
DoorlessCarp’s Scientific Literature Reviews is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
DoorlessCarp’s Scientific Literature Reviews is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
McKernan K, Helbert Y, Kane LT, McLaughlin S. Sequencing of bivalent Moderna and Pfizer mRNA vaccines reveals nanogram to microgram quantities of expression vector dsDNA per dose. Published online January 9, 2024. doi:10.31219/osf.io/b9t7m
Speicher DJ, Rose J, Gutschi LM, PhD DMW, McKernan K. DNA fragments detected in monovalent and bivalent Pfizer/BioNTech and Moderna modRNA COVID-19 vaccines from Ontario, Canada: Exploratory dose response relationship with serious adverse events. Published online January 9, 2024. doi:10.31219/osf.io/mjc97
“An Admission of Epic Proportions”: Health Canada Confirms DNA Plasmid Contamination of COVID Vaccines • Children’s Health Defense. Accessed January 9, 2024. https://perma.cc/6G94-8ZGV
Committee I of M (US) ISR, Stratton K, Almario DA, McCormick MC. Immunization Safety Review: SV40 Contamination of Polio Vaccine and Cancer. In: Immunization Safety Review: SV40 Contamination of Polio Vaccine and Cancer. National Academies Press (US); 2002. Accessed January 9, 2024. https://www.ncbi.nlm.nih.gov/books/NBK221112/
Frost G. The latency period of mesothelioma among a cohort of British asbestos workers (1978–2005).Br J Cancer. 2013;109(7):1965-1973. doi:10.1038/bjc.2013.514
Butel JS, Vilchez RA, Jorgensen JL, Kozinetz CA. Association between SV40 and non-Hodgkin’s lymphoma.Leuk Lymphoma. 2003;44 Suppl 3:S33-39. doi:10.1080/10428190310001623784
Sheng-Fowler L, Lewis AM, Peden K. Issues associated with residual cell-substrate DNA in viral vaccines.Biologicals. 2009;37(3):190-195. doi:10.1016/j.biologicals.2009.02.015
Sattar S, Kabat J, Jerome K, Feldmann F, Bailey K, Mehedi M. Nuclear translocation of spike mRNA and protein is a novel feature of SARS-CoV-2.Front Microbiol. 2023;14:1073789. doi:10.3389/fmicb.2023.1073789
Martini F, Corallini A, Balatti V, Sabbioni S, Pancaldi C, Tognon M. Simian virus 40 in humans.Infectious Agents and Cancer. 2007;2(1):13. doi:10.1186/1750-9378-2-13
Hachana M, Trimeche M, Ziadi S, Amara K, Korbi S. Evidence for a role of the Simian Virus 40 in human breast carcinomas.Breast Cancer Res Treat. 2009;113(1):43-58. doi:10.1007/s10549-008-9901-z
B U, C H, G R, et al. HER2-low expression in patients with advanced or metastatic solid tumors.Annals of oncology : official journal of the European Society for Medical Oncology. 2023;34(11). doi:10.1016/j.annonc.2023.08.005
Sutherl JV, Bailar JC. The multihit model of carcinogenesis: Etiologic implications for colon cancer.Journal of Chronic Diseases. 1984;37(6):465-480. doi:10.1016/0021-9681(84)90030-4
Humans IWG on the E of CR to. SIMIAN VIRUS 40. In: Malaria and Some Polyomaviruses (SV40, BK, JC, and Merkel Cell Viruses). International Agency for Research on Cancer; 2013. Accessed January 12, 2024. https://www.ncbi.nlm.nih.gov/books/NBK294242/
Gouglas D, Christodoulou M, Hatchett R. The 100 Days Mission—2022 Global Pandemic Preparedness Summit.Emerg Infect Dis. 2023;29(3):e221142. doi:10.3201/eid2903.221142
Rubio-Casillas A, Rodriguez-Quintero CM, Redwan EM, Gupta MN, Uversky VN, Raszek M. Do vaccines increase or decrease susceptibility to diseases other than those they protect against?Vaccine. Published online December 29, 2023. doi:10.1016/j.vaccine.2023.12.060
The broad spectrum host-directed agent ivermectin as an antiviral for SARS-CoV-2 ? (2021)
"... It was initially shown to inhibit nuclear import not only of IN, but also of simian virus SV40 large tumour antigen (T-ag) and other IMPα/β1- (but not IMPβ1-) dependent cargoes, consistent with the idea that IMPα (not IN) is the direct target of ivermectin [34,35]. Subsequent work has confirmed this, with ivermectin’s ability to inhibit the nuclear accumulation of various different host, including NF-kB p65 [37,38] and viral proteins demonstrated in transfected and infected cell systems (see Table 1) [14,34]. Ivermectin’s ability to inhibit binding of IMPα to the viral proteins NS5 and T-ag has also been confirmed in a cellular context using the biomolecular fluorescence complementation technique [11] (Table 1)."































IVM helps stop TAG going into the nucleus:
The broad spectrum host-directed agent ivermectin as an antiviral for SARS-CoV-2 ? (2021)
"... It was initially shown to inhibit nuclear import not only of IN, but also of simian virus SV40 large tumour antigen (T-ag) and other IMPα/β1- (but not IMPβ1-) dependent cargoes, consistent with the idea that IMPα (not IN) is the direct target of ivermectin [34,35]. Subsequent work has confirmed this, with ivermectin’s ability to inhibit the nuclear accumulation of various different host, including NF-kB p65 [37,38] and viral proteins demonstrated in transfected and infected cell systems (see Table 1) [14,34]. Ivermectin’s ability to inhibit binding of IMPα to the viral proteins NS5 and T-ag has also been confirmed in a cellular context using the biomolecular fluorescence complementation technique [11] (Table 1)."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7577703/
Just say no.