short story - novelette - novella - novel - PhD thesis - Trump’s tariff list - War and Peace - U.S. Tax Code
Updates:
27th April ‘25: Addendum: “DMSO induces drastic changes in human cellular processes and epigenetic landscape in vitro”.
Any extracts used in the following article are for non-commercial research and educational purposes only and may be subject to copyright from their respective owners.
On July 31. 1980, Senator Mark Hatfield of Oregon testified at a hearing of Senator Edward Kennedy's sub-committee on health:
“I cannot make an absolute statement that DMSO is indeed the wonder drug of our century; but every bit of evidence I encounter reinforces the premise that it is. After 1,200 scientific publications on the merits of DMSO, after international symposia in Germany, the U.S., and Austria - all concluding that DMSO is safe and effective - after three separate pharmaceutical firms have submitted for new drug applications to the FDA (all rejected), DMSO is still not available to Americans, although it is available in many other countries. I have urged the Senate to support my legislation (to approve DMSO) on behalf of all Americans who are suffering from diseases untreatable by any other known substance and those who may have need of this drug in the future.”
From: “Chapter 6: DMSO - The Persecuted Drug; by Dr. Stanley Jacob
[from the book: Politics In Healing by Daniel Haley] 27 Feb 2011”
I need to discuss alternative therapeutics more, and will be doing so over the next few months. Part of the reason is that it’s an area I have neglected for some time, choosing instead to focus on mechanisms and consequences of IgG4 class switching, and why I would recommend not going near replicon gene agents with a ten-foot bargepole…
This time, the elixir of life known as dimethylsulfoxide (DMSO) is the focus. I have seen headlines from some fantastical articles by famous authors such as the Midwestern Doctor or Dr Mercola. However, to stay fair and objective, I have deliberately refrained from reading these.
Think of this Substack as another valproate or chlorine dioxide (CDS)-type review. I start with a white sheet and report as I find, good or bad.
By restricting myself to pre-prints and peer-reviewed research, I risk adopting establishment-journal censorship regimes at the expense of accounts derived from personal anecdotes. But by focusing on underlying mechanisms and in vitro/in vivo studies, it should provide a useful reference.
Before penning this piece, all I knew about DMSO was that it has been used as a carrier and a control in various experiments, and that many claims have been made about its therapeutic properties.
I will cover the following points:
Explain what DMSO is, and how it was discovered and developed.
Take a look at what benefits have been reported anecdotally for DMSO, and whether there are any known risks to health.
Review some of the research literature supporting these claims.
Dosing information or contraindications.
As ever in medicine, clinical beats lab. If it works for you, then it works!
It doesn’t make you right or me wrong. It just means that existing research may have been flawed, or more research is required, or the dosing was different. But we should both be better informed as to the mechanisms, and any serious safety concerns raised.
And we are all well aware of how Big Pharma works to suppress alternatives that do work, where these pose a threat to their business plans and narratives. The list is long.
Discussion
In January 2012, Paul May (currently Professor of Physical Chemistry at the University of Bristol) wrote an excellent guide when he featured DMSO as “Molecule of the Month”.
I reproduce his work in full here, as it’s succinct.
(Emphasis in bold, as ever, and lightly edited for typos)
One of the first observations is that its solvent properties may be one of the reasons why it is useful to us, for trafficking other therapeutics through otherwise almost-impermeable membranes such as the skin. Magnesium springs to mind here, too:
Dimethylsulfoxide
(DMSO)
The smelly solvent that may have a variety of medical uses
It's just a smelly solvent, isn't it?
Yes, and no. It is a good solvent which is frequently used for reactions involving salts, especially nucleophilic substitutions. But it has the unusual property that it can pass through membranes and rubber gloves quite easily, and penetrate the skin. After contact with it on the skin, some people find that DMSO is secreted out onto the surface of the tongue causing a garlic-like taste in the mouth, and garlic breath!
I need to differentiate between the therapeutic properties of DMSO itself vs the drug in solution. If it is a painkiller, anti-inflammatory, and an antioxidant, then what are the mechanisms?
Yuck! What use is that?
Well, actually, that property is quite useful, because DMSO can dissolve certain useful medicines and transport them through the skin without the need for an injection. DMSO is predominantly used as a localised painkiller, as an anti-inflammatory, and an antioxidant. It is frequently mixed with antifungal medications, enabling them to penetrate the skin, and also toenails and fingernails.
Originally, it arose as a by-product of the paper production process:
Who discovered this?
DMSO is a by-product of kraft pulping, which is the conversion of wood into wood pulp consisting of almost pure cellulose fibres. Wood-chips are treated with a mixture of sodium hydroxide and sodium sulfide (known as white liquor), that break the bonds that link lignin to cellulose. Oxidation of dimethyl sulfide with oxygen or nitrogen dioxide gives DMSO. DMSO was first synthesized in 1866 by the Russian scientist Alexander Zaytsev (photo, right).
It took almost another century before medicine started to find uses for it:
But the history of DMSO as a pharmaceutical began in 1961, when Dr. Stanley Jacob was head of the organ transplant program at Oregon Health Sciences University. While investigating the potential for DMSO as a preservative for organs, he discovered that it penetrated the skin quickly and deeply without damaging it, and became intrigued.
It solidifies at just below your typical room temperature.
The relative molecular mass of water is 18.015 g/mol, vs 78.13 g/mol for DMSO. In other words, it has a significantly higher molecular mass.
Aprotic: A solvent that cannot donate a hydrogen ion (i.e. a proton).
Polar aprotic solvents: Lacking an acidic proton, these have a separation of charge within the molecule, i.e., a dipole moment. They can dissolve both polar and nonpolar compounds. Both DMSO and nitromethane have this property.
What are its properties?
Molecular formula: (CH3)2SO
Relative molecular mass: 78.13
CAS registry: [67-68-5]
Melting point: 18.5°C
Boiling point: 189°C
DMSO is a clear, colourless, hygroscopic liquid. It is a dipolar aprotic solvent, miscible with water and soluble in many polar organic solvents such as alcohols, ester, ketones and chlorinated solvents. It will dissolve many inorganic salts.
One of the reasons it penetrates the skin so well is due to interactions with lipids. But this can be a curse as well as a blessing:
Its ability to penetrate the skin is due to the fact that the molecule is highly polar, but also because it has two methyl groups which interact strongly with lipids in the skin. One particular danger associated with DMSO is that although not considered toxic itself, it is highly effective at transferring other (potentially toxic) substances into the body via skin contact. For example skin contact with DMSO and a cyanide salt would pose a high risk of cyanide poisoning.
Although less popular due to latex allergies, your usual lab PPE may not protect you:
DMSO will dissolve and penetrate ordinary rubber gloves, so alternative materials should be used such as butyl rubber or blue nitrile.
Any risk of organ damage catches your attention, and be careful what you mix it with.
Acid chlorides include oxalyl chloride, acetyl chloride, and benzoyl chloride.
No smoking!
(I’m sure I didn’t need to tell you that)
Although it is non-toxic for short exposures, other safety concerns associated with DMSO are that it can be irritant and harmful at higher dosages. Prolonged exposure can lead to dermatitis, and possibly to liver and kidney damage. It can produce explosive reactions with some compounds, such as acid chlorides.
It’s used in a wide range of non-therapeutic applications:
What's it used for?
DMSO is widely used as a solvent in many organic syntheses and has several important industrial applications including polymer chemistry, pharmaceuticals and agrochemicals. It is a dipolar aprotic solvent, and has many similar properties to dimethylformamide (DMF) (see structure right).
It is often used as the solvent for SN2 syntheses, and in the preparation of organometallics such as ferrocene. It is used as a rinsing agent in the electronics industry, and deuterated DMSO-d6 is used as a solvent for NMR spectroscopy. It is particularly good for this as it will dissolve a wide range of compounds, and does not interfere with the sample signals excessively.
It makes a great paint stripper and is cryoprotective:
DMSO is used in antifreeze and it makes an effective paint stripper, which is safer than many other products such as nitromethane and dichloromethane. DMSO is used as a cryoprotectant for protecting human and other biological tissues when frozen for storage.
Veterinary uses are always interesting, partly because the owner isn’t likely to pay you good money for snake oil, or risk the health of very valuable bloodstock:
DMSO also has several veterinary uses, such as a liniment for horses, which relieves pain when rubbed onto the muscles.
I’m following a trail that is very well trod.
A PubMed search alone returns nearly 4,000 papers, dating back to 1946:
It has a lot of uses. So why is it controversial?
According to Stanley Jacob (photo left) more than 40,000 articles on the chemistry of DMSO have appeared in scientific journals. 11,000 articles have been written on its medical and clinical implications, and in 125 countries throughout the world doctors prescribe it for a variety of ailments, including pain, inflammation, scleroderma, interstitial cystitis, arthritis and elevated intercranial pressure.
Why the disconnect between what we know so far vs FDA (Fraud, Deaths, Atrocities) approvals?
The not-so-hidden hand of Big Pharma at work:
Why is the FDA Funded in Part by the Companies It Regulates?
Nearly half the agency's budget now comes from 'user fees' paid by companies seeking approval for medical devices or drugs
The Food and Drug Administration has moved from an entirely taxpayer-funded entity to one increasingly funded by user fees paid by manufacturers that are being regulated. Today, close to 45% of its budget comes from these user fees that companies pay when they apply for approval of a medical device or drug.
As a pharmacist and medication and dietary supplement safety researcher, I understand the vital role that the FDA plays in ensuring the safety of medications and medical devices.
But I, along with many others, now wonder: Was this move a clever win-win for the manufacturers and the public, or did it place patient safety second to corporate profitability? It is critical that the U.S. public understand the positive and negative ramifications so the nation can strike the right balance.
… While the number and speed of drug approvals have been increasing over time, so have the number of drugs that end up having serious safety issuescoming to light after FDA approval.
In one assessment, investigators looked at the number of newly approved medications that were subsequently removed from the market or had to include a new black box warning over 16 years from the year of approval. These black box warnings are the highest level of safety alert that the FDA can employ, warning users that a very serious adverse event could occur.
Before the user fee act was approved, 21% of medications were removed or had new black box warnings as compared to 27% afterwards.
Tens of thousands of medical research papers going back decades, discussing how DMSO does, or doesn’t do something, and all they can manage is just two approvals by 2012?
That’s a lot of research funding and time to spend on a substance with only two medicinal uses.
I looked to see if any more approvals followed, and if you exclude preserving transplant organs, even now, it is only approved for one human indication: the treatment of a type of cystitis.
Go steady, FDA!
You can see why it’s not in their interest. You can buy a half-litre of the stuff, at pharmaceutical grade, for around $35 (£30):
Yet in the US, until 2016 DMSO had Food and Drug Administration (FDA) approval only for use as a preservative of organs for transplant and for interstitial cystitis, a bladder disease!
After its clinical effects were discovered in 1961 it wasn't long before reporters, the pharmaceutical industry, and patients with a variety of medical complaints jumped on the news. However, since DMSO was widely available as a solvent and industrial chemical (rather than as a restricted drug), patients did not need to obtain a doctor's prescription to get hold of it. As a result, many patients began to dose themselves, often without knowing about the correct dosage or potential side-effects.
I can’t accept this explanation. Surely this is a good reason to do more randomised controlled trials, not less, or to dismiss a lack of reports of poisoning:
As a result of these uncontrolled treatments, the FDA was unable to confirm that its experimentation and use were safe. The mainstream medical community became soured, and DMSO has been tainted with a bad reputation ever since.
Agreed, the garlic smell would be a challenge, but not intractable; in vivo animal studies should be easier to blind with ventilation and fume cupboards. The mouse isn’t likely to care! And the FDA is quite happy to approve some drugs after unblinded clinical studies1.
Another problem with clinical testing is that its main side-effect, garlic-smelling breath, makes double-blind experiments difficult, because the patients (and doctors) can always tell who had been given DMSO and who had the placebo!
Another irrelevance. It doesn't seem to stop ill people from buying it by the bottle and self-medicating:
The smell also puts off drug companies, who fear it would be hard to market.
The Willie Sutton Rule, which is probably 90% of the reason it’s not licensed:
A bigger problem for the drug companies, however, is that because DMSO is a widespread industrial chemical and solvent, no company would be granted an exclusive patent for its medical use. Without potential profits, drug companies would not spend millions on the clinical testing required for FDA approval.
If only they applied the one-case-rule to pulling the DeathVax™:
The controversy really began in November 1965, when an Irish woman died of an allergic reaction after taking DMSO together with several other drugs. Although the precise cause of death was never determined, the press reported it to be DMSO.
In humans, DMSO has been applied topically for up to 7 years without lens toxicity:
… In a more encompassing report on human utilization from the Second International DMSO Symposium in Vienna, an astounding 9521 patients were followed and treated with DMSO for up to 2.5 years [27]. There was not a single instance of lens toxicity reported in any of these study participants.
In 1973, a landmark report published in the Annals New York Academy of Sciences further supported its safe human use. Here, a topical DMSO aqueous solution was administered daily to 65 patients with up to 4–7 years of follow-up. No observable toxicity was found outside of transient irritation and occasional conjunctival erythema [28].
More recently, one case report of DMSO-related lenticular pigmentary change was noted in a woman being treated for interstitial cystitis [29]. Her treatment was with RIMSO-50, administered via multiple bladder washouts. The pigmentary changes were thought to be responsible for mild hypermetropic shift; however, no change in best corrected visual acuity was noted.
From: “Rosacea Blepharoconjunctivitis Treated with a Novel Preparation of Dilute Povidone Iodine and Dimethylsulfoxide: a Case Report and Review of the Literature” (2015)
Hydroxychloroquine use was also buried by such BS:
At around the same time laboratory animals that had been given doses of DMSO many times higher than would be given humans developed abnormalities in their eye lenses. Two months later the FDA closed down all clinical trials of DMSO in the United States, citing the woman's death and the negative findings from animal experiments as the reason.
Bringing in an MSDS here, it’s rated as safe, and the dose to kill 50% of those administered (the LD50) is high. It has a high therapeutic index (ratio), and higher is better. It is many times less toxic than aspirin (LD50 14,500 - 40,000 mg/kg vs. 200 mg/kg in rats2).
They even conducted mutagenicity and teratogenicity tests, which is more than can be said for the DeathVax™ or the replicon agent Kostaive:
Guess who's been using DMSO...or was it just beans for dinner?
But 20 years and hundreds of laboratory and human studies later, no other deaths have been reported, nor have changes in the eyes of humans been reported or claimed.
None of this cuts any ice with the FDA:
However, the FDA has refused seven applications to conduct clinical studies, and approved only 2, one for intersititial cystitis which was subsequently approved for prescription use in 1978, and another for the treatment of closed head injury.
In 2016 the EPA finally approved DMSO for medicinal use in the US, which at last opens up a lot of potential uses.
From the mechanistic view, I’m more interested in its role as a standalone therapeutic rather than as a carrier:
What could it be used for?
Its main potential use is to ferry other drugs across membranes, including drugs such as morphine sulfate, penicillin, steroids, and cortisone. The fact that it can do so without opening the skin removes many problems associated with infections. It can also act as a local aneasthetic, reducing pain by blocking peripheral nerve fibres. Burns, cuts, and sprains have been treated with DMSO, and relief is reported to be almost immediate, lasting up to 6 hours. Because is an antioxidant, i.e. a scavenger of the free radicals that gather at the site of injury, DMSO can be used to reduce inflammation.
This is useful, but would prolonged use lead to tolerance or side effects? Does it suppress any root causes of disease?
Ideally, you shouldn't need to take any therapeutic drug, however safe and effective it may be. Instead, you could start by reviewing your diet, exercise, and lifestyle, or at least address these alongside:
Examples include relieving the symptoms of people with rheumatoid arthritis and chronic low-back inflammatory-type symptoms, silicon immune toxicity syndromes, or any kind of autoimmune process.
I won’t have the space to walk through every paper I can find for all these potential applications; this is a nice problem to have:
DMSO may also be used as a clot-busting agent to help stroke patients, or to reduce intercranial pressure in patients with severe head trauma. It's been used to treat minor cuts and burns, soft tissue damage, local tissue death, skin ulcers, and burns, and may even delay the spread of certain types of cancer. Toxic shock, radiation sickness, and septicemia have also been suggested as possibly being responsive to DMSO.
An intriguing possibility is that due to its antioxidant powers, DMSO could be used to mitigate some of the effects of ageing, but little work has been done to investigate this yet.
Looks like the scientist working on the anti-ageing properties of DMSO took things a bit too far...
“… the study of kinetics of absorption, distribution, metabolism and excretion (ADME) of drugs and their corresponding pharmacologic, therapeutic, or toxic responses in man and animals.”3
There was a lot of publicity and controversy about DMSO in the 1960s and 70s. There was also some groundbreaking research into the pharmacokinetics, and I can cite a couple here.
The first is a paywalled extract that defies OCR, but it presents some interesting findings, derived from experiments using radioactive labelled DMSO.
Highlights from “ABSORPTION, DISTRIBUTION AND ELIMINATION OF LABELED DIMETHYL SULFOXIDE IN MAN AND ANIMALS” by Kolb et al. (1967)4.
After being applied to the skin of rats, the maximum arterial counts were reached in only ten minutes. In other words, it very quickly gets absorbed and enters your circulation.
The half-life was greater than 10 hours:
Results were similar in beagles; in humans, it only took 5 minutes to enter the blood, levels plateaued for 4-6 hours, but remained elevated and almost unchanged for 1 1/2 to 3 days.
Their experiments showed that in dogs, over 90% of the cutaneously applied dose was absorbed. By day 14, barely any detectable amounts remained:
Our next study was from 1971 and conducted along similar lines, but using miniature pigs and gas chromatography instead of radioactive labelling.
Key takes from “ABSORPTION, EXCRETION, AND BIOTRANSFORMATION OF DIMETHYL SULFOXIDE IN MAN AND MINIATURE PIGS AFTER TOPICAL APPLICATION AS AN 80% GEL“ by Wong et al.5:
t.i.d: “Three times a day”.
The absorption, excretion, and biotransformation of dimethyl sulfoxide (DMSO) 80% gel, DEMASORB®, was studied in man and in miniature pigs. DMSO 80% gel (15 cc, t.i.d.) was applied topically to the elbows of human subjects and allowed to remain there for 30 minutes after each application.
Even from the elbow, which is quite bony, absorption ranged from 25-40%:
Under these conditions, daily absorption of DMSO 80% gel ranged from 25 to 40% of the total dose. DMSO 80% gel (15 g, t.i.d.) was completely absorbed within 4 hours after application to the shaved backs of miniature pigs.
A small amount of the DMSO is metabolised to dimethylsulphide (DMS) and lost through exhalation; much of the DMSO is metabolized to dimethyl sulfone (DMSO2); and most of the DMSO and DMSO2 is excreted in urine, with DMSO2 the largest fraction:
Both man and miniature pig transformed DMSO to dimethyl sulfone (DMSO2) and dimethylsulfide (DMS). DMSO and DMSO, were excreted in the urine, whereas DMS was eliminated in the expired air.
In man, the relative amounts of DMSO and DMSO, in the plasma were similar to those found in the urine. The biological half-life of DMSO, in both the plasma and urine of man was 2.5 to 3 days.
Urinary excretion of DMSO plus DMSO, ranged from 9 to 35% of the dose in both man and miniature pigs; only 1.6% of the dose was present in the feces of miniature pigs. Whereas DMSO, was the main excretory product in the urine of man, DMSO was the major component in the urine of miniature pigs.
Dimethyl sulfoxide (DMSO) has been used to facilitate the percutaneous absorption of drugs ( 1, 2, 3) and as a medication for the treatment of pain associated with various joints of the body ( 4).
250cm2: An area of skin measuring ~15 x 15 cm.
Studies in man. Studies were conducted at Lankenau Hospital, Philadelphia, Pa. under the supervision of Dr. John J. Blizzard. DMSO 80% gel (15 cc, equivalent to 16.5 g) was applied t.i.d. around the elbow of normal male subjects to cover an area of approximately 250 cm2".
The application of DMSO 80% gel t.i.d. was continued for 8 days. Urine was collected daily at 4-hour intervals, except from midnight to 8 AJI.1, when an 8-hour collection was made. A sample of plasma was obtained once daily at 2 PM. Concentrations of DMSO and dimethyl sulfone (DMSO2) in urine and plasma were determined by gas chromatography.
Samples of expired air were collected from human subjects for the determination of volatile metabolites by having them breathe into a bag equipped with a check valve, permitting air to flow in only one direction. Each collection was carried out for 5 minutes.
From: “Fig. 1. Absorption of DMSO 80% gel in man. Each of the three subjects received 15 cc of DMSO 80% gel, t.i.d. Each bar is the amount of gel absorbed after a single application.” Source: https://www.jidonline.org/article/S0022-202X(15)47943-6/pdf
From: “TABLE. DMS in the expired air of man. Samples were taken for 5-minute intervals during each of the three periods in which DMSO 80% gel was present on the skin. Each figure for DMS expired is an average of figures for the three collection periods each day. The number of subjects participating in the test on each day is shown in parentheses.” Source: https://www.jidonline.org/article/S0022-202X(15)47943-6/pdf
Both DMSO and DMS became undetectable within 24 hours, whereas DMSO2 persisted and was detectable in the urine for several days, according to various studies:
In man, Gerhards and Gibian (11) reported that DMSO and DMSO2 were excreted in the urine after intravenous or topical administration of DMSO. The excretion of DMSO in the urine diminished rapidly and the drug was not detectable 24 hours after its administration, but DMSO2 was detectable in the urine 96 hours after administration of DMSO.
Kolb et al. (10) reported that about 40% of the dose was eliminated in human urine during the first week after topical administration of 50% DMSO;
DMS was detected in the expired air during the first 6 hours after administration but none could be demonstrated after 24 hours. Thus, the results of the present studies in man show a metabolic disposition for DMSO 80% gel similar to that described previously for unformulated DMSO.
In 1985, Layman & Jacob studied “The absorption, metabolism and excretion of dimethyl sulfoxide by Rhesus monkeys”6. These should approximate human physiology more closely, and the administration was oral instead of topical.
Key takes (paywalled):
The absorption and excretion of dimethyl sulfoxide (DMSO) were studied in Rhesus monkeys (Macacamulatta) given daily oral doses of3 gms DMSO/kg B.W. for 14 days.
DMSOand its major metabolite, dimethyl sulfone (DMSO2), were measured in serum, urine and feces by gas-liquid chromatography.
DMSO was absorbed rapidly, reached a steady state blood level after 1 day and then was cleared from blood within 72 hrs after ending treatment.
Serum DMSO declined in a linear fashion on semilogarithmic coordinates as described by second order kinetics. It had a half-life of 16 hrs.
DMSO2 appeared in blood within 2 hrs and reached a steady state concentration after 4 days of treatment.
DMSO2 was cleared from blood about 120 hrs after DMSO administration was stopped.
The half-life in blood was 38 hours:
Its half-life in blood was calculated to be 38 hrs. Urinary excretion of unmetabolized DMSO and DMSO2 accouted for about 60% and 16%, respectively, of the total ingested dose.
Neither DMSO nor DMSO2 was detected in fecal samples. However, when added to fecal samples, DMSO was degraded rapidly.
Although dimethyl sulfide (DMS) was not measured, some DMSO was metabolized to this compound because of the particular sweetness of breath of the monkeys.
We conclude that the absorption of DMSO by monkeys is similar to that for humans, but that its conversion to DMSO2 and urinary elimination are more rapid in monkeys.
For a deeper dive into how DMSO changes skin to become much more permeable, we owe thanks to Richard P. Oertel and his 1977 paper “Protein conformational changes induced in human stratum corneum by organic sulfoxides: An infrared spectroscopic investigation”7.
As ever with obscure older papers, it is paywalled and only the abstract is freely available.
α-helix protein:
From "Wiki: “An alpha helix (or α-helix) is a sequence of amino acids in a protein that are twisted into a coil (a helix).
The alpha helix is the most common structural arrangement in the secondary structure of proteins. It is also the most extreme type of local structure, and it is the local structure that is most easily predicted from a sequence of amino acids.
The alpha helix has a right-handed helix conformation in which every backbone N−H group hydrogen bonds to the backbone C=O group of the amino acid that is four residues earlier in the protein sequence.”
Key:
Nitrogen (blue) - Hydrogen (light grey)
bonds to:
Oxygen (red) - Carbon (dark grey)
β-sheet protein:
From "Wiki: “The beta sheet (β-sheet, also β-pleated sheet) is a common motif of the regular protein secondary structure. Beta sheets consist of beta strands (β-strands) connected laterally by at least two or three backbone hydrogen bonds, forming a generally twisted, pleated sheet. A β-strand is a stretch of polypeptide chain typically 3 to 10 amino acids long with backbone in an extended conformation. The supramolecular association of β-sheets has been implicated in the formation of thefibrilsandprotein aggregates observed in amyloidosis, Alzheimer's diseaseand otherproteinopathies.”
From: “Three-dimensional structure[1] of parts of a beta sheet in green fluorescent protein” By Theislikerice - Own work, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=108233511
From Oertel (1977), we learn that DMSO dehydrates the stratum corneum by displacement and changes the protein conformation from α-helix to antiparallel-chain β-sheet, which is looser and much more permeable.
Fortunately, with DMSO, the process is reversed when your skin gets rehydrated; you don’t stay like it indefinitely!
Abstract
Formation of the antiparallel-chain β-sheet protein conformation is induced in in vitro human stratum corneum by three homologous organic sulfoxides known to enhance skin permeability: dimethylsulfoxide (Me2SO), hexylmethylsulfoxide (HxMeSO), and decylmethylsulfoxide (DecMeSO). Me2SO and HxMeSO apparently function by displacing water molecules bound to polar protein side-chains, whereas DecMeSO probably interacts hydrophobically with the protein.
It is not caused by dissolving your lipids away, which would be a bad thing™.
The conformational transition does not result from lipid removal. The β-sheet protein, most likely formed in normally α-helical portions of the intracellular keratin filaments, is reconverted to α-helix upon rehydration of the tissue.
The other solvents tested were more reactive than DMSO:
Though neat Me2SO produces the most β-sheet of all treatments examined, the sequence of ability to promote β-sheet formation at the 1M level is HxMeSO > DecMeSO > Me2SO.
These variables all affect transformation rates:
Spectroscopic evidence is presented regarding the dependence of β-sheet formation on sulfoxide concentration, treatment duration, pH, and tissue hydration. The relationship of this conformational change to the enhancement of skin permeability is briefly discussed. The result of sulfoxide treatment is different from results of sodium dodecylsulfate and heat treatments of stratum corneum.
I do have full access to a second study from 1995, which confirmed the findings and added to our knowledge base.
They used fourier transform raman spectroscopy to identify and quantify skin protein secondary structures.
There are different models, some with more equipment built-in than others:
There are several methods for measuring the temporal coherence of the light (see: field-autocorrelation), including the continuous-wave and the pulsed Fourier-transform spectrometer or Fourier-transform spectrograph.
… The term "Fourier-transform spectroscopy" reflects the fact that in all these techniques, a Fourier transform is required to turn the raw data into the actual spectrum, and in many of the cases in optics involving interferometers, is based on the Wiener–Khinchin theorem.
… To be more specific, between the light source and the detector, there is a certain configuration of mirrors that allows some wavelengths to pass through but blocks others (due to wave interference). The beam is modified for each new data point by moving one of the mirrors; this changes the set of wavelengths that can pass through.
The Fourier-transform spectrometer is just a Michelson interferometer, but one of the two fully reflecting mirrors is movable, allowing a variable delay (in the travel time of the light) to be included in one of the beams.
Fourier transform infrared (FT-IR) or Raman spectroscopy are one of the most powerful techniques for determining the secondary structure of globular proteins in aqueous solutions (Arrondo et al. 1993, Surewicz et al. 1993) and are also often employed as investigation tools for monitoring the nature of changes in the conformation of the proteins (Fang and Dalgleish 1997, Farrell et al. 2002a, Le Quéré et al. 1999, Lefèvre and Subirade 1999, Lübke et al. 1999, Nonaka et al. 1993, Qi et al. 1997, 2001b, Subirade et al. 1998, Tian et al. 2004).
It is a quick approach which allows identification of the types of secondary structure (α-helix or β-sheet) involved in structural changes, but the resolution is too low to determine the precise localisation of these changes.
From chapter “9 - Protein–flavour interactions” of “Flavour in Food”
Key takes from “Fourier transform raman spectroscopy of interactions between the penetration enhancer dimethyl sulfoxide and human stratum corneum” by Anigbogu et al8.
The stratum corneum, the outermost layer of human skin, is the major barrier to transdermal delivery of most drugs. Dimethyl sulfoxide (DMSO) is an established penetration enhancer.
To assess its mechanism of flux enhancement, Fourier transform (FT) Raman spectroscopy was used to study the effects of a series of aqueous solutions of DMSO on hydrated human stratum corneum following treatment for 1 h.
The results showed changes in the stratum corneum keratin from an a-helical to a {3-sheet conformation.
They found the minimum effective concentration of DMSO as a carrier to be above 60% v/v, and that the effects were not just due to protein conformational changes or drug partitioning, but due to lipid reorganisation too:
In addition, at concentrations >= 60% v/v, at which DMSO enhances drug flux, there was evidence of interactions with stratum corneum lipids.
These observations suggest that the skin penetration enhancement produced by DMSO not only involves changes in protein structure but may also be related to alterations in stratum corneum lipid organization, besides any increased drug partitioning effects.
In the normal condition, human skin works to keep in water, and to keep out noxious substances:
Human skin functions as an excellent barrier in two directions, controlling the loss of water and other body constituents while preventing the entry of noxious substances from the external environment.
The percutaneous route for drug administration holds several advantages over the oral or systemic routes such as the avoidance of first pass gut and hepatic metabolism, the ability to deliver drugs continuously, potentially fewer side effects, better patient compliance and ease of rapid cessation of therapy (Barry, 1983; Weissinger, 1993). Widespread use of the skin for drug delivery is, however, limited because of the aforementioned barrier properties.
The outermost stratum corneum is responsible for most of the barrier properties:
Human skin consists essentially of three tissue layers, the multi-layered epidermis, the underlying dermis containing a matrix of connective tissue woven from fibrous protein and the deep subcutaneous fatty layer.
The outermost stratum of the epidermis, the stratum corneum or horny layer, is recognized as contributing the rate-limiting step in the barrier function of human skin to most drugs (Blank, 1953; Barry, 1983).
“You may feel a little scratch.”
It’s only about 10 µm (0.01 mm) thick when dry and about 25µm (0.025 mm) fully hydrated, which helps to explain why DMSO is so effective:
This tissue typically consists of 10-15 layers of flattened, keratinized dead cells embedded in a lipid-rich matrix and may be about 10 /µm when dry but usually swells to several times this thickness when hydrated.
The stratum corneum consists mainly of protein, with 5-15% lipids:
The barrier properties of the stratum corneum are controlled by its composition: 75- 80% proteins, 5-15% lipids and 5-10% unidentified material on a dry weight basis (Wilkes et al., 1973).
Dimethyl sulfoxide (DMSO) is a dipolar aprotic solvent with a wide range of physical and chemical properties to which its diverse physiological and pharmacological activities are attributable.
It is the earliest and the most widely studied skin penetration enhancer. It has been found to improve the permeation of a wide range of ionic and non-ionic compounds of molecular weight below 3000 at concentrations exceeding 60% (Ritschel, 1969) and a product containing a 5% solution of the anti-viral agent idoxuridine in DMSO is available for clinical use.
There were various theories as to how it worked, but thirty years ago, the mechanisms were still unclear:
More recent studies suggest that DMSO exerts its role in enhancement of drug permeation by not only extracting soluble components of the horny structure but also by delaminating the horny layer and denaturing the proteins (Kurihara-Bergstrom et al., 1986, 1987).
It has been proposed that part of the effects of DMSO arises from its solvent properties and thus, at high concentrations, it may promote partitioning of lipophilic drugs into the stratum corneum (Barry, 1987).
Results of Fourier transform infrared (FTIR) spectroscopic investigations suggest that DMSO changes stratum corneum protein conformations (Oertel, 1977).
Water displacement may be another part of the mechanisms:
Based on results of recent differential scanning calorimetric studies, it has been suggested that DMSO acts by displacing bound protein water, leaving a looser structure (Barry, 1987).
Despite the wide ranging studies that have been performed with DMSO, its mechanisms of action as a penetration enhancer still remain unclear.
Post-mortem Caucasian abdominal skin was prepared and rehydrated before being exposed to DMSO and analysed for Raman spectra.
From: “Fig. 2. FT Raman spectra of (a) untreated stratum corneum, (b) stratum corneum treated with DMSO-d 6 for 1 h and (c) pure DMSO-d 6. The spectra clearly show the presence of dimethyl sulfoxide in the skin.” Source: https://www.sciencedirect.com/science/article/pii/0378517395001415
They confirmed that α-helical keratin declines and mirrors the conformational change to β-pleated sheets after exposure to DMSO:
From: “Fig. 7. (a}Changes in the Raman signal arising from the amide I mode of α-helical keratin ( ♦ ), the symmetrical parallel mode of anti-parallel /3-pleated sheets (•), the asymmetrical parallel mode of anti-parallel /3-pleated sheets (■) and unidentified protein residues (*), in human stratum corneum with different concentrations of aqueous DMSO. (b)Profile showing amount of α-helical keratin(•) and /β-pleated sheets (0) in human stratum corneum at different concentrations of DMSO, expressed as the percentage of total amount, β-pleated + keratin.” Source: https://www.sciencedirect.com/science/article/pii/0378517395001415
The spectra show effects partly due to the above conformational changes of keratin protein in the stratum corneum, and partly due to changing the structure of intercellular lipids:
Our results show that following extensive lipid extraction, the C-H olefinic stretching mode for stratum corneum at about 3060 cm-1 remained invariant suggesting that it mostly derives from the keratin, while the C-H aliphatic stretching mode at about 2725 cm-1 was entirely removed, indicating it arises essentially from the intercellular lipids.
The band at about 2852 cm-] assigned as a CH2 symmetric stretching mode, is not present in the spectrum of the extracted stratum corneum, suggesting that this band arises mostly fromintercellular lipids.
The band at about 2883 cm -1, assigned as a CH 2 asymmetric stretching mode is markedly reduced in intensity but a fraction of this band remains, indicating that it is mainly due to the intercellular lipids but may have a contribution from the keratin.
The band at about 2931 cm -1 which has been assigned as a CH 3 symmetric stretching mode is however only slightly reduced in intensity suggesting that most of the vibrations responsible for this band arise from the keratin component of the stratum corneum with a minor contribution from the lipids.
Similarly, of the four C-C skeletal stretching modes in the spectrum of stratum corneum, the one found at about 1031 cm -1 remained prominent after lipid extraction, suggesting it is derived from keratin, while the other three at about 1062, 1082 and 1126, cm -1 were markedly reduced, indicating they arise mainly from the intercellular lipid alkyl chains.
Their techniques closely reproduced those obtained from DMSO-treated commercial keratin powder:
All the changes discussed above are summarized in Table 2. The spectrum of the resultant extracted stratum corneum we obtained is in fact markedly similar to the spectrum of commercially available keratin powder (Fig. lb) which we also subjected to extensive solvent extraction to remove lipid contaminants.
Of interest here, a Midwestern Doctor has written about water existing in different states, such as liquid crystalline, and how this is linked to health and disease.
Not an area that allopathic medicine explores:
The changes outlined above suggest that DMSO, in addition to altering the protein conformation, also affects the intercellular lipids in stratum corneum.
The lipids in the stratum corneum are arranged in a multiply bilayered structure. At physiological temperatures and in their unperturbed state, stratum corneum lipids exist in various phases; crystalline, gel and liquid crystalline forms with the gel phase predominating (White et al., 1988).
In the gel phase, lipid backbone C-C bonds are arranged in a zig-zag manner such that the alkyl chains are maximally extended, affording close packing. This is the all-trans structure which has the lowest energy and lateral motion is highly restricted (Lee, 1975).
“… chemical perturbation”i.e. DMSO changes intercellular lipids from the gel phase to the liquid-crystalline phase:
With thermal or chemical perturbation, trans conformers convert to gauche conformers along the alkyl chains. The energy associated with the structure is higher and the carbon atoms are less rigidly held together and thus C-C single bonds along the alkyl chains vibrate with a greater degree of motional freedom.
This increasing mobility along the alkyl chain is associated with a decrease in the microviscosity of the hydrocarbon region of the lipid bilayer. The lipids are thus thought to exist in a more fluid-like state and this is termed the liquid crystalline phase.
Overall, the results from this study show a concentration-dependence in the action of DMSO on stratum corneum lipids and proteins and correlates with data from earlier DSC studies (Barry, 1987).
The displacement of water in the corneocytes is linked to the keratin protein conformational changes:
The nature of DMSO-water binary mixtures has been the subject of many investigations and it is generally agreed that at high concentrations, DMSO breaks up the structure of water.
It is likely that the structural effects of DMSO on water present in biological systems can help explain its various biological properties.
The obvious site for such interactions in the skin is at the polar head group regions of the lipids, and with keratin where water is present. It is worth noting that in the skin, similar shifts were observed in the S--O stretching mode of DMSO as those observed when it was mixed with water.
Results from small angle X-ray scattering (SAXS) studies have shown that the repeat distance between lipid lamellae found in untreated human stratum corneum remained unchanged upon treatment with water, indicating that no swelling between the lipid bilayers occurred and therefore water did not intercalate between the bilayers (Bouwstra et al., 1991).
This implies that water in extensively hydrated skin is mainly associated with the keratin component of the corneocytes. In the native form, the conformational integrity of a protein is dependent upon bound water which forms a hydration sheath.
DMSO may substitute or displace this bound water and in so doing alter the protein conformation as observed in the present study.
This, in itself, does not explain how it also acts as a drug carrier, which is where the lipid phase-state changes offer an explanation:
However, these protein structural changes cannot fully explain the actions of DMSO as at concentrations similar to those at which it is known to enhance drug flux, DMSO was shown to affect stratum corneum lipids and the intercellular domain is presumed to be the main site of the resistance to solute transport for most drugs.
In addition, DMSO may promote the partitioning of lipophilic drugs into the stratum corneum.
In conclusion, therefore, DMSO appears to absorb into the corneocytes whose keratin conformation tends to alter from an a-helix to β-sheets. In the lipid domains, DMSO appears to disturb the multilamellar lipid bilayers by causing conformational changes from an all trans gel phase to a trans-gauche liquid crystalline phase.
The bottom line:
Overall, the action of DMSO on the keratin and lipids thus results in looser or more permeable structures which are presumably responsible at least in part for the observed increases in the flux of very many drugs following DMSO treatment.
Sidebar
Liquid crystalline lipids within hepatic lipid droplets (HLDs) are involved in the development and progression of non-alcoholic fatty liver disease (NAFLD)9, as well as some metabolic disorders, some cancers, and atherosclerosis.
Is it necessarily a good thing that DMSO changes the state of lipids to liquid crystalline? Something to ponder on.
LD: lipid droplets.
CE: cholesteryl ester droplets.
… We show that under normal culture conditions, LDs exhibit the expected morphology of an amorphous emulsion of neutral lipids surrounded by a phospholipid monolayer. However, under conditions of mitotic arrest and nutrient depravation, LDs structurally reorganize into a liquid-crystalline shell surrounding an amorphous core.
By accurate quantification of the shell lattice spacing of 3.4 to 3.6 nm, we could attribute the crystalline phase to CE. These observations are consistent with previous reports in yeast (21).
We further show that the volume ratio of the amorphous core to the crystalline shell falls in the range of 1:2. To further validate this hypothesis, we showed that heat shock treatment of cells with crystalline LDs beyond the phase transition temperature of predominant CE species in cells results in melting of the lattice.
Our experimental conditions, consisting of hours-long mitotic arrest and starvation, led to a homogenously crystalline population of LDs throughout the cell.
… Altogether, these data demonstrate that LDs can exhibit different structural phases that are directly related to cellular conditions and metabolic scenarios and present different modes of interactions with various cellular organelles.
There is a general consensus that cancer cells and immortalized cell cultures display metabolic reprogramming compared with healthy cells (reviewed in refs. 11 and 12). It remains to be validated whether the phase transitions we describe in HeLa cells exist in nontransformed cells.
… CE droplets are also a major component of atherosclerotic lesions in human arteries (18, 34). Intriguingly, Rambold et al. (25) established that LDs in starved fibroblasts can be secreted to the extracellular milieu due to the limited LD storage capacity in cells of nonadipose origin.
Our data raise the possibility that secreted crystalline LDs may directly contribute to the formation of atherosclerotic lesions, in analogy to LDL particles, and may therefore have a direct link to human pathologies.
From: “Liquid-crystalline phase transitions in lipid droplets are related to cellular states and specific organelle association” (2019)
The more I learn, the more I realise how little I know, and how Western allopathic medicine is still in the Stone Age in some respects.
In 2006, Notman et al. published another study into mechanisms, which further improved our understanding: “Molecular Basis for Dimethylsulfoxide (DMSO) Action on Lipid Membranes”10
A walkthrough of this paper alone would fill a Substack, but the reference to cryopreservation is of interest:
Dimethylsulfoxide (DMSO) is an aprotic solvent that has the ability to induce cell fusion and cell differentiation and enhance the permeability of lipid membranes. It is also an effective cryoprotectant.
Insights into how this molecule modulates membrane structure and function would be invaluable toward regulating the above processes and for developing chemical means for enhancing or hindering the absorption of biologically active molecules, in particular into or via the skin.
The enhanced permeability is thought to be due to the induction of tensionless “hourglass-like” water pores in lipid bilayers. They used molecular simulations to support their proposal:
We show here by means of molecular simulations that DMSO can induce water pores in dipalmitoyl-phosphatidylcholine bilayers and propose this to be a possible pathway for the enhancement of penetration of actives through lipid membranes.
DMSO also causes the membrane to become floppier, which would enhance permeability, facilitate membrane fusion, and enable the cell membrane to accommodate osmotic and mechanical stresses during cryopreservation.
The simulations reveal a number of features that are significant in respect to the effects of DMSO on membrane structure and function. Thus DMSO molecules readily partition into the bilayer occupying a position just beneath the lipid headgroups, reduce bilayer thickness, increase headgroup area, markedly reduce both the area compressibility modulus and the bending rigidity of the membrane, and induce water pore formation.
In their simulation, the water pores formed in 0.00000024 seconds!
The remarkable event of the formation of a water pore was observed for the 27 mol % DMSO system after 240 ns (Figure 1). The formation of the pore was initiated by a fluctuation in the bilayer that caused two of the lipid molecules sitting on the opposite sides of the bilayer to get deeper into the bilayer.
Water molecules then started to enter the bilayer (most likely encouraged by the headgroups of these lipids), which were followed by DMSO molecules that in turn facilitated the entry of more water into the bilayer until there was a continuous chain of water.
Reconstruction. I once went to a waterpark like this.
At this point the lipids reoriented to form an hourglasslike pore that rapidly expanded to a size that was stable for the remainder of the simulation.
From: “Figure 1 Water pore formation in a tensionless DPPC bilayer with 27 mol % DMSO after 261.4 ns. Water molecules are shown in cyan, DMSO in brown, DPPC headgroup and glycerol backbone particles in blue, and hydrocarbon particles in light gray.” Source: https://pubs.acs.org/doi/10.1021/ja063363t
Pores can be induced in skin membranes in experiments by applying mechanical stress 16 or an electric field. 17
Pores have also been observed in MD simulations of phospholipid bilayers as transient structures in tensionless bilayers 18 and when the membrane is subjected to either an electric field (electroporation)18 or mechanical stress. 14,19
We propose that the observed DMSO-induced water pore formation could be an important possible mechanism by which DMSO enhances the permeability of membranes.
And from 2020, in “Effect of DMSO on the Mechanical and Structural Properties of Model and Biological Membranes”11, Gironi et al. went a step further and used synthetic liposomes and the plasma membrane of human red blood cells (erythrocytes) to investigate the effects:
In this work, we used two- and three-component synthetic membranes (liposomes) and the plasma membrane of human erythrocytes to investigate the effect of DMSO when added to the membrane-solvating environment.
Fourier transform infrared spectroscopy and thermal fluctuation spectroscopy revealed significant differences in the response of the two types of liposome systems to DMSO in terms of the bilayer thermotropic behavior, available free volume of the bilayer, its excess surface area, and bending elasticity.
DMSO also alters the mechanical properties of the erythrocyte membrane in a concentration-dependent manner and is capable of increasing membrane permeability to ATP at even relatively low concentrations (3% v/v and above).
Taken in its entirety, these results show that DMSO is likely to have a differential effect on heterogeneous biological membranes, depending on their local composition and structure, and could affect membrane-hosted biological functions.
This is a caution against the risk of long-term effects, including when used for blood transfusions:
The membrane is the first barrier that natural and exogenous agents encounter in their initial approach to the cell, and the outcome of their interactions with the membrane could be decisive for the fate of the cell, especially in the case of highly reactive compounds ranging from reactive oxidative species to membrane active peptides and toxins.
Other compounds commonly used in laboratory or clinical practice could also have far-reaching effects on the plasma membrane organization and physical properties (hence, function), and even though their impact may not be dramatically manifested, they could elicit more subtle, but important, membrane responses on different timescales, leading to modulated or impaired membrane function.
A primary example of such a scenario is the modification of the membrane organization and physical properties of stored red blood cells (RBC) (9) and its importance for blood transfusion (10).
It is therefore important to understand and quantify the effects that commonly used exogenous species have on the membrane as a basis for clarifying altered function.
Even in 2020, the mechanisms were unclear:
It would be important to clarify the mechanism by which DMSO could cause ATP release from red cells.
However, transmembrane ATP transport in erythrocytes still remains unclear and a focus of continued debates.
A growing body of evidence suggests that ATP transport across the erythrocyte membrane is regulated. Proteins implicated in the process include members of the family of the erythrocyte membrane ATP binding cassette, also involved in transmembrane ATP transport in other cell types (60).
More recently, a signal transduction pathway for ATP release from red cells has been identified that includes the heterotrimeric Gi protein, adenylyl cyclase, protein kinase A, and the cystic fibrosis transmembrane conductance regulator (CFTR) (for a review, see (61)).
Yet, it is not clear which mechanism is dominant and under which conditions, and how the presence of DMSO might affect it. If we assume that ATP is released from red cells via a regulated transport, DMSO must be interfering with the release pathways.
I will return to this later:
This is plausible because DMSO has been found to alter protein structure and function. For example, DMSO is reported to activate activator protein 1, which consequently stimulates the tumor suppressor protein HLJ1 (64).
Another study found that even a low concentration of DMSO, up to 1.5% v/v, can alter protein secondary structure from α-helical to β-sheet (65). We could therefore hypothesize that DMSO might affect one or more constituents of the ATP transport pathway, thereby facilitating ATP release from the cell.
This is why we need to know:
Whatever the mechanism of DMSO-induced ATP release, these results could be of physiological importance, assuming DMSO also increases membrane permeability to ATP in other cell types.
It is a common practice to use DMSO in relatively large concentrations (10%) as a cryoprotectant, for example for preservation (banking) of umbilical cord blood (67) rich in progenitor and stem cells (68).
A decrease of cell ATP levels caused by DMSO may influence the cell viability and functionality upon thawing because a large number of cell functions and properties are dependent on ATP levels.
Therapeutic studies
Some of these have been described in the opening “Molecule of the Month” article, and others are of particular interest.
In veterinary medicine
It’s always worth checking the vet’s handbooks for an objective guide to drugs that aren’t necessarily also approved for humans.
Key takes from “Plumb’s Veterinary Drug Handbook (7th Edition, 2011)”.
One of the brand names for animal use is “Domoso®”, and Plumb’s guide is quite comprehensive:
“Topical anti-inflammatory analgesic roll-on gel to aid the reduction of acute swelling due to injury in horses and dogs.” Source: https://www.jurox.com.au/product/domoso/
DIMETHYL SULFOXIDE DMSO
(dye-meth-el sul-fox-ide) Domoso®
FREE RADICAL SCAVENGER
Prescriber Highlights
Free radical scavenger that has antiinflammatory, cryopreservative, anti-ischemic, & radioprotective effects
Caution: Mastocytomas, dehydration/shock; may mask existing pathology
Handle cautiously; will be absorbed through skin & can carry toxic compounds across skin
May cause localized “burning” when administered topically
Administer IV to horses slowly & at concentrations of 20% or preferably, less (10%); may occasionally cause diarrhea, tremors, & colic
Odor may be an issue
Uses/Indications
Purported uses for DMSO are rampant, but the only FDA-approved veterinary indication for DMSO is: “… as a topical application to reduce acute swelling due to trauma” (Package Insert; Domoso®—Syntex).
Other possible indications for DMSO include: adjunctive treatment in transient ischemic conditions, CNS trauma and cerebral edema, skin ulcers/wounds/burns, adjunctive therapy in intestinal surgeries, and analgesia for post-operative or intractable pain, amyloidosis in dogs, reduction of mammary engorgement in the nursing bitch, enhancement of antibiotic penetration in mastitis in cattle, and limitation of tissue damage following extravasation injuries secondary to chemotherapeutic agents.
DMSO’s effect on alcohol dehydrogenase, may make it useful in the treatment of ethylene glycol poisoning, but this has not been sufficiently studied as of yet.
DMSO’s attributes as a potential carrier of therapeutic agents across the skin and into the systemic circulation and its synergistic effects with other agents are potentially exciting, but require much more study before they can be routinely recommended.
While the potential indications for DMSO are many, unfortunately, the lack of well-controlled studies leaves many more questions than answers regarding this drug.
Both DMSO and DMS demonstrate antioxidant effects through the reduction of free radicals:
Pharmacology/Actions
The pharmacologic effects of DMSO are diverse. DMSO traps free radical hydroxide and its metabolite, dimethyl sulfide (DMS), traps free radical oxygen. It appears that these actions help to explain some of the antiinflammatory, cryopreservative, antiischemic, and radioprotective qualities of DMSO.
DMSO has weak antibacterial activity when used clinically and possible clinical efficacy when used topically as an antifungal. The mechanism for these antimicrobial effects has not been elucidated.
As an anti-inflammatory, analgesic therapeutic, which has been compared to some narcotic analgesics:
The antiinflammatory/analgesic properties of DMSO have been thoroughly investigated. DMSO appears to be more effective as an antiinflammatory agent when used for acute inflammation versus chronic inflammatory conditions. The analgesic effects of DMSO have been compared to that produced by narcotic analgesics and is efficacious for both acute and chronic musculoskeletal pain.
Conflicting data about its effects on coagulation or heart muscle:
DMSO decreases platelet aggregation but reports of its effects on coagulability have been conflicting, as has its effect on the myocardium.
DMSO has diuretic activity independent of the method of administration.
It provokes histamine release from mast cells, which probably contributes to the local vasodilatory effects seen after topical administration.
It affects some prostaglandins. These are hormone-like, help repair tissue damage, and are responsible for uterine contractions during menstruation:
DMSO also apparently has some anticholinesterase activity and enhances prostaglandin E, but blocksthe synthesis of prostaglandins E2, F2-alpha, H2, and G2.
This is a concern, as we need this enzyme to help protect us from alcohol intoxication:
It inhibits the enzyme alcohol dehydrogenase, which not only is responsible for the metabolism of alcohol, but also the metabolism of ethylene glycol into toxic metabolites.
Pharmacokinetics
DMSO is well absorbed after topical administration, especially at concentrations between 80–100%. It is extensively and rapidly distributed to virtually every area of the body.
Horses metabolize and excrete DMSO much faster than dogs:
After IV administration to horses, the serum half-life was approximately 9 hours. In dogs, the elimination half-life is approximately 1.5 days. DMSO is metabolized to dimethyl sulfide (DMS) and is primarily excreted by the kidneys, although biliary and respiratory excretion also takes place.
In cattle, the drug is eliminated quite rapidly and after 20 days no detectable drug or metabolites are found in milk, urine, blood, or tissues.
The main reason for PPE is so that you don’t unwittingly self-medicate with toxic substances or animal medications.
Worth being wary of if you are asthmatic or suffer from other allergies:
Contraindications/Precautions/Warnings
Wear rubber gloves when applying topically, and apply with clean or sterile cotton to minimize the chances for contaminating with potentially harmful substances. Apply only to clean, dry areas to avoid carrying other chemicals into the systemic circulation.
It may also hide underlying pathologies:
DMSO may mask existing pathology with its antiinflammatory and analgesic activity.
Mastocytoma: an accumulation of mast cells under the skin.
Because DMSO may degranulate mast cells, animals with mastocytomas should only receive DMSO with extreme caution. DMSO should be used cautiously in animals suffering from dehydration or shock as its diuretic and peripheral vasodilatory effects may exacerbate these conditions.
Adverse Effects
When used as labeled, DMSO appears to be anextremely safe drug. Local effects (“burning”, erythema, vesiculation, dry skin, local allergic reactions) and garlic or oyster-like breath odor are the most likely adverse effects. They are transient and quickly resolve when therapy is discontinued.
It may temporarily lead to shortsightedness in dogs and rabbits:
Lenticular changes, which may result in myopia, have been noted primarily in dogs and rabbits when DMSO is used chronically and at high doses. These effects are slowly reversible after the drug is discontinued.
When DMSO is administered intravenously to horses it may cause hemolysis and hemoglobinuria.
They may administer it to horses via IV, but at low doses:
While older dosage references often recommended 20% or less concentrations for IV use in horses, 10% solutions are more commonly recommended today as they are probably safer. Slow administration IV may also reduce adverse effects.
Other adverse effects may includediarrhea, muscle tremorsandcolic.
Liver and kidney damage is a risk:
Reports of hepatotoxicity and renal toxicity have also been reported for various species and dosages. These occur fairly rarely and some clinicians actually believe DMSO has a protective effect on ischemically insulted renal tissue.
There is a risk of teratogenic effects if applied during pregnancy, although it appears to be a high-dose phenomenon:
Reproductive/Nursing Safety
At high doses, DMSO has been shown to be teratogenic in hamsters and chicks, but not mice, rats, or rabbits; weigh the risks versus benefits when using in pregnant animals.
In humans, the FDA categorizes this drug as category C for use during pregnancy (Animal studies have shown an adverse effect on the fetus, but there are no adequate studies in humans; or there are no animal reproduction studies and no adequate studies in humans.).
In a separate system evaluating the safety of drugs in canine and feline pregnancy (Papich 1989), this drug is categorized as in class: C (These drugs may have potential risks. Studies in people or laboratory animals have uncovered risks, and these drugs should be used cautiously as a last resort when the benefit of therapy clearly outweighs the risks.)
As it’s dipolar and has a half-life of several days, I would at least expect its metabolites to be detected in milk:
It is not known whether this drug is excreted in milk; use in nursing dams with caution.
It would be relatively easy to OD the animal by IV:
Overdosage/Acute Toxicity
The reported LD50’s following IV dosage in dogs and cats are: Cats ≈ 4 g/kg, and Dogs ≈ 2.5 g/kg. Signs of toxicity include: sedation and hematuria at non-lethal doses; coma, seizures, opisthotonus, dyspnea and pulmonary edema at higher dosages. Should an acute overdosage be encountered, treat supportively.
Anticholinesterases: These help to block the breakdown of the neurotransmitter acetylcholine (ACh), leading to toxicity in humans through nerve stimulation. Some chemical warfare agents exploit their effects12.
Drug Interactions
The following drug interactions have either been reported or are theoretical in humans or animals receiving DMSO and may be of significance in veterinary patients:
Because of its anticholinesterase activity, avoid the use of organophosphates or other cholinesterase inhibitors with DMSO.
Unintentional mercury poisoning:
A fatality secondary to mercury intoxication was reported when DMSO was mixed with a mercury salt “red blister” and applied topically to the leg of a horse.
Because it inhibits alcohol dehydrogenase, DMSO may prolong the effects ofalcohol.
Increased risk of OD of various drugs:
Insulin, corticosteroids, (including endogenous steroids), and atropine may be potentiated by DMSO.
The FDA (them again) posted criminally negligent advice about Ivermectin, but it is the reason I will skip the section on veterinary dosing advice.
However, the following advice applies equally to us humans:
Client Information
Do not use non-medical grades of DMSO as they may contain harmful impurities.
N.B. Vinyl gloves?
Wear rubber gloves when applying topically. DMSO should be applied with clean or sterile cotton to minimize the chances for contaminating with potentially harmful substances.
Apply only to clean, dry skin. Use in well-ventilated area; avoid inhalation and contact with eyes. May damage some fabrics. Keep lid tightly on container when not in use. Keep out of reach of children. Do not mix with any other substance without veterinarian’s approval.
Selected DMSO products are FDA-approved for use in dogs and in horses not intended for food purposes. It is a veterinary prescription (Rx) drug.
Storage/Stability
Must be stored in airtight containersaway from light. As DMSO may react with some plastics, it should be stored in glass or in the container provided by the manufacturer. If DMSO is allowed to contact room air it will self-dilute to a concentration of 66–67%.
Advice is to be extremely careful if compounding with other meds:
Compatibility/Compounding Considerations
DMSO is apparently compatible with many compounds, but because of the chances for accidental percutaneous absorption of potentially toxic compounds, the admixing of DMSO with other compounds is not to be done casually.
This is a relatively low dose, and for the only approved human treatment: interstitial cystitis:
Moving on to other PubMed studies for further reading:
For cardiac / CNS damage
Pharmacology of dimethyl sulfoxide in cardiac and CNS damage (2009)
Abstract
The pharmacological effects of dimethyl sulfoxide (DMSO) administration include some desirable properties that may be useful in the treatment of medical disorders resulting in tissue injury and compromised organ systems. These properties include the reported effects of DMSO on impaired blood flow, suppression of cytotoxicity from excess glutamate release that may result in lethal NMDA-AMPA activation, restriction of cytotoxic Na(+) and Ca(2+) entry into damaged cells, blocking tissue factor (TF) from contributing to thrombosis, reduction of intracranial pressure, tissue edema, and inflammatory reactions, and inhibition of vascular smooth muscle cell migration and proliferation that can lead to atherosclerosis of the coronary, peripheral, and cerebral circulation. A review of the basic and clinical literature on the biological actions of DMSO in cardiac and central nervous system (CNS) damage or dysfunction indicates that this agent, alone or in combination with other synergistic molecules, has been reported to neutralize or attenuate pathological complications that harmed or can further harm these two organ systems. The effects of DMSO make it potentially useful in the treatment of medical disorders involving head and spinal cord injury, stroke, memory dysfunction, and ischemic heart disease.
Effect of Local and Systemic Dimethylsulfoxide on Peripheral Nerve Repair: A Controlled Randomized Experimental Study (2021)
Abstract
We investigated the possible beneficial effect of dimethylsulfoxide (DMSO) on peripheral nerve repair in rats.
Methods:
Seventy rats were divided into four groups: control, sham, DMSO-L, and DMSO-IP. Except in the control group, nerve repair was done at the right sciatic nerve. DMSO was administered locally and intraperitoneally for 12 weeks to the DMSO-L and DMSO-IP groups, respectively. No therapeutic agent was administered to the other groups. Nerve regeneration was assessed by behavioral, electrophysiological, histopathological, and immunohistochemical tests.
Results:
With the exception of S-100 protein expression, all results indicate that DMSO has a beneficial effect on peripheral nerve regeneration. Functional nerve recovery was notably more evident in the DMSO-L than in the DMSO-IP group. Under macroscopic examination, nerve scores of the regeneration area in the DMSO-L group was also better than in the others.
Discussion: We believe that DMSO can improve peripheral nerve regeneration in rats.
Dimethylsulfoxide (DMSO) blocks conduction in peripheral nerve C fibers: a possible mechanism of analgesia (1993)
Abstract
Dimethylsulfoxide (DMSO) is readily absorbed through skin, and relieves musculoskeletal pain when applied topically to painful areas. We studied the effects of DMSO on C-type nerve fibers, which mediate pain sensation. DMSO was applied directly to exposed cat sural nerves. C fiber conduction velocity was slowed by DMSO, even in low concentrations (5-7% v/v). Higher concentrations completely blocked C fiber conduction, with a minimum blocking concentration of 9%. Onset of nerve block was almost immediate with 15% DMSO or higher concentrations. C fiber blockade may account for analgesia with DMSO.
There is a concern here because a 2019 study found that 1% DMSO may be cytotoxic to oligodendrocytes. These are the glial cells responsible for producing the myelin sheath. Demyelination in MS hinders nerve transmission and leads to a range of symptoms.
Dimethylsulfoxide Inhibits Oligodendrocyte Fate Choice of Adult Neural Stem and Progenitor Cells (2019)
Abstract
Several clinical trials address demyelinating diseases via transplantation of mesenchymal stromal cells (MSCs). Published reports detail that administration of MSCs in patients may provide a beneficial immunomodulation, and that factors secreted by MSCs are potent inducers of oligodendrogenesis. Dimethylsulfoxide (DMSO) is widely used in life science and medicine as solvent, vehicle or cryoprotectant for cells used in transplantation. Importantly, most transplantation protocols do not include the removal of DMSO before injecting the cell suspension into patients. This indifferent application of DMSO is coming under increasing scrutiny following reports investigating its potential toxic side-effects. While the impact of DMSO on the central nervous system (CNS) has been partially studied, its effect on oligodendrocytes and oligodendrogenesis has not been addressed yet. Consequently, we evaluated the influence of DMSO on oligodendrogenesis, and on the pro-oligodendrogenic effect of MSCs’ secreted factors, using adult rat neural stem and progenitor cells (NSPCs). Here, we demonstrate that a concentration of 1% DMSO robustly suppressed oligodendrogenesis and drove the fate of differentiating NSPCs toward astrogenesis. Furthermore, the pro-oligodendrogenic effect of MSC-conditioned medium (MSCCM) was also nearly completely abolished by the presence of 1% DMSO. In this condition, inhibition of the Erk1/2 signal transduction pathway and high levels of Id2 expression, a specific inhibitor of oligodendrogenic differentiation, were detected. Furthermore, inflammatory demyelinating diseases may even potentiate the impact of DMSO on oligodendrogenesis. Our results demonstrate the imperative of considering the strong anti-oligodendrogenic activity of DMSO when designing future clinical trial protocols.
… In young adults, the most common neurological disease leading to permanent disability is multiple sclerosis (MS). The latter is a neuroinflammatory disorder of the central nervous system (CNS) characterized by the progressive destruction of myelin sheaths. Although MS patients can recover from their first demyelinating episodes through a process known as remyelination, the regenerative capacity of the CNS declines through the course of the disease.
MSC-conditioned medium (MSCCM) should promote oligodendrogenesis, but is inhibited by 1% DMSO. Less astroglial fate determinant Id2 is better:
… The transcription factors Olig2 (oligodendroglial lineage) and Id2 (astroglial lineage) are key determinants of NSPC’s glial lineage commitment (Samanta and Kessler, 2004; Steffenhagen et al., 2012).
… The expression levels of Olig2 did not differ significantly throughout the conditions. Hence, these results suggest that DMSO mainly impacted differentiation through an increase of the expression of the astroglial fate determinant Id2, thereby inhibiting oligodendroglial fate decision in NSPCs.
From: “FIGURE 3. Expression of glial fate determinants after treatment with 1% DMSO. RT-PCRs of pro-oligodendrogenic Olig2 and pro-astrocytic Id2 gene expression were performed on NSPCs differentiating for 3 days. (A) Relative levels of mRNA expression for Id2 (red) and Olig2 (green) detected in NSPCs cultivated in aMEM or MSCCM, with or without 1% DMSO. (B) Ratio of Olig2/Id2. Data are shown as mean ± SD. Asterisks mark significant difference compared to aMEM, ∗p < 0.05.” Source: https://pmc.ncbi.nlm.nih.gov/articles/PMC6901908/
DMSO Represses Inflammatory Cytokine Production from Human Blood Cells and Reduces Autoimmune Arthritis (2016)
Herein, we demonstrate that DMSO has ex-vivo anti-inflammatory activity using Escherichia coli- (E. coli) and herpes simplex virus-1 (HSV-1)-stimulated whole human blood. Specifically, we found that between 0.5%-2%, DMSO significantly suppressed the expression of many pro-inflammatory cytokines/chemokines and prostaglandin E2 (PGE2). However, a significant reduction in monocyte viability was also observed at 2% DMSO, suggesting a narrow window of efficacy. Anti-inflammatory concentrations of DMSO suppressed E. coli-induced ERK1/2, p38, JNK and Akt phosphorylation, suggesting DMSO acts on these signaling pathways to suppress inflammatory cytokine/chemokine production. Although DMSO induces the differentiation of B16/F10 melanoma cells in vitro, topical administration of DMSO to mice subcutaneously implanted with B16 melanoma cells was ineffective at reducing tumor growth, DMSO was also found to block mouse macrophages from polarizing to either an M1- or an M2-phenotype, which may contribute to its inability to slow tumor growth. Topical administration of DMSO, however, significantly mitigated K/BxN serum-induced arthritis in mice, and this was associated with reduced levels of pro-inflammatory cytokines in the joints and white blood cell levels in the blood. Thus, while we cannot confirm the efficacy of DMSO as an anti-cancer agent, the use of DMSO in arthritis warrants further investigation to ascertain its therapeutic potential.
The importance of using a very low dose when treating rheumatoid arthritis:
Dimethyl Sulfoxide: A Bio-Friendly or Bio-Hazard Chemical? The Effect of DMSO in Human Fibroblast-like Synoviocytes (2022)
Abstract
The effect of dimethyl sulfoxide (DMSO) in rheumatoid arthritis (RA) human fibroblast-like synoviocytes (FLSs) has been studied on five different samples harvested from the joints (fingers, hands and pelvis) of five women with RA. At high concentrations (>5%), the presence of DMSO induces the cleavage of caspase-3 and PARP-1, two phenomena associated with the cell death mechanism. Even at a 0.5% concentration of DMSO, MTT assays show a strong toxicity after 24 h exposure (≈25% cell death). Therefore, to ensure a minimum impact of DMSO on RA FLSs, our study shows that the concentration of DMSO has to be below 0.05% to be considered safe.
In the light of this, overdosing very likely explains why these experiments failed:
Dimethyl sulfoxide does not suppress an experimental model of arthritis in rabbits (1983)
Abstract
We studied the ability of dimethyl sulfoxide (DMSO) to influence the course of an experimental model of inflammatory arthritis. A Dumonde-Glynn model of arthritis was induced in both tibio-femoral joints of 10 rabbits, using ovalbumin as the immunogen. At one month post induction of the arthritis, the right tibio-femoral joint of 6 animals was treated for 3 months with topical 80% DMSO--1 g/kg body weight applied to the shaved skin for 5 out of 7 days each week. In another 4 animals, the right tibio-femoral joint was injected with 0.5 ml of 80% DMSO at one month post induction of the arthritis. Joint radiographs were taken at monthly intervals. The rabbits were sequentially sacrificed and the joint tissues evaluated by a blinded observer. Neither the topical DMSO nor the intraarticular DMSO treated joints showed any favorable responses to therapy; in fact the topically treated joints exhibited somewhat more inflammatory and destructive changes than the untreated joints. However the repeated injection of DMSO into normal joints did not, of itself, produce any deleterious effects. This study indicates a need to assess more thoroughly a possible deleterious effect of DMSO on the course of untreated inflammatory arthritis.
Even at relatively low doses, DMSO may destroy the cartilage in your joints. You may not be aware of this, though, due to its painkilling effects.
Effect of dimethylsulfoxide on articular cartilage proteoglycan synthesis and degradation, chondrocyte viability, and matrix water content (1998)
Objective: To determine the effects of dimethylsulfoxide (DMSO) exposure on cartilage proteoglycan (PG) synthesis, PG degradation, chondrocyte viability, and matrix water content.
Study design: Using a cartilage explant culture system, PG synthesis, PG degradation, matrix water content, and chondrocyte viability were determined for cartilage exposed to DMSO daily for selected periods of time.
Methods: PG synthesis: Explants (n = 30/group) were separated into 10 groups based on the time of daily exposure to 10% DMSO. Exposure time was repeated daily for 3 days. The control group was incubated in basal medium alone for 3 days, with daily medium changes. Once all DMSO exposure times were complete for the third day, PG synthesis was determined by analysis of incorporation of radiolabelled sulfate.
… Results: PG synthesis was significantly lower than control for all time periods of DMSO exposure except for 1 and 3 hours, and decreased in a time-dependent manner after the 1-hour exposure time. The mean percentage of viable cells/hpf was significantly lower than control for the 1-, 3-, 9-, 12-, and 24-hour treatment groups. There was no significant difference in PG degradation for any group compared with control for the first 2 days of incubation. All groups except the 24-hour group had a significantly higher degradation compared with control for the third day of incubation. Cartilage exposed to DMSO for 72 hours had a significantly lower water content, and cartilage incubated in basal medium alone for 72 hours had a significantly higher water content than cartilage that received no DMSO and no incubation.
Conclusions: DMSO, in relatively low concentration, is detrimental to articular cartilage PG synthesis in a time-dependent manner. Dehydration of the cartilage and chondrocyte death also occur with increasing time of DMSO exposure. Significant PG degradation occurs on the third day of culture with daily DMSO exposure.
Clinical relevance: As a joint lavage solution, DMSO has potentially deleterious effects on the metabolism of chondrocytes.
Efficacy and safety of topical diclofenac containing dimethyl sulfoxide (DMSO) compared with those of topical placebo, DMSO vehicle and oral diclofenac for knee osteoarthritis (2009)
Abstract
While topical non-steroidal anti-inflammatory drugs are considered safe, their long-term efficacy for osteoarthritis has been suspect. We conducted a 12-week, double-blind, double-dummy, randomized controlled trial of topical diclofenac (TDiclo) in a vehicle solution containing dimethyl sulfoxide (DMSO) in 775 subjects with radiologically confirmed, symptomatic primary osteoarthritis of the knee. This 5-arm study compared TDiclo with a placebo solution, the DMSO vehicle, oral diclofenac (ODiclo) and the combination of TDiclo+ODiclo for relieving the signs and symptoms of knee osteoarthritis. Subjects applied study solution, 40 drops four times daily, and took one study tablet daily for 12 weeks. Co-primary efficacy variables were WOMAC pain and physical function and a patient overall health assessment. Secondary variables were WOMAC stiffness and patient global assessment (PGA) of the knee osteoarthritis. TDiclo was superior to placebo for pain (-6.0 vs. -4.7, P=0.015), physical function (-15.8 vs. -12.3, P=0.034), overall health (-0.95 vs. -0.37, P<0.0001), and PGA (-1.36 vs. -1.01, P=0.016), and was superior to DMSO vehicle for all efficacy variables. No significant difference was observed between DMSO vehicle and placebo or between TDiclo and ODiclo. The commonest adverse event associated with TDiclo was dry skin (18.2%). Fewer digestive system and laboratory abnormalities were observed with TDiclo than with ODiclo. Addition of TDiclo to ODiclo did not increase the incidence of systemic adverse events. TDiclo in DMSO vehicle is an effective treatment option for knee osteoarthritis with efficacy similar to, but tolerability better than ODiclo. DMSO vehicle was no more efficacious than placebo.
This has implications for treating stroke victims, too:
Antioxidant-based neuroprotective effect of dimethylsulfoxide against induced traumatic brain injury in a rats model (2022)
Traumatic brain injury (TBI) has been the result of neurological deficit and oxidative stress. This study evaluated the antioxidative neuroprotective property and learning and memory-enhancing effects of dimethyl sulfoxide (DMSO) in a rat model after the induction of TBI.
… Group I was induced with TBI and treated with DMSO at 67.5 mg/kg orally once daily which started 30 min after the induction of TBI and lasted 21 days. Group II was induced with TBI but not treated while Group III was neither induced with TBI nor treated.
… Administration of DMSO to rats with induced TBI has improved learning and memory, locomotor function and decreased anxiety in Group I compared to Group II. Moreover, the level of S100B was significantly (p < 0.05) lower in Group I compared to Group II. Treatment with DMSO also decreased lipid peroxidation significantly (p < 0.05) compared to Group II. There exists a significant (p < 0.05) increase in CAT, SOD, and GPX activities in Group I compared to Group II. Therefore, DMSO has demonstrated a potential antioxidative neuroprotective effect through its ability to increase the level of antioxidant enzymes which they quench and inhibit the formation of ROS, thereby improving cognitive functions.
DMSO inhibits human platelet activation through cyclooxygenase-1 inhibition. A novel agent for drug eluting stents? (2009)
Abstract
Background: DMSO is routinely infused together with hematopoietic cells in patients undergoing myeloablative therapy and was recently found to inhibit smooth muscle cells proliferation and arterial thrombus formation in the mouse by preventing tissue factor (TF), a key activator of the coagulation cascade. This study was designed to investigate whether DMSO prevents platelet activation and thus, whether it may represent an interesting agent to be used on drug eluting stents.
Methods and results: Human venous blood from healthy volunteers was collected in citrated tubes and platelet activation was studied by cone and platelet analyzer (CPA) and rapid-platelet-function-assay (RPFA). CPA analysis showed that DMSO-treated platelets exhibit a lower adherence in response to shear stress (-15.54+/-0.9427%, n=5, P<0.0001 versus control). Additionally, aggregometry studies revealed that DMSO-treated, arachidonate-stimulated platelets had an increased lag phase (18.0%+/-4.031, n=9, P=0.0004 versus control) as well as a decreased maximal aggregation (-6.388+/-2.212%, n=6, P=0.0162 versus control). Inhibitory action of DMSO could be rescued by exogenous thromboxane A2 and was mediated, at least in part, by COX-1 inhibition.
Conclusions: Clinically relevant concentrations of DMSO impair platelet activation by a thromboxane A2-dependent, COX-1-mediated effect. This finding may be crucial for the previously reported anti-thrombotic property displayed by DMSO. Our findings support a role for DMSO as a novel drug to prevent not only proliferation, but also thrombotic complications of drug eluting stents.
For treating strokes (cerebrovascular accidents, CVA)
Effects of intravenous dimethyl sulfoxide on ischemia evolution in a rat permanent occlusion model (2010)
Abstract
Dimethyl sulfoxide (DMSO) has a variety of biological actions that suggest efficacy as a neuroprotectant. We (1) tested the neuroprotective potential of DMSO at different time windows on infarct size using 2,3,5-triphenyltetrazolium staining and (2) investigated the effects of DMSO on ischemia evolution using quantitative diffusion and perfusion imaging in a permanent middle cerebral artery occlusion (MCAO) model in rats. In experiment 1, DMSO treatment (1.5 g/kg intravenously over 3 h) reduced infarct volume 24 h after MCAO by 65% (P<0.00001) when initiated 20 h before MCAO, by 44% (P=0.0006) when initiated 1 h after MCAO, and by 17% (P=0.11) when started 2 h after MCAO. Significant infarct reduction was also observed after a 3-day survival in animals treated 1 h after MCAO (P=0.005). In experiment 2, treatment was initiated 1 h after MCAO and maps for cerebral blood flow (CBF) and apparent diffusion coefficient (ADC) were acquired before treatment and then every 30 mins up to 4 h. Cerebral blood flow characteristics and CBF-derived lesion volumes did not differ between treated and untreated animals, whereas the ADC-derived lesion volume essentially stopped progressing during DMSO treatment, resulting in a persistent diffusion/perfusion mismatch. This effect was mainly observed in the cortex. Our data suggest that DMSO represents an interesting candidate for acute stroke treatment.
This study (paywalled) found that 1% DMSO increased the permeability of the blood-brain barrier in rats. This is potentially useful for conveying therapeutics, eg to treat fluid buildup in the brain:
Effect of dimethyl sulfoxide on blood-brain barrier integrity following middle cerebral artery occlusion in the rat (2006)
Abstract
Dimethyl sulfoxide (DMSO) is widely used as a solvent for other drugs, i.e., for the protein kinase C activator phorbol 12-myristate 13-acetate (PMA) and the V1a receptor-antagonist SR49059, to reduce brain edema. We studied the effect of DMSO on blood-brain barrier (BBB) integrity following middle cerebral artery occlusion (MCAO) and the consequences on brain edema development. Male Sprague-Dawley rats were randomly assigned to sham procedure or infusion of 1% DMSO, PMA (230 microg/kg in 1% DMSO), or SR49059 (1 mg/kg in 1% DMSO) followed by MCAO (each group n = 10). After a 2-hour period of ischemia and 2 hours reperfusion, the animals were sacrificed for assessment of brain water content, sodium, and potassium concentration. BBB integrity was assessed by Evans blue extravasation. Statistical analysis was performed by ANOVA followed by a Tukey post hoc test. Low-dose DMSO treatment following MCAO significantly opened the BBB on the ischemic side (p < 0.037). PMA and SR49059 did not have any additional effect on BBB compromise compared to DMSO (p = 1.000, p < 0.957, respectively). We conclude that DMSO as a vehicle for drug administration may increase the drug concentration into the extracellular space, but since BBB permeability is increased, it may also provide an avenue for development of vasogenic edema.
This property has been known for at least forty-three years:
(Paywalled)
Morphologic effect of dimethyl sulfoxide on the blood-brain barrier (1982)
Abstract
Dimethyl sulfoxide (DMSO) opens the blood-brain barrier of mice to the enzymatic tracer horseradish peroxidase. A single injection of horseradish peroxidase in 10 to 15 percent DMSO into the tail vein along with 10 to 15 percent DMSO delivered intraperitoneally allowed horseradish peroxidase to fill the extracellular clefts throughout the brain within 2 hours. In the absence of DMSO, peroxidase failed to enter brain parenchyma except through the circumventricular organs. Opening of the blood-brain barrier by DMSO is reversible. Dimethyl sulfoxide stimulated the pinocytosis of horseradish peroxidase by the cerebral endothelium; the peroxidase was then directed to lysosomal dense bodies for degradation. Vesicular transport of horseradish peroxidase from the luminal to the abluminal wall of the endothelial cell was not observed. Dimethyl sulfoxide did not alter the morphology of endothelial cells or brain parenchyma.
Hypoalbuminemia: When your body produces insufficient albumin protein, and levels in the blood are too low. Albumin makes up to 50% of the proteins found in plasma. A deficiency means that hormones and other compounds may not be transported to where they need to be. This may lead to malnutrition, liver disease, kidney disease or heart failure, and circulatory collapse.
From burns, hypoalbuminemia is associated with fluid build-up (oedema) and sepsis.
The role of dimethyl sulfoxide (DMSO) in ex-vivo examination of human skin burn injury treatment (2018)
Abstract
… Thermal injury is associated with the appearance of lipid peroxidation products in the burned skin. The influence of DMSO on protein structure and stability is concentration and temperature dependant. The aim of this study was to assess the impact of DMSO on human burn wounds and examine the interactions between DMSO and skin surface. The real problem in burn treatment is hypoalbuminemia. At the level of the laboratory studies there was an attempt at answering the question of whether the DMSO will modify the standard serum solution. In the case of the incubation of skin fragments in 1%-100% DMSO, the following findings were reported: modification of the serum, appearance of low molecular weight oligomer bands, disappearance of albumin bands or reconstruction of native serum bands during incubation in antioxidant solutions. The result of the modification is also the exposure of FTIR 1603 and 1046cm-1 bands observed in frozen serum solutions. In the case of modification of the burned skin by DMSO solutions or antioxidants - frequency shifts, an increase in the intensity of amide I band as well as the appearance of the 1601cm-1 band can be specific biomarkers of the tissue regeneration process. In this study the areas 1780-1580cm-1 and 1418-1250cm-1 on the Raman spectra are particularly rich in spectral information.
… it appears that DMSO accelerates fixation, enhances stabilization of cellular ultrastructure via its interaction with remnant interfacial water in fixed cells [8]. Lipid fusogens could induce a conformational change in the bilayer-forming lipids at physiological and probably also at pathological temperatures (for example in burn skin). A destabilization of phospholipid membranes at higher temperatures due to a hydrophobic association between DMSO and the bilayer [9]. DMSO can reduce the temperature of transition from the lamellar to non-lamellar phase in the membrane lipid bilayer matrix [1]. DMSO increase membrane fluidity thereby altering the transport functions and permeability properties of the membrane.
… In this study the environment of burn human skin modifiers was changed by adding 80% and 1% DMSO. It appears that DMSO accelerates fixation, enhances stabilization of cellular ultrastructure via its interaction with remnant interfacial water in fixed cells.
… 4. Discussion
DMSO is one of the most versatile solvents in biological science. DMSO changes the scope of penetration of chemical compounds in biological membranes, including human skin, affecting the nature of interactions in protein-lipid membranes.
… From a clinical point of view, the real problem in burn treatment is hypoalbuminemia. Hypoalbuminemia is a common clinical deficiency in burn patients and is associated with complications related to increased extravascular fluid, including edema, abnormal healing, and susceptibility to sepsis [[18], [19], [20]]. Burns affecting >20% of the body surface cause a major loss of extracellular fluids, thereby inducing shock by increasing vascular permeability and reducing plasma albumin from the wound exudations. It is known that DMSO is cell fusogen and a permeability enhancing agent. DMSO has been used successfully to induce fusion between cells or liposomes. The effect in this case has been explained as an occlusion of water movement through membrane protein pores by DMSO [1]. Thus, it appears that DMSO accelerates fixation, enhances stabilization of cellular ultrastructure via its interaction with remnant interfacial water in fixed cells [8]. It seems that the easily penetrating DMSO solution applied on the skin may block the loss of body fluids from the burn wound causing a natural sealing of the wound. Analyzing the photographsFig. 10a, b, c, this effect can be expected. Selection of optimal concentrations of DMSO requires further research.
From: “Fig. 10. Scanning electron microscopy images of the surfaces of: (a) human burn wound in presence of 10% DMSO (BS 10DMSO); (b) human burn wound in presence of 10% DMSO (BS 10DMSO); (c) human burn wound in presence of 80% DMSO (BS 80DMSO); (d) allogeneic undamaged human skin samples (SP).” Source: https://pubmed.ncbi.nlm.nih.gov/29475183
DMSO stimulated healing by promoting cell proliferation via the Akt/mTOR signalling pathway.
Note that dysfunction in components of this pathway helps to promote cancer progression and resistance to treatments13.
In other words, you only want to promote cell proliferation to help heal an injury, not in otherwise healthy tissues.
Low‐concentration DMSO accelerates skin wound healing by Akt/mTOR‐mediated cell proliferation and migration in diabetic mice (2020)
Abstract
Background and Purpose
DMSO has been found to promote tissue repair. However, the role of DMSO in diabetic skin wound healing and the underlying molecular mechanisms are still unclear.
Experimental Approach
The effects of DMSO on wound healing were evaluated by HE staining, immunohistochemistry and collagen staining using a wound model of full‐thickness skin resection on the backs of non‐diabetic or diabetic mice. Real‐time cell analysis and 5‐ethynyl‐2′‐deoxyuridine incorporation assays were used to study the effect of DMSO on primary fibroblast proliferation. A transwell assay was used to investigate keratinocyte migration. The associated signalling pathway was identified by western blotting and inhibitor blocking. The effect of DMSO on the translation rate of downstream target genes was studied by RT‐qPCR of polyribosome mRNA.
Key Results
We found that low‐concentration DMSO significantly accelerated skin wound closure by promoting fibroblast proliferation in both nondiabetic and diabetic mice. In addition, increased migration of keratinocytes may also contribute to accelerated wound healing, which was stimulated by increased TGF‐β1 secretion from fibroblasts. Furthermore, we demonstrated that this effect of DMSO depends on Akt/mTOR‐mediated translational control and the promotion of the translation of a set of cell proliferation‐related genes. As expected, DMSO‐induced wound healing and cell proliferation were impaired by rapamycin, an inhibitor of Akt/mTOR signalling.
Conclusion and Implications
DMSO can promote skin wound healing in diabetic mice by activating the Akt/mTOR pathway. Low‐concentration DMSO presents an alternative medication for chronic cutaneous wounds, especially for diabetic patients.
… These results demonstrate that DMSO improved wound healing by activating mTORC1 but not mTORC2. Together, these results suggested that activation of Akt/mTORC1 is necessary for DMSO-induced cell proliferation and translational activation in diabetic primary skin fibroblasts and is thus vital in DMSO-promoted skin wound healing.
… In summary, DMSO promotes the healing of refractory diabetic wounds by activating the Akt/mTORC1 signalling pathway, leading to enhanced cap-dependent translation of proliferation-related genes, accelerated fibroblast proliferation and keratinocyte migration and increased extracellular matrix secretion, ultimately promoting diabetic wound healing (Figure 7). Thus, our findings provide a theoretical basis for the further development of DMSO as a pro-healing drug for refractory wounds and highlight the regulatory role of Akt/mTOR signalling in the healing of refractory diabetic wounds. These results also warrant caution when using DMSO as a solvent in future pharmacological studies.
From “FIGURE 7. Schematic of the pharmacological mechanism of DMSO. DMSO has a profound effect on fibroblast proliferation via Akt/mTOR-mediated protein translation, which activates both collagen production and TGF-β1 secretion. The active fibroblast TGF-β1 induces EMT signalling in keratinocytes, promoting EMT-like transdifferentiation and keratinocyte migration. EMT, epithelial–mesenchymal transition.” Source: https://bpspubs.onlinelibrary.wiley.com/doi/10.1111/bph.15052
Keep Cool but Don’t Freeze: The Influence of William J. Mills Jr. on the Treatment of Frostbite (2024)
Abstract
Dr William J. Mills Jr., an Alaskan orthopedic surgeon, helped establish the current protocols for frostbite treatment and changed a dogma used for more than 140 years that was established by Napoleon's surgeon general of the army, Baron Dominique-Jean Larrey. During Napoleon's 1812 siege of Moscow, Larrey noticed the destructive effects of using open fire heat for warming frozen body parts, so he suggested rubbing snow or immersion in cold water. Dr Mills treated many cold injuries during his medical career. After setting up his medical practice in Anchorage, Alaska, he realized the inefficiency of the established protocols and started researching new treatments for frostbite. Dr Mills followed Meryman's method of rapidly thawing frozen red blood cells in warm water. Mills and his colleagues established a treatment protocol for freezing cold injury that included rapid warming in warm water. These studies resulted in the publication of three key papers in 1960 and 1961. These papers were the first clinical studies that described rapid warming as a treatment. Subsequently, rapid warming, with some variation in water temperatures, has been accepted as the standard of treatment. Due to his outstanding contribution to the treatment of frostbite, he has been referred to as “the nation's leading authority on cold injury.”
… Mills studied vasodilating agents (tolazoline hydrochloride); anticoagulants (heparin), vasodilators (priscoline), hypotensive adrenergic blocking agents (guanethidine, reserpine), sympatholytic drugs (dibenzyline), hemorheological agents (oxpentifylline); calcium blocking agents (nifedipine); sympatholytic agents (phenoxybenzamine hydrochloride); and dimethyl sulfoxide (DMSO). He also proposed that the use of thrombolytic enzymes (streptokinase, urokinase) for deep thrombosis should be evaluated. He explained, “The risk of hemorrhage and lysis of fresh fibrin may limit the use of these drugs with associated trauma, especially in head trauma where the cerebral vascular bleed may be of concern.”He suggested that the administration of these drugs needed special considerations.18
A Combination of Synthetic Molecules Acts as Antifreeze for the Protection of Skin against Cold-Induced Injuries (2021)
Abstract
Seasonal and occupational exposure of the human body to extreme cold temperatures can result in cell death in the exposed area due to the formation of ice crystals. This leads to superficial or deep burn injury and compromised functionality. Currently available therapeutics can be ineffective in extreme cases, and thus, it is necessary to develop prophylactic strategies. In this study, we have devised a combination of known synthetic cryopreservative agents (termed SynAFP) and evaluated their potential antifreeze applications on skin. The prophylactic activity of SynAFP in vitro is indicated by improved cellular revival and cell viability, retention of the cytoskeleton, and normal cell cycle progression even after cold stress. A comprehensive whole-cell proteomic approach revealed that in the presence of SynAFP, cold-induced downregulation of proteins involved in cell–cell adhesion and upregulation of those related to mitochondrial stress were ameliorated. Pre-application of SynAFP in mice facing a frostbite challenge prevents their skin from incurring significant injury as confirmed through macroscopic and histological examination. Moreover, multiple applications of SynAFP on mouse skin at room temperature did not compromise skin integrity. SynAFP was also formulated in an Aloe vera-based cream (referred to as fSynAFP), which offered similar protection under cold stress conditions. Thus, SynAFP can be considered as a potential candidate for formulating a topical intervention for protection from cold-induced injuries to skin.
… In this study, we describe a combination of synthetic chemicals, dimethyl sulfoxide (DMSO) and poly(vinyl alcohol) (PVA), which can be pre-applied to skin cells and tissue to provide protection from cold-induced injuries. DMSO is an aprotic organic solvent that is widely used for cryopreservation of biological materials through a process called vitrification. (22) Devitrification upon warming leads to ice recrystallization and causes toxicity because of the very high DMSO concentrations used in the process (5 to 20 wt %). Therefore, DMSO is not suitable to be used alone for the prevention of cold-induced injuries. (23) On the other hand, 9 kDa PVA has been shown to exhibit excellent biocompatibility at concentrations as low as 10 mg/mL and confer high post-thaw recovery in sheep and human RBCs when supplemented with a low concentration of hydroxyethyl starch (HES). (24) We have identified the optimal combination of these chemicals, which can provide protection to mammalian skin cells and tissue from cold-induced injury without any toxic effects at physiological temperatures. We conjecture that this method can be extended to generate formulations for the prevention of cold-induced injuries in a convenient, non-invasive, and safe manner.
… In general, our data indicates a possible antifreeze action of SynAFP. We speculate that the synergistic effect of the principal components of SynAFP, DMSO, and PVA might be attributed to the mechanism of action of the two. DMSO, a known cryopreservative, can easily penetrate cells without any evidence of cellular injury (59−61) and protect them from freezing damage by a plethora of mechanisms. It can enhance cell membrane permeability and make it floppier to facilitate membrane fusion, thus enabling the cell to withstand osmotic and mechanical stresses that develop during freezing protocols. (60) Moreover, the ability of DMSO to form strong hydrogen bonds with water molecules prevents the coming together of water molecules for ice nucleation. (62) Addition of DMSO also causes water efflux from the cells, thus reducing the likelihood of intracellular ice formation. (28,63) However, this does not confer the prevention of extracellular ice nucleation. This aspect is taken care of by the other component of SynAFP, i.e., PVA, which is one of the most potent FDA-approved polymers for ice recrystallization inhibition currently available. It is reported to remain in the extracellular region when added to cells, implying that any freeze–thaw method will not increase the toxicity due to its easy removal from the medium. (64,65) This explains its biocompatibility at physiological temperatures in skin cells in our study.
The mechanisms appear to be conflicting, possibly due to its anti-inflammatory properties. It’s challenging to be “friendly” to the healing of healthy tissues, whilst being toxic only to cancer cells.
DMSO appears to reduce anti-tumour immune responses, at least in one study cited earlier. Blocking macrophage phenotypic differentiation would be concerning.
M1 macrophages secrete more pro-inflammatory cytokines and are the ones you want to fight cancer; whereas M2 macrophages secrete anti-inflammatory and healing cytokines such as IL-10 and TGF-β, inhibit anti-tumor immune responses, promote tumor angiogenesis, and contribute to tumor progression and metastasis.
Although DMSO induces the differentiation of B16/F10 melanoma cells in vitro, topical administration of DMSO to mice subcutaneously implanted with B16 melanoma cells was ineffective at reducing tumor growth, DMSO was also found to block mouse macrophages from polarizing to either an M1- or an M2-phenotype, which may contribute to its inability to slow tumor growth.
From: “DMSO Represses Inflammatory Cytokine Production from Human Blood Cells and Reduces Autoimmune Arthritis” (2016)”
Although it may lack anti-tumour cytotoxicity, that doesn’t mean it isn’t of use to us as an anti-cancer therapeutic.
DMSO has been demonstrated to induce cancer cell differentiation, which is great for fighting malignancy. Differentiation may lead to functional maturity and loss of proliferative properties.
DMSO promotes at least three types of tumour suppressor
Some cancers are linked to mutations in the gene encoding for tumour suppressor proteins, such as p53 or Phosphatase and tensin homolog (PTEN).
Promotion of multiple TS’s may compensate for the loss of efficacy due to mutations.
Genetic alterations of PTEN in human melanoma (2011)
Abstract
The PTEN gene is one of the most frequently inactivated tumor suppressor genes in sporadic cancers. Inactivating mutations and deletions of the PTEN gene are found in many types of cancers, including melanoma. However, the exact frequency of PTEN alteration in melanoma is unknown. In this study, we comprehensively reviewed 16 studies on PTEN genetic changes in melanoma cell lines and tumor biopsies. To date, 76 PTEN alterations have been reported in melanoma cell lines and 38 PTEN alterations in melanoma biopsies. The rate of PTEN alterations in melanoma cell lines, primary melanoma, and metastatic melanoma is 27.6, 7.3, and 15.2%, respectively.
… Phosphatase and tensin homolog (PTEN) is 47-kDa protein and was first identified as a candidate tumor suppressor gene in 1997 after its positional cloning from a region of chromosome 10q23 known to exhibit loss in a wide spectrum of tumor types [1–3]. Since then, mutations of PTEN have been detected in a variety of human cancers including breast, thyroid, glioblastomas, endometrial, prostate, and melanoma [4–14]. Inherited mutations in this gene also predispose carriers to develop Cowden’s disease, a heritable cancer risk syndrome, and several related conditions [15–17]. PTEN is classified as a tumor suppressor because its activity is lost by deletion, mutation, or through epigenetic changes [18–21].
The Rationality of Implementation of Dimethyl Sulfoxide as Differentiation-inducing Agent in Cancer Therapy (2023)
Abstract
One of the major hallmarks of many cancer cells is dedifferentiated cells (immature cells) with little or no resemblance to normal cells. Besides the poor differentiation, malignant cells also have important features such as aggressiveness and resistance to different therapeutics. Differentiation potentiators hold great promise for cancer treatment. Dimethyl sulfoxide (DMSO) is a well-characterized pharmaceutical solvent. It is used as a component of numerous cancer therapeutic approaches, including cancer treatment and several approved cancer immune therapeutics such as Car-T cell therapy and the FDA-approved drug Mekinist (trametinib DMSO) for melanoma treatment.
… Differentiation is the cellular developmental process whereby cells change in form and develop specialized functions. The tumor cell differentiation stage is a crucial aspect of defining histopathological malignancies. The differentiation process is typically unidirectional in normal cells; however, cancer cells, like stem cells, have shown that this process can be reversible, be dedifferentiated or re-differentiated. Higher degrees of differentiation pose a better prognosis than a low degree and are strongly associated with tumor behavior, invasiveness, and resistance to cancer therapy (1).
Treating cancers through the induction of cell differentiation has been an attractive and practical approach (2). Reagents, such as all-trans-retinoic acid (ATRA), nerve growth factor (NGF), dimethyl sulfoxide (DMSO), vitamin D3, 12-0-tetradecanoylphorbol 13-acetate (TPA), peroxisome proliferator-activated receptor-gamma (PPAR-γ), hexamethylene-bis-acetamide (HMBA), transforming growth factor-beta (TGF-β), butyric acid, cAMP, and vesnarinone, have been extensively studied for their differentiation-inducing ability on cancer cells in in vitro models and validated in preclinical studies and human trials (3-5). Notably, combining differentiation agents with conventional medicine such as chemotherapy or radiation therapy, can potentiate the treatment effect seen in patients with advanced cancer (6,7).
… When using retinoic acid in combination with cytotoxic chemotherapies for acute promyelocytic leukemia (APML), the remission rates progressively improve from around 50% to more than 90% in newly diagnosed APML patients (3,10). Despite the success of ATRA, numerous challenges remain for cancer redifferentiation therapy, particularly in solid tumors.
Previously, our group reported the excellent safety profile and efficacy of DMSO for palliative care and pain control in advanced cancer patients (27-30).
Sidebar
27.Hoang BX, Le BT, Tran HD, Hoang C, Tran HQ, Tran DM, Pham CQ, Pham TD, Ha TV, Bui NT, Shaw DG. Dimethyl sulfoxide-sodium bicarbonate infusion for palliative care and pain relief in patients with metastatic prostate cancer. J Pain Palliat Care Pharmacother. 2011;25(4):350–355. doi: 10.3109/15360288.2011.606294. [DOI] [PubMed] [Google Scholar]
28.Hoang BX, Tran DM, Tran HQ, Nguyen PT, Pham TD, Dang HV, Ha TV, Tran HD, Hoang C, Luong KN, Shaw DG. Dimethyl sulfoxide and sodium bicarbonate in the treatment of refractory cancer pain. J Pain Palliat Care Pharmacother. 2011;25(1):19–24. doi: 10.3109/15360288.2010.536306. [DOI] [PubMed] [Google Scholar]
29.Hoang BX, Tran HQ, Vu UV, Pham QT, Shaw DG. Palliative treatment for advanced biliary adenocarcinomas with combination dimethyl sulfoxide-sodium bicarbonate infusion and S-adenosyl-L-methionine. J Pain Palliat Care Pharmacother. 2014;28(3):206–211. doi: 10.3109/15360288.2014.938882. [DOI] [PubMed] [Google Scholar]
30.Hoang BX, Levine SA, Shaw DG, Tran DM, Tran HQ, Nguyen PM, Tran HD, Hoang C, Pham PT. Dimethyl sulfoxide as an excitatory modulator and its possible role in cancer pain management. Inflamm Allergy Drug Targets. 2010;9(4):306–312. doi: 10.2174/187152810793358732. [DOI] [PubMed] [Google Scholar]
… DMSO as a differentiation-inducing/signal-transducing agent in experimental cancer studies.
In 1971, a series of experimental studies documented DMSO’s properties of viable differentiation-inducing activities in erythroleukemic cells (32-34). In these studies, DMSO induced differentiation by altering gene expression via regulating DNA and protein interactions through inducing conformational changes. Abnormal cell differentiation, particularly the suppression of terminal cell differentiation, exists in all tumors, especially leukemia. Tumor suppressors are vital in the gateway to terminal cell differentiation. Teimourian et al. studied the differentiation-inducing effects of DMSO and ATRA through the phosphatase and tensin homolog gene (PTEN) (35). The researchers inhibited PTEN tumor suppressor gene expression by siRNA to investigate the effect of potentiating cell survival and inhibiting apoptosis on HL-60 cell differentiation by DMSO and ATRA. The results showed that PTEN siRNA significantly increased HL-60 cell differentiation in the presence of DMSO and ATRA (35). At the same time, the presence of siRNA hampered the accumulation of apoptotic cells during incubation. The study suggested that adding DMSO could increase the efficacy of differentiation therapy through the manipulation of PTEN for acute myelogenous leukemia.
Peripheral blood leukocytes from a patient with APML are predominantly promyelocytes. When DMSO was added in the culture medium, cells were induced to differentiate into mature types of granulocytes, including myelocytes, metamyelocytes, and segmented neutrophils. All 150 clones developed from the HL-60 culture showed similar morphological differentiation with functional maturity, causing leukemic cells to lose their proliferative propertiesin the presence of DMSO (36). Theinduction of leukemic cell differentiation into mature cells is a major strategy for treating leukemia. Since differentiated leukemic cells lose their proliferative and tumor-forming abilities, different differentiation inducers have been extensively studied as valuable candidates for leukemia treatment.
… In another study, the same group of researchers demonstrated that DMSO induced up-regulation of the tumor suppressor PTEN by activating NF-kB (38). It is proposed that the degradation of phosphatidylinositol 3,4,5-trisphosphate (PIP3) to phosphatidylinositol 4,5-bisphosphate inhibits the activity of PI3K. PIP3 is an essential regulator of cell growth and survival through Akt, expressed in HL60 cells (39). Cancer survival signals are mediated mainly by PI3K/Akt (40); hence this pathway may contribute to a resistant phenotype. Therefore, an increased expression of the tumor suppressor PTEN could lead to the inhibition of Akt phosphorylation, allowing HL60 cells to differentiate into neutrophil-like cells.
The highly aggressive prostate cancer cells utilizeandrogen receptor (AR) to signal their growth and metastasis. Despite the treatment advancement achieved through androgen deprivation therapy, the recurrence of castration-resistant prostate cancer (CRPC) cannot be prevented. DMSO has been shown to suppress AR levels in the CRPC cell lines by decreasing the expression of hetero-nuclear ribonucleoprotein H1 (41). Treatment with low dose DMSO (0.1-1%) did not exhibit any cytotoxicity or changes in cell viability; minimal cytotoxicity was observed when DMSO concentration increased to 2.5% in a 96-h treatment. These clinical doses of DMSO caused a significant (p<0.01) decrease in the migratory ability of CRPC cell lines, suggesting that DMSO may decrease the metastatic ability of CRPC cells (41).
Low-dose DMSO significantly enhanced the antiproliferative effect of interferon-alpha (IFN-α) in several human lung adenocarcinoma cells in vitro and in vivo studies (42).
… Different concentrations of DMSO induced morphological changes in the adenocarcinoma cells, with 1% of DMSO causing cells to become cuboidal, polygonal, and adhere closely to each other. Additionally, when tested in conjunction with IFN-α, DMSO increased the sensitivity of the cancer cells compared to other drugs, and also increasing alkaline phosphatase activity (42). Alkaline phosphatase is a marker of type II pneumocyte maturation and differentiation (44), indicating that DMSO could potentiate cancer treatments in lung cancer patients. Another in vitro study compared the differentiation-inducing effect of DMSO and retinoic acid on a polyclonal human ovarian cancer cell line (HOC-7) (45). DMSO caused elevation of membrane-associated staining epidermal growth factor-receptor (EGF-R) and desmoplakins I and II (DPI+II) (46). After treatment, evaluation with ELISA and western blotting revealed that both DMSO and retinoic acid caused down-regulation of Myc oncoproteins, with DMSO causing a more significant reduction, leading to a decrease in cell growth. Interestingly, only treatment with DMSO caused increased epithelial cell differentiation.
Note: One of the best ways to optimise your gut butyrate levels is through taking probiotics, such as kefir:
DMSO and butyrate were studied for their effects on four human intestinal tumor cell lines in vitro (47).The growth of all four of these tumor cell lines was significantly inhibited, and doubling times increased by twofold in the presence of 2 mM butyrate and 2% DMSO. Their lectin-binding properties were evaluated using flow cytometric analysis to assess the effects on modulating cell gene expression. All four cell lines showed an increased lectin binding, indicating a differentiation-inducing effect of butyrate and DMSO on these cell lines (47).
Tsao et al. (48) evaluated three differentiation-modifying agents, sodium butyrate, DMSO, and retinoic acid, on the human rectal adenocarcinoma cell line (HRT-18) on cell growth, morphology, carcinoembryonic antigen content, cell surface membrane-associated enzyme activities, and glycoprotein profiles in vitro. All tested agents caused a marked reversible increase in doubling times, decreased saturation densities, and a markedly reduced colony-forming efficiency. DMSO caused a significant reduction in carcinoembryonic antigen levels and alkaline phosphatase activity, whereas it was shown to increase with butyrate (48).
The most attractive potential application of DMSO in cancer treatment is as an adjuvant in immunotherapy. Jiang et al. (49) proposed a possible implementation of DMSO to induce anti-tumor immunity during chemotherapy.
… Prados et al. (52) demonstrated that the addition of 1.25% DMSO can modulate cell differentiation even in rhabdomyosarcomas, poorly differentiated malignant tumors.
… The above experimental research indicates a robust differentiation-inducing activity of DMSO in different cancer cell lines, suggesting a possible practical application of this already approved pharmaceutical solvent, cryoprotectant, and drug as adjuvant therapy in conventional cancer treatment.
… Although clinical research on DMSO has regained some enthusiasm in the past 20 years, the development of DMSO as an active pharmaceutical drug or adjuvant therapeutic has not been attractive to the pharmaceutical industry, mainly because of its generic status.
… Since DMSO is inexpensive and non-patentable, pharmaceutical companies lack the financial incentive to develop this therapeutic agent in cancer clinical applications. Future non-profit and doctors-driven explorative and translational clinical investigations are needed to prove and promote the practical implementation of DMSO as a possible adjuvant drug, analgesic, and palliative care therapy for cancer patients.
Conflicts of Interest
No competing financial interests exist in relation to this study.
Growth inhibition of murine melanoma by butyric acid and dimethylsulfoxide (1986)
Abstract
Treatment of B16-F10 melanoma cells with dimethylsulfoxide (DMSO) or butyric acid (BA) inhibits cell growth and delays tumor appearance in syngeneic mice. Both agents induce morphological changes in these cells. Treatment of melanoma cells with DMSO results in a marked increase in tyrosinase activity and melanin content. BA, on the other hand, does not increase melanin content and decreases tyrosinase activity. The data show that there are marked differences in the effect of DMSO and BA on melanin biosynthesis, whereas both agents inhibit cell growth and cause a delay in tumor appearance. These findings indicate that decreased proliferation of melanoma cells and induction of melanin biosynthesis are not necessarily associated phenomena.
As you can see from some of the publishing dates, a lot of this has been known for decades, but never developed into marketable products or guidelines:
Dimethyl Sulfoxide Promotes the Multiple Functions of the Tumor Suppressor HLJ1 through Activator Protein-1 Activation in NSCLC Cells (2012)
Abstract
Background
Dimethyl sulfoxide (DMSO) is an amphipathic molecule that displays a diversity of antitumor activities. Previous studies have demonstrated that DMSO can modulate AP-1 activity and lead to cell cycle arrest at the G1 phase. HLJ1 is a newly identified tumor and invasion suppressor that inhibits tumorigenesis and cancer metastasis. Its transcriptional activity is regulated by the transcription factor AP-1. However, the effects of DMSO on HLJ1 are still unknown. In the present study, we investigate the antitumor effects of DMSO through HLJ1 induction and demonstrate the mechanisms involved.
Methods and Findings
Low-HLJ1-expressing highly invasive CL1–5 lung adenocarcinoma cells were treated with various concentrations of DMSO. We found that DMSO can significantly inhibit cancer cell invasion, migration, proliferation, and colony formation capabilities through upregulation of HLJ1 in a concentration-dependent manner, whereas ethanol has no effect. In addition, the HLJ1 promoter and enhancer reporter assay revealed that DMSO transcriptionally upregulates HLJ1 expression through an AP-1 site within the HLJ1 enhancer. The AP-1 subfamily members JunD and JunB were significantly upregulated by DMSO in a concentration-dependent manner. Furthermore, pretreatment with DMSO led to a significant increase in the percentage of UV-induced apoptotic cells.
Conclusions
Our results suggest that DMSO may be an important stimulator of the tumor suppressor protein HLJ1 through AP-1 activation in highly invasive lung adenocarcinoma cells. Targeted induction of HLJ1 represents a promising approach for cancer therapy, which also implied that DMSO may serve as a potential lead compound or coordinated ligand for the development of novel anticancer drugs.
Our third TS is a biggie: p53, “the guardian of the genome”:
Dimethyl sulfoxide activates tumor necrosis factorα-p53 mediated apoptosis and down regulates d-fructose-6-phosphate-2-kinase and lactate dehydrogenase-5 in Dalton's lymphoma in vivo (2011)
Abstract
Dimethyl sulfoxide (DMSO) is evident to induce apoptosis in certain tumor cells in vitro. However, its apoptotic mechanism remains unexplored in in vivo tumors. This article describes that DMSO, being non-toxic to the normal lymphocytes, up regulated TNFα and p53, declined Bcl-2/Bax ratio, activated caspase 9 and PARP-1 cleavage and produced apoptotic pattern of DNA ladder in Dalton's lymphoma (DL) in vivo. This was consistent with the declined expressions of tumor growth supportive glycolytic enzymes; inducible d-fructose-6-phosphate-2-kinase and lactate dehydrogenase-5 in the DL cells. The findings suggest induction of TNFα-p53-mitochondrial pathway of apoptosis by DMSO in a non-Hodgkin's lymphoma and support evolving concept of glycolytic inhibition led apoptosis in a tumor cell in vivo.
Telomerase is helpful to tumours as it helps a cell to divide indefinitely, i.e., immortality.
Dimethyl sulfoxide (DMSO) causes a reversible inhibition of telomerase activity in a Burkitt lymphoma cell line (1998)
Abstract
Introduction: Telomerase is an enzyme that is required for maintenance of telomeres. This enzyme has been shown to be present in germline tissues and majority of tumors and tumor cell lines. The regulation of telomerase is an area of active investigation in different models because, potentially, inhibition of this enzyme could be important in cancer therapy. To study the regulation of this enzyme in lymphoma cell lines, we used DMSO to produce a reversible G0/G1 arrest in Raji cell line, as shown earlier [Sawai M, Takase K, Teraoka H, Tsukada K. Reversible G1 arrest in the cell cycle of human lymphoid cell lines by dimethyl sulphoxide. Exp Cell Res 1990;187:4–10].
Methods: In this study, we use a highly quantifiable conventional (non-amplified) assay to study the effect of DMSO on telomerase. In addition, we studied cellular proliferation and cell cycle profiles of the cells treated and, subsequently, released from DMSO induced blockage.
Results: In this model, DMSO reversibly inhibited telomerase activity that could be restored after release from the blockage. The inhibition of telomerase seems to parallel cellular proliferation and it appears that telomerase is regulated upon entry into the cell cycle. This view is consistent with other previously published views on relationship of telomerase with exit from cell cycle.
Conclusion: Our observations demonstrate a novel effect of DMSO on cellular mechanisms in Raji cell line. It may provide an attractive model to further study regulation of telomerase in this cell line.
Our final paper is another cautionary note, in that the wrong dose of DMSO may promote certain cancer types. In this case, 0.2% DMSO increased the growth rate of myeloma cells by over threefold:
Low Concentration DMSO Stimulates Cell Growth and In vitro Transformation of Human Multiple Myeloma Cells (2014)
Abstract
Aims: To evaluate the effect of Dimethyl sulfoxide (DMSO) on multiple myeloma (MM) cells.
Study Design: Experimental study.
Place and Duration of Study: Department of Pathology and Genomic Medicine, the Methodist Hospital, Cancer Pathology Lab, the Methodist Hospital Research Institute, between 2011 and 2013.
Methodology: We treated RPMI 8226 and Dox-40 MM cells with DMSO. The cell growth, proliferation, apoptosis, and colony formation were examined.
Results:Exposure of RPMI 8226 and Dox-40 myeloma cells to low concentrations of DMSO resulted in a marked increase in cell growth as detected by viable cell counts and cell proliferation analysis. This DMSO-stimulated cell growth showed a dose-dependent pattern and could reach a maximal 3.57 fold-increase in the presence of 0.2% DMSO. In contrast, other common solvents including methanol and ethanol had little or no effect on cell growth. In addition, the in vitro cell transformation assay by colony formation in soft agar culture revealed that the presence of low concentrations of DMSO significantly enhanced potential of oncogenesis of myeloma cells.
Conclusion: Taken together, the findings demonstrate that DMSO could stimulate growth and the in vitro transformation of myeloma cells. However, further work is needed to understand the effect of DMSO on the pathogenesis and progression of MM.
Fig. 1. Low concentrations of DMSO enhance growth of RPMI 8226 and Dox-40 myeloma cells in a dose-dependent fashion
A, RPMI 8226 myeloma cells were cultured in the presence of different concentrations of DMSO as indicated with 2% FCS. After 5 days the cells were stained by trypan blue and the number of viable cells counted under light microscope with hemocytometer. The relative cell growth rate was determined by dividing the cell number by the number of cells counted for the control (cells cultured without DMSO). B, Dox-40 myeloma cells (doxorubicin-resistant variants of RPMI 8226 myeloma cells) were treated with different concentrations of DMSO for 5 days as indicated with 2% FCS and relative cell growth rate was evaluated. The relative cell growth rate was determined by dividing the cell number by the number of cells counted for the control (cells cultured without DMSO). The data represent the mean ± SD of 3 independent experiments. *, P < 0.05; **, P < 0.01 compared with control (cells cultured without DMSO). Statistical significance was determined by multiple comparison test after ANOVA.
Fig. 2. Enhanced DMSO effects on cell growth when cultured in low FCS concentrations
RPMI 8226 myeloma cells were cultured in different concentrations of FCS as indicated and treated with 0.2% DMSO for 3 days. The cells were stained by trypan blue and number of viable cells was counted under microscope using a hemocytometer. Open bars represent cell numbers from cultures without DMSO. Solid bars represent the cell numbers from cultures with 0.2% DMSO. The data represent the mean ± SD of 3 independent experiments. *, P < 0.05; **, P < 0.01 compared with control (cells cultured without DMSO). Statistical significance was determined by t test
Fig. 3. Methanol and ethanol had little effect on RPMI 8226 myeloma cell growth
RPMI 8226 cells were cultured in 2% FCS and exposed to methanol, ethanol, and DMSO at a final concentration of 0.05-0.8% as indicated. After culture for 3 days the cells were stained by trypan blue and number of viable cells was counted under microscope with hemocytometer. Relative cell growth rates were obtained by dividing cell numbers with exposure by cell numbers obtained in control cultures without treatment. The data represent the mean ± SD of 3 independent experiments. *, P < 0.05; **, P < 0.01 compared with control (cells cultured without treatment). Statistical significance was determined by multiple comparison test after ANOVA
… Our study also indicates that with RPMI 8226myeloma cells and its variant Dox-40 myeloma cells a low level of DMSO results in a small effect in cell apoptosis (no statistically significant difference). In contrast, some studies demonstrate that DMSO can cause the cytotoxicity [20,40]. However, the concentration of DMSO they used is 2% or 5% which is much higher than the highest concentration (0.8%) used in our study. Thus, we believe that the concentration of DMSO is critical to determine its function.
Their hypothesis appears to be that dying cancer cells, perhaps induced by radio-, chemotherapy, or DMSO, may secrete caspase 3 as a signal to other cancer cells to proliferate. Note the involvement of prostaglandin E2, which is blocked by DMSO at higher doses:
Interestingly, in the meantime of the low level of DMSO-induced apoptosis, we observed the DMSO-enhanced cell proliferation as measured by MTT assay and DMSO-improved cell growth as measured by viable cell counting with trypan blue staining. In recent study, it was shown that tumor cells that were induced to die by radiotherapy stimulate tumor regrowth [41]. Dying tumor cells were able to secrete signaling molecules for tumor cells proliferation. Caspase3 which was activated during apoptosis was required to mediate this stimulation through cleavage and activation of cytosolic calcium independent phospholipase A2 (iPLA2) that ultimately produces prostaglandin E2 [41,42]. Therefore, radio-and chemotherapy-induced apoptotic tumor cells can induce proliferation of surviving tumor cells, which may dampen the therapy effect [43]. In addition, we found that the presence of DMSO augmented in vitro transformation/colony formation of RPMI 8226 myeloma cells. Taken together, our findings demonstrate that low levels of DMSO have an overall stimulating effect on in vitro cell growth and potential of transformation of RPMI 8226myeloma cells.
RxList is an online reference for drugs typically available on prescription. Even though DMSO is easily obtained, self-medication without medical supervision is not recommended, as the therapeutic window for some applications is quite small - you may make some conditions worse; and what you buy online may actually be “industrial grade” and contain impurities.
Don’t read about DMSO, buy a 500ml bottle of the stuff and go splashing it around or swallowing it without medical advice!
Side Effects
DMSO is LIKELY SAFE when used as a prescription medication. Don't use products that are not prescribed by your health professional. There is concern that some non-prescription DMSO products might be “industrial grade”, which is not intended for human use. These products are POSSIBLY UNSAFE, as they can contain impurities that can cause health effects. To make matters worse, DMSO readily penetrates the skin, so it carries these impurities rapidly into the body.
Some side effects of taking DMSO by mouth or applying it to the skin include skin reactions, dry skin, headache, dizziness, drowsiness, nausea, vomiting, diarrhea, constipation, breathing problems, vision problems, blood problems, and allergic reactions. DMSO also causes a garlic-like taste, and breath and body odor.
Precautions
Pregnancy and breast-feeding: There is not enough reliable information about the safety of taking DMSO if you are pregnant or breast-feeding. Stay on the safe side and avoid use.
Diabetes: There are reports that topical use of DMSO can change how insulin works in the body. If you use insulin to treat diabetes and also use DMSO, monitor your blood sugar closely. Insulin doses may need to be adjusted.
Certain blood disorders. Injecting DMSO intravenously (by IV) might cause red blood cells to break down. This might be a problem for people with certain blood disorders. DMSO might make these conditions worse.
Liver problems: DMSO might harm theliver. If you have liver conditions and use DMSO, be sure to get liver function tests every 6 months.
Kidney problems: DMSO might harm thekidneys. Kidney function tests are recommended every 6 months if you use DMSO and have a kidney condition.
Interactions
Medications applied to the skin, eyes, or ears (Topical drugs)
Interaction Rating: Moderate
Be cautious with this combination. Talk with your health provider.
DMSO can sometimes increase how much medicine the body absorbs. Applying DMSO along with medications you put on the skin or in the eyes or ears can increase how much medicine your body absorbs. Increasing how much medicine your body absorbs might increase the effects and side effects of the medicine.
Medications given as a shot (Injectable drugs)
Interaction Rating: Moderate
Be cautious with this combination. Talk with your health provider.
DMSO (dimethylsulfoxide) might help the body absorb some medicines. Using DMSO and getting a shot might increase how much medicine the body absorbs and increase the effects and side effects of medications given as a shot.
Medications taken by mouth (Oral drugs)
Interaction Rating: Moderate
Be cautious with this combination. Talk with your health provider.
DMSO (dimethylsulfoxide) might increase how much medicine your body absorbs. Taking DMSO along with medications taken by mouth might increase how much medicine your body absorbs. Increasing how much medicine your body absorbs can increase the effects and side effects of your medicines.
Dosing
The following doses have been studied in scientific research:
APPLIED TO THE SKIN:
For prevention of some side effects of cancer treatment: 77-90% DMSO is typically applied under medical supervision every 3-8 hours for 10-14 days.
For shingles (herpes zoster): 5-40% idoxuridine in DMSO is within 48 hours after the appearance of a rash and applied every 4 hours for 4 days.
For nerve pain: 50% DMSO solution has been used 4 times daily for up to 3 weeks.
For osteoarthritis: 25% DMSO gel has been used 3 times a day, and 45.5% DMSO topical solution has been used 4 times a day.
It's important to note that DMSO is POSSIBLY UNSAFE when applied to the skin. There are reports that industrial-grade DMSO is being used for self-treatment of several disease conditions. Industrial-grade DMSO is not of the same quality as the DMSO that is used for drug research purposes since it may contain impurities. DMSO easily penetrates the skin and brings along impurities and other substances that may be hazardous to health.
INSIDE THE BLADDER:
For frequent urge to urinate (interstitial cystitis) and for chronic inflammatory bladder disease: Healthcare providers drip a DMSO solution into the bladder using a tube called a catheter. The catheter is removed and the patient is asked to hold the solution for a period of time before urinating.
We do know that DMSO may interact with other medications, including organophosphates, cholinesterase inhibitors, the NSAID drug “Sulindac”, and the benzoporphyrin derivative photosensitizer “Verteporfin”14.
But that’s not what the Lawrence Livermore investigators are saying:
Death of Gloria Ramirez
Gloria Cecilia Ramirez (January 11, 1963 – February 19, 1994)[1] was an American woman who was dubbed the Toxic Lady or the Toxic Woman by the media when several hospital workers became ill after airborne exposure to her body and blood. Ramirez had been admitted to the emergency room suffering from late-stage cervical cancer. While treating Ramirez, three hospital workers fainted, and others experienced symptoms such as shortness of breath and muscle spasms. Five workers required hospitalization, one of whom remained in an intensive care unit for two weeks. Ramirez herself died from complications related to her cancer shortly after arriving at the hospital.
The incident was initially considered to be a case of mass hysteria. An investigation by Lawrence Livermore National Laboratory suggested that Ramirez had been self-administering dimethyl sulfoxide (DMSO) as a pain treatment. The oxygen from the mask provided by paramedics during her transport to the hospital likely converted the DMSO into dimethyl sulfate (DMS), a highly toxic and carcinogenic alkylating agent. Although dimethyl sulfate has a very low vapor pressure at body temperature, it is believed to have transitioned to a gaseous state due to the vacuum inside the vacutainer. This is similar to how water boils at a lower temperature when exposed to low pressure. This theory has been endorsed by the Riverside Coroner's Office and published in the journal Forensic Science International.
Investigation
… The Riverside County health specialist department called in California's Department of Health and Human Services, which put two scientists, Drs. Ana Maria Osorio and Kirsten Waller, on the case. They interviewed 34 hospital staff who had been working in the emergency room on February 19. Using a standardized questionnaire, Osorio and Waller found that the people who had developed severe symptoms, such as loss of consciousness, shortness of breath and muscle spasms, tended to have certain things in common. People who had worked within two feet of Ramirez and had handled her intravenous lines had been at high risk. But other factors that correlated with severe symptoms did not appear to match a scenario in which fumes had been released: the survey found that those afflicted tended to be women rather than men, and they all had normal blood tests after the exposure. They believed the hospital workers suffered from an incident of mass hysteria.[4] In total, 27 of the 37 staff members in the emergency room that night reported feeling some type of symptom.[3]
Gorchynski denied that she had been affected by mass hysteria and pointed to her own medical history as evidence. After the exposure, she spent two weeks in the intensive care unit with breathing problems. She developed hepatitis and avascular necrosis in her knees. The Riverside Coroner's Office contacted the Lawrence Livermore National Laboratory to investigate the incident. Livermore postulated[citation needed] that Ramirez had been using dimethyl sulfoxide (DMSO), a solvent most commonly used as a degreaser, as a home remedy for pain. Users of this substance report that it has a garlic-like taste.[4]Sold in gel form at hardware stores, topical application to Ramirez's skin could explain the greasy appearance of Ramirez's body.[4][5]Livermorescientists theorized that the DMSO in Ramirez's system might have built up owing to urinary blockage caused by her kidney failure.[5] Oxygen administered by the paramedics would have combined with the DMSO to form dimethyl sulfone (DMSO2); DMSO2 is known to crystallize at room temperature, and crystals were observed in some of Ramirez's drawn blood.[4]Electric shocks administered during emergency defibrillation could have then converted the DMSO2 into dimethyl sulfate (DMSO4), the highly toxic dimethyl ester of sulfuric acid, exposure to which could have caused the reported symptoms of the emergency room staff.[6] Livermore scientists postulated on The New Detectives that the change in temperature of the blood drawn, from the 98.6 °F (37 °C) of Ramirez's body to the 64 °F (18 °C) of the emergency room, may have also contributed to a conversion from DMSO2 into DMSO4. However, many organic chemists are dismissive of this theory, citing the length of time required for a reaction like this to occur and the fact that the human body is not warm enough for the conversion to happen.[3]
This case was one of the most extensive investigations in medical history, with "medical detectives from ten local, state and federal outfits," examining dozens of potential causes behind the hysteria. In the end, it was suggested that the staff underwent an outbreak of a mass sociogenic illness, which could have been a result of the chemical conversion described above.[3]
AI to replace qualified staff, hospitals, and wards?
Instead of being honest about poisoning the population with COVID vaccines, etc, the UK’s answer to the consequential ramp-up in waiting lists was a recent proposal to increase the number of diagnostic centres and surgical hubs.
The UK Column recently reported on this Next Big Thing™.
It goes something like this:
You fill in an online questionnaire. Note that you never have contact with a doctor.
You send in a blood sample so that your DNA can be profiled.
They are not looking for tumour-suppressor gene mutations or anything like that, just for correlations with, say, diabetes, mental illness, or obesity.
You may have “unhealthy genes”, but just as epigenetics makes one twin into a psychopath but not the other, correlation isn’t causation.
And the reverse is true. You may have a “healthy profile”, and yet still progress to disease decades earlier than this alone would predict.
I guess they aren’t profiling your lipid drop phases either.
Your demographic profile is considered, and a software medic “diagnoses” you.
For instance, perhaps you live in an impoverished seaside town. You must be obese and at risk of diabetes, especially if your DNA profile is unclean. You are from Glasgow you say? Yup, you must be an alcoholic.
A “pre-crime” prescription of something useless (or worse than useless, long term) is recommended.
Predictix: DNA, AI, and the Infiltration of UK Mental Health
Predictix Digital: Predictix Genetics: The next generation in genetic testing
PREDICTIX Genetics is a mental health clinical decision support tool that harnesses Artificial Intelligence (AI) with genetic testing and clinical insight […]
Predictix AI: Driving Health Outcomes with AI (Dr. Dekel Taliaz)
Association of Jews of Vilna and vicinity in Israel: Eisenberg family
The Predictix algorithms go beyond traditional genetic testing, by holistically understanding patients' unique genetic code, alongside their clinical history and demographic data. With this new level of clinical predictions, we can help improve patients’ quality of life and reduce the number of patients dropping out of treatment.
Genetic and demographic profiling isn’t medicine. It’s Ferguson-style modelling, and a pseudo-science.
It’s the Big Pharma equivalent of the conman who walks up and down your street looking for old ladies with broken concrete drives, then rips them off with low-quality tarmac they don't need.
The “leftover asphalt scam”
We had the scamdemic, now Gormless Wes plans to take it to the limit one more time.
This article mentions getting workers approaching retirement age signed up “for activities such as voluntary work, hobbies and exercise, in a bid to maintain health”, but from the preamble, proposed use of smartphone apps, and trials of blood pressure checks at the dentists, we know it’s more about pushing drugs and 100-day vaccines on the population.
Streeting plots ‘game-changing’ health MOTs
NHS technology could give patients personalised advice based on genes, lifestyle and demographic group
Wes Streeting, the Health Secretary, says his approach is inspired by advances in Japan Credit: Heathcliff O'Malley for The Telegraph
Personalised health MOTs could be offered to everyone approaching retirement age under plans being considered by the Health Secretary.
Wes Streeting said the approach – inspired by advances in Japan – could prove a “game changer” that revolutionises the way Britain delivers health care.
Officials are examining the use of personalised technology, including genomic profiling, as they draw up a 10-year plan for the NHS, which is expected to be published in June.
The Health Secretary told The Telegraph: “I think Japan is interesting on two fronts. I’m particularly interested in the science and technology side, where you’d expect Japan to be a leader, but also they’ve got a very significant ageing society, so [looking at] how they support people to age.”
He said the country was embarking on a “really interesting approach” combining genomics and AI machine learning to create personalised MOTs.
… Some health experts believe that the Japanese model could be integrated with a scheme from Brazil, which has already begun being rolled out in parts of the UK.
Under the door-knocking scheme, first piloted in London, community health workers are sent to carry out checks on the health and wellbeing of whole streets at a time.
Some common sense from a former health secretary, although the V-word is still verboten and Brazil is a hell-hole of vaccine mandates, door-to-door intimidation and persecution:
AI alone cannot fix NHS, former health secretary warns Streeting
A former health secretary has warned that Wes Streeting cannot solely rely on artificial intelligence (AI) to fix the NHS.
Dame Patricia Hewitt, who preceded Mr Streeting in the role from 2005 to 2007, suggested more traditional methods of care could also keep elderly people healthy for longer.
In a letter to The Telegraph, Dame Patricia wrote: “Personalised health checks for older people are vital. But truly radical reform of the NHS must not be all about genomic profiling and AI, as Wes Streeting appears to suggest.”
The former Labour MP pointed to a scheme in Brazil where community health agents go from door to door. The Telegraph reported earlier this month that they provide health advice, education and links to health services.
… She also lauded Australia’s health checks for all 75-year-old citizens, which look for signs of osteoporosis, skin cancer and depression.
“These countries take an approach to healthy ageing that genuinely gets to the roots of the problem, and would achieve far better results at even lower cost than today’s out-of-date programmes,” Dame Patricia wrote.
… Japan has developed the world’s fastest supercomputer, Fugaku, which is now being used to accelerate research in personalised medicine.
Mr Streeting hopes to take a similar approach, ultimately giving everyone personalised advice based on their genes, lifestyle and demographic group.
He said that by using genomics and AI “people aren’t just getting a general MOT, but a personal one ... where we’re able to very early on, not only diagnose earlier and treat faster, but predict and prevent illness”.
Mr Streeting added: “That is a game-changer, and that is the kind of exciting revolution in medical technology and life sciences that is just going to completely change the way we think about, let alone deliver, health and care.
My serum vitamin levels are too low, especially D or K2, perhaps due to long-term statin misuse or diet?
My plasma magnesium indicates a deficiency. This is difficult to measure as our bones act as a store. An AI program may be of genuine benefit here by analysing your diet. But Gormless Wes isn’t interested in that.
I have gut microbiome dysbiosis and need to review my diet. Do I need to increase my pre and pro-biotic intake? Butyrate?
I am insulin resistant?
Do I have elevated levels of post-vaccination IgG-4 or Spike protein antibodies?
My CD4+ and CD8+ T cell counts are normal?
I am anaemic or have ferroptosis?
Do I have excess serum linoleic acid and vascular or systemic inflammation, due to following official dietary advice?
I have elevated ApoB, a heart disease marker that is missed by cholesterol checks?
Is my cardiac output too low?
If you are going to profile my genes, please provide a genetic methylation check, so that I know which genes are turned on or off.
Whilst I was wrapping this up, with perfect timing, Zerohedge just posted about the growing popularity of at-home biomarker testing.
The expert they consulted suggested some more biomarkers and a lifestyle approach to improvement. In other words, a move away from “population averages”, so beloved by Wes.
I’m pleased to see vitamin D on the list, and that they emphasise that one size doesn’t fit all - we are all different:
Why More People Are Testing Their Blood Without A Doctor
The scale doesn’t lie—but it doesn’t tell the whole story.
You might be eating better, exercising more, and still seeing the same number each morning. It’s frustrating, discouraging, and, as it turns out, possibly misleading.
For decades, weight has been treated as a primary marker of health. But a number on the scale says little about inflammation, cardiovascular risk, or metabolic dysfunction—factors that often shift before any visible weight loss appears.
… Your Body, Your Baseline
At-home testing shifts the focus from population averages to personal baselines—moving health tracking from what works for most to what works for you.
This idea underpins “N=1 medicine,” a growing movement in which individuals act as their own experiments. Instead of relying on annual checkups or generic advice, users collect data, track trends, and make changes based on what works for them.
But where to begin?
Lufkin recommends starting with a foundational lab panel that includes fasting insulin, fasting glucose, HbA1c (a longer-term marker of blood glucose levels), triglycerides and HDL (to calculate the ratio), CRP (a marker of inflammation), LDL-C, and vitamin D.
“These give a snapshot of your metabolic and inflammatory status—far more informative than weight or BMI,” he said.
Once you have your baseline, Lufkin advises a gradual, focused approach:
Pick one change, such as cutting added sugar, walking after meals, or improving sleep.
Track how you feel—energy, mood, cravings, and digestion often shift before lab numbers do.
Retest every three to six months to monitor trends and confirm your direction.
“Even small improvements confirm that your efforts are working—long before the mirror shows it,” he said.
Ultimately, at-home testing isn’t about micromanaging every fluctuation. “You don’t need to be perfect—just curious,” Lufkin said. “Let data guide your next best step. That’s real empowerment.”
Before reading the literature, I had no idea about the broad-spectrum therapeutic properties of DMSO, or just how quickly it enters the circulation after topical application. I was quite skeptical.
But now my skepticism moves across to that of the FDA, other health regulators, and the shamefully conflicted research charities (a recurring theme!). They appear to have done their best to try to bury it for over 50 years, using vague, vaporous excuses.
This was another Substack that ended up much longer than expected, because the research is so extensive. However, cancer treatment roles for DMSO need to be developed by conducting more clinical trials, especially as a co-treatment with existing regimes.
I think it has great appeal for emergency use in response to muscle pain, skeletal injuries, burns, frostbite, or strokes. But throughout we have seen how important it is to use genuine pharmaceutical-grade products, to avoid cross-contamination, to be wary of long-term use, and, most importantly, to be administered under expert guidance for dosing.
It’s healing properties appear to be invaluable, although it’s something of a mixed bag. I was somewhat surprised to see its cytotoxic effects on some cell lines, such as the collagen-forming chondrocytes, and the myelin-forming oligodendrocytes. DMSO is quite a powerful drug, but care is needed because of this, and it can potentiate the effects of other drugs.
Although considered to be a very safe drug when taken under medical supervision, if you get it wrong, it may make your allergic condition or arthritis worse, promote cancer growth, or cause a relapse of your MS. It could even kill you, due to contamination.
DoorlessCarp’s Scientific Literature Reviews is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
A hat tip to the brilliant Annelise for linking to this study in her post about DMSO:
"The extreme changes in microRNAs and alterations in the epigenetic landscape indicate that DMSO is not inert. Its use should be reconsidered, especially for cryopreservation of embryos and oocytes, since it may impact embryonic development."
Note that the effective dose is only 0.1%, and over 2000 genes for protein expression were either upregulated or downregulated by DMSO, affecting multiple organs.
They used human 3D microtissues (MTs) in a maturing cardiac model and a mature hepatic (liver) model, and exposed these to 0.1% DMSO for two weeks, and took samples at 2, 8, 72, 168, 240, and 336 hours.
Maturing cardiac MTs were most affected, and 60.7% of 2051 differentially expressed genes were downregulated. The authors conclude that this poses the greatest threat to the developing embryo, due to DMSO-induced ATP decrease. We also saw an ATP decrease in the study of the effects of DMSO on erythrocytes (red blood cells).
DMSO induces drastic changes in human cellular processes and epigenetic landscape in vitro (2019)
Abstract
Though clinical trials for medical applications of dimethyl sulfoxide (DMSO) reported toxicity in the 1960s, later, the FDA classified DMSO in the safest solvent category. DMSO became widely used in many biomedical fields and biological effects were overlooked. Meanwhile, biomedical science has evolved towards sensitive high-throughput techniques and new research areas, including epigenomics and microRNAs. Considering its wide use, especially for cryopreservation and in vitro assays, we evaluated biological effect of DMSO using these technological innovations. We exposed 3D cardiac and hepatic microtissues to medium with or without 0.1% DMSO and analyzed the transcriptome, proteome and DNA methylation profiles. In both tissue types, transcriptome analysis detected >2000 differentially expressed genes affecting similar biological processes, thereby indicating consistent cross-organ actions of DMSO. Furthermore, microRNA analysis revealed large-scale deregulations of cardiac microRNAs and smaller, though still massive, effects in hepatic microtissues. Genome-wide methylation patterns also revealed tissue-specificity. While hepatic microtissues demonstrated non-significant changes, findings from cardiac microtissues suggested disruption of DNA methylation mechanisms leading to genome-wide changes. The extreme changes in microRNAs and alterations in the epigenetic landscape indicate that DMSO is not inert. Its use should be reconsidered, especially for cryopreservation of embryos and oocytes, since it may impact embryonic development.
… Results
The proteome (approximately 2,000 measured proteins), the full transcriptome (including miRNAs) and whole-genome methylation were measured on material obtained from the same sample. Figure 1 contains a graphical overview of the experimental design. In order to obtain a first overview of DMSO-induced cross-omics effects, amounts of differentially changed entities (all corrected for multiple testing using FDR <0.05) are summarized for each platform. Numbers of differentially changed entities differed between the tissue types, with cardiac samples showing a larger effect of DMSO than hepatic, with the exception of mRNAs. This difference is especially noticeable for miRNAs and genome methylation. Because proteomics data was least informative due to its partial nature, these results were included in Supplementary Data. Furthermore, principal component analysis (PCA), using averages of triplicates, for each platform (Fig. 2 & Supplementary Data) depicts clear differences between 0.1% DMSO exposed (DMSO) and untreated (UNTR) samples, with the exception of methylation in hepatic MTs.
Figure 1. Graphical overview of experimental design combined with summary of differential entities of each analysis method. Tissue-specific information is depicted in orange for cardiac and green for hepatic. Furthermore, exposures are coloured blue and measurement platforms purple. Abbreviations: h = hours; mRNA = messenger RNA; miRNA = microRNA.
… DMSO effects on cellular processes
DMSO effects on mRNAs were depicted by of PCA (Fig. 2a,b). The clear separation between UNTR and 0.1% DMSO indicated that DMSO was able to affect cellular processes by altering gene expression. Comparison between DMSO and UNTR resulted in 2051 differentially expressed genes (DEGs = FDR <0.05; of which 871 with |log2FC| >1) in cardiac MTs and 2711 DEGs (of which 1879 with |log2FC| >1) in hepatic MTs, of which 60.7% and 62.9% DEGs were downregulated respectively.
… Observed changes in cellular processes include changes in mitochondrial pathways linked to ROS production and cellular ATP generation. DMSO is a known radical scavenger23. While this property of DMSO may provide protection against high levels of ROS, at normal or decreased levels of ROS, it may hamper basal cell metabolism by scavenging electrons needed for ATP production24. The resulting decrease in ATP content was observed in our two DMSO treated cell models (Supplementary Fig. 2). Cardiac MTs showed a steep decrease over time (87% decrease after 2 weeks of exposure), while the ATP content of hepatic MTs show a small decrease initially (36% decrease in the first 72 h), after which ATP content slowly recovered to baseline level.
… Within assisted reproductive technology, the ATP content is a good predictor of embryo viability. The DMSO-induced ATP decrease, especially in the cleavage-stage, can induce downstream effects that may disrupt cellular function, implantation ability and fetal development25,26. DMSO-induced reduction in implantation rates and pregnancy losses were already observed from animal models27.
… Conclusions
Our study highlights the capability of DMSO to induce changes in cellular processes in both cardiac and hepatic cells, but more severely, induce alterations in miRNA and epigenetic landscape in the 3D maturing cardiac model. The changes in cellular processes can have consequences for conclusions drawn from cell assays and therefore also in any application of these findings (e.g. false negative drug toxicity conclusions). Furthermore, the extreme changes in miRNA and alterations in the epigenetic landscape may pose a threat, especially for assisted reproductive technology. Genome-wide hypermethylation induced by global deregulation of methylation mechanisms, especially when it affects genes important in development, may have negative consequences directly, later in life or possibly in later generations.
Overall, use of DMSO should be avoided where possible. However, for the time being, DMSO is indispensable within biotechnological applications. In these cases, the effects that DMSO may have should be considered and the concentration should be kept as low as possible, becauseeven at low concentrations DMSO is not inert.
This site is strictly an information website reviewing research into potential therapeutic agents. It does not advertise anything, or provide medical advice, diagnosis, or treatment. This site does not promote any of these as potential treatments or offer any claims for efficacy. Its content is aimed at researchers, registered medical practitioners, nurses, or pharmacists. This content is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website. Always consult a qualified health provider before introducing or stopping any medications as any possible drug interactions or effects will need to be considered.
Any extracts quoted in the previous article are for non-commercial research and educational purposes only and may be subject to copyright from their respective owners.
Kolb, K. H., G. Jaenicke, M. Kramer, and P. E. Schulze. ‘Absorption, Distribution and Elimination of Labeled Dimethyl Sulfoxide in Man and Animals’.Annals of the New York Academy of Sciences 141, no. 1 (1967): 85–95. https://doi.org/10.1111/j.1749-6632.1967.tb34869.x.
Wong, K. K., G. M. Wang, J. Dreyfuss, and E. C. Schreiber. ‘Absorption, Excretion, and Biotransformation of Dimethyl Sulfoxide in Man and Miniature Pigs after Topical Application as an 80 per Cent Gel’. The Journal of Investigative Dermatology 56, no. 1 (January 1971): 44–48. https://doi.org/10.1111/1523-1747.ep12291900.
1. Layman DL, Jacob SW. The absorption, metabolism and excretion of dimethyl sulfoxide by rhesus monkeys. Life Sci. 1985;37(25):2431-2437. doi:10.1016/0024-3205(85)90111-0
Oertel RP. Protein conformational changes induced in human stratum corneum by organic sulfoxides: An infrared spectroscopic investigation.Biopolymers. 1977;16(10):2329-2345. doi:10.1002/bip.1977.360161017
Fourier transform raman spectroscopy of interactions between the penetration enhancer dimethyl sulfoxide and human stratum corneum.International Journal of Pharmaceutics. 1995;125(2):265-282. doi:10.1016/0378-5173(95)00141-5
Wang L, Xu M, Jones OD, et al. Nonalcoholic fatty liver disease experiences accumulation of hepatic liquid crystal associated with increasing lipophagy. Cell Biosci. 2020;10:55. doi:10.1186/s13578-020-00414-2
Notman R, Noro M, O’Malley B, Anwar J. Molecular Basis for Dimethylsulfoxide (DMSO) Action on Lipid Membranes. J Am Chem Soc. 2006;128(43):13982-13983. doi:10.1021/ja063363t
Gironi B, Kahveci Z, McGill B, et al. Effect of DMSO on the Mechanical and Structural Properties of Model and Biological Membranes.Biophys J. 2020;119(2):274-286. doi:10.1016/j.bpj.2020.05.037
Chemicals NRC (US) P on A, Chemicals NRC (US) P on A. ANTICHOLINESTERASES. In: Possible Long-Term Health Effects of Short-Term Exposure to Chemical Agents: Volume 1 Anticholinesterases and Anticholinergics. National Academies Press (US); 1982. Accessed April 22, 2025. https://www.ncbi.nlm.nih.gov/books/NBK217772/
Glaviano A, Foo ASC, Lam HY, et al. PI3K/AKT/mTOR signaling transduction pathway and targeted therapies in cancer.Molecular Cancer. 2023;22(1):138. doi:10.1186/s12943-023-01827-6
I would have to concur with these findings, and link to a pdf of 132 references is provided:
"How DMSO Naturally Eliminates Cancers
Analysis by A Midwestern Doctor"
"... In the first part of this series, I presented dozens of studies that show DMSO effectively treats cancer pain (which is often very challenging to address) and dramatically reduces many of the complications experienced from radiation therapy and chemotherapy (as it selectively protects healthy cells from those agents).
Given how debilitating each of those can be for a cancer patient, it is remarkable DMSO has not been adopted for any of those applications, particularly since addressing those does not take business from the cancer industry (and if anything would make more patients want to undergo conventional cancer care).
Note: 65% of oncologists' revenue comes from chemotherapy drugs3 (which coincidentally are by far the most profitable drug market4)."
While cautionary advice should be heeded in the use of any medication, it should be noted that pharmaceutical grade and uncontaminated DMSO for human use is widely available from legitimate sources and reputable companies; one needn't visit your local hardware store.














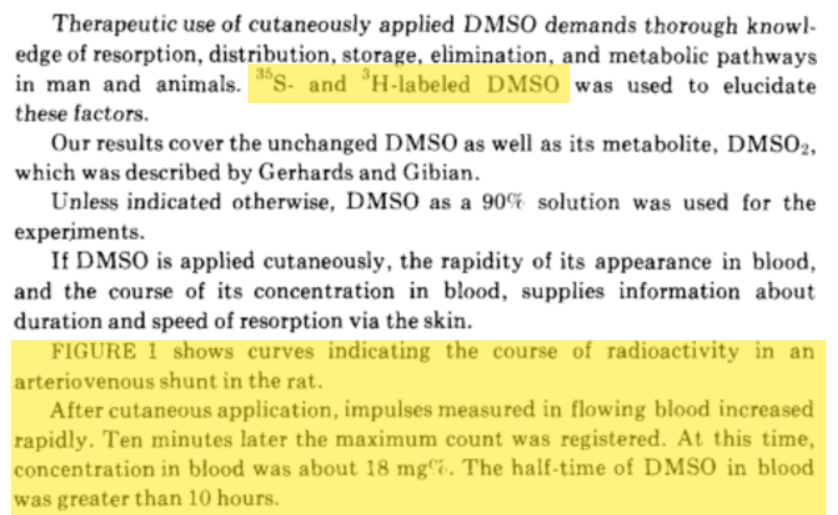
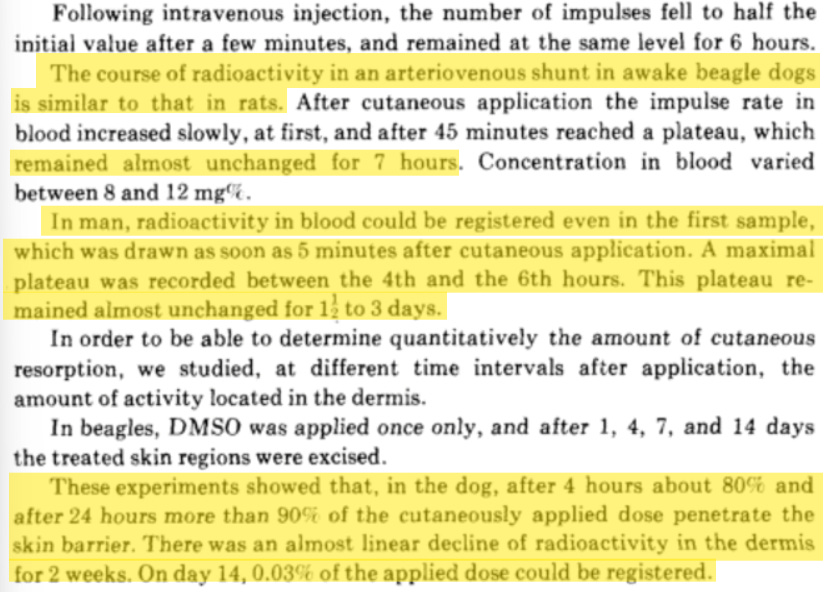





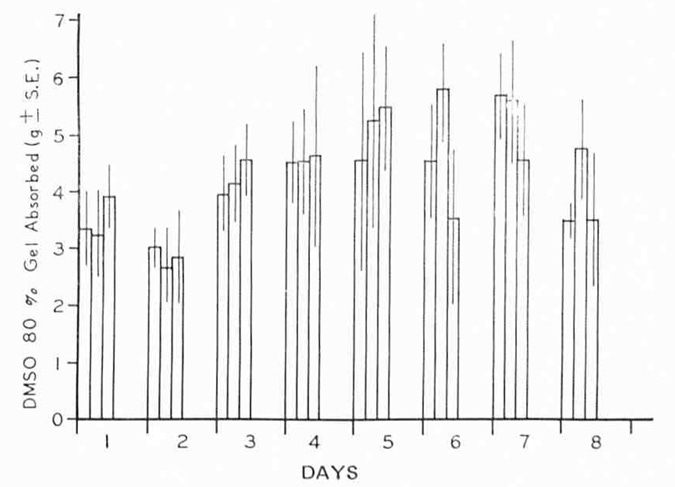


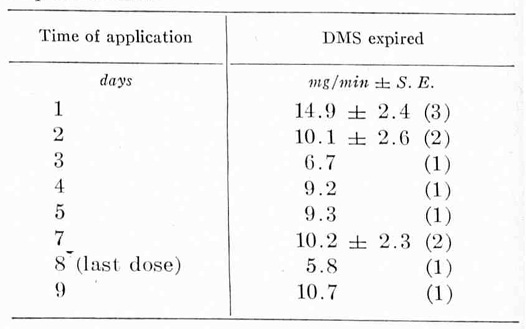
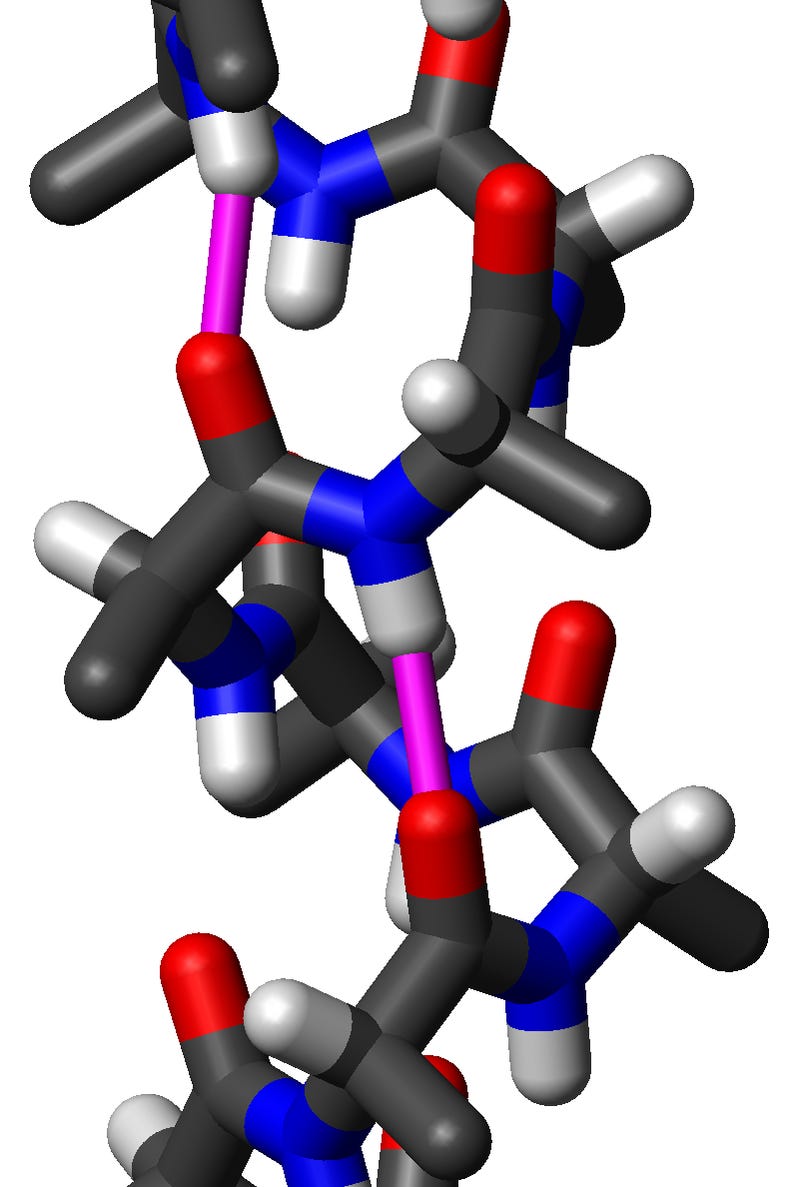

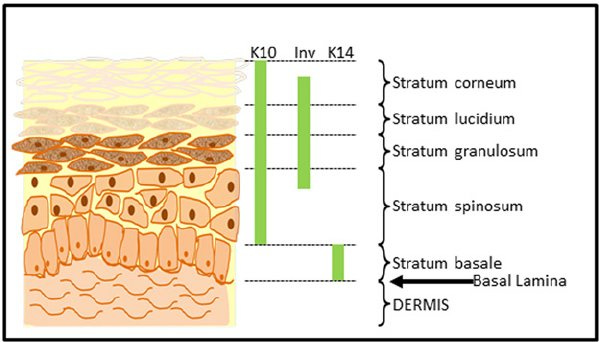


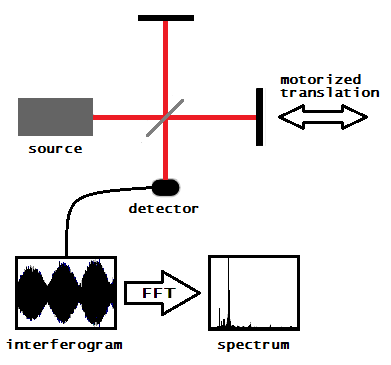
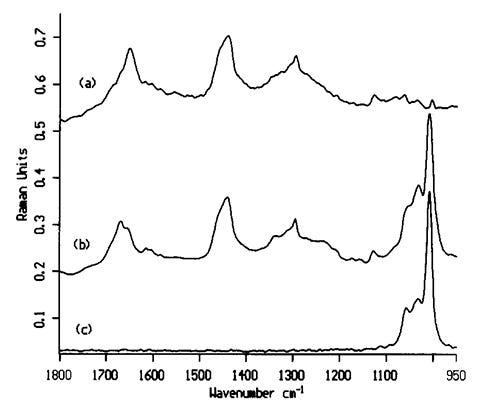

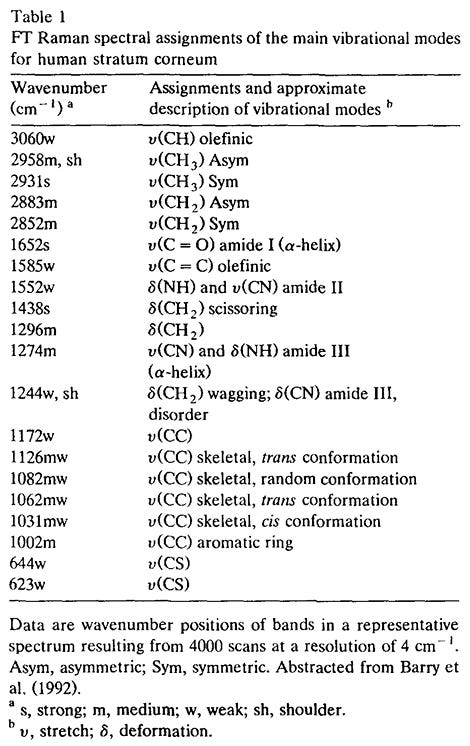

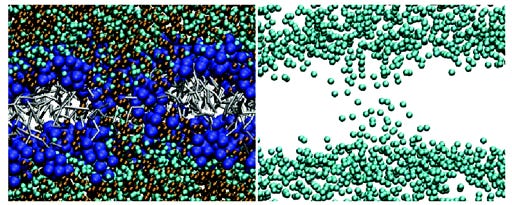

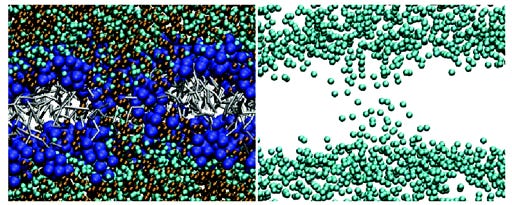


 Affects the Myelin Shealth")

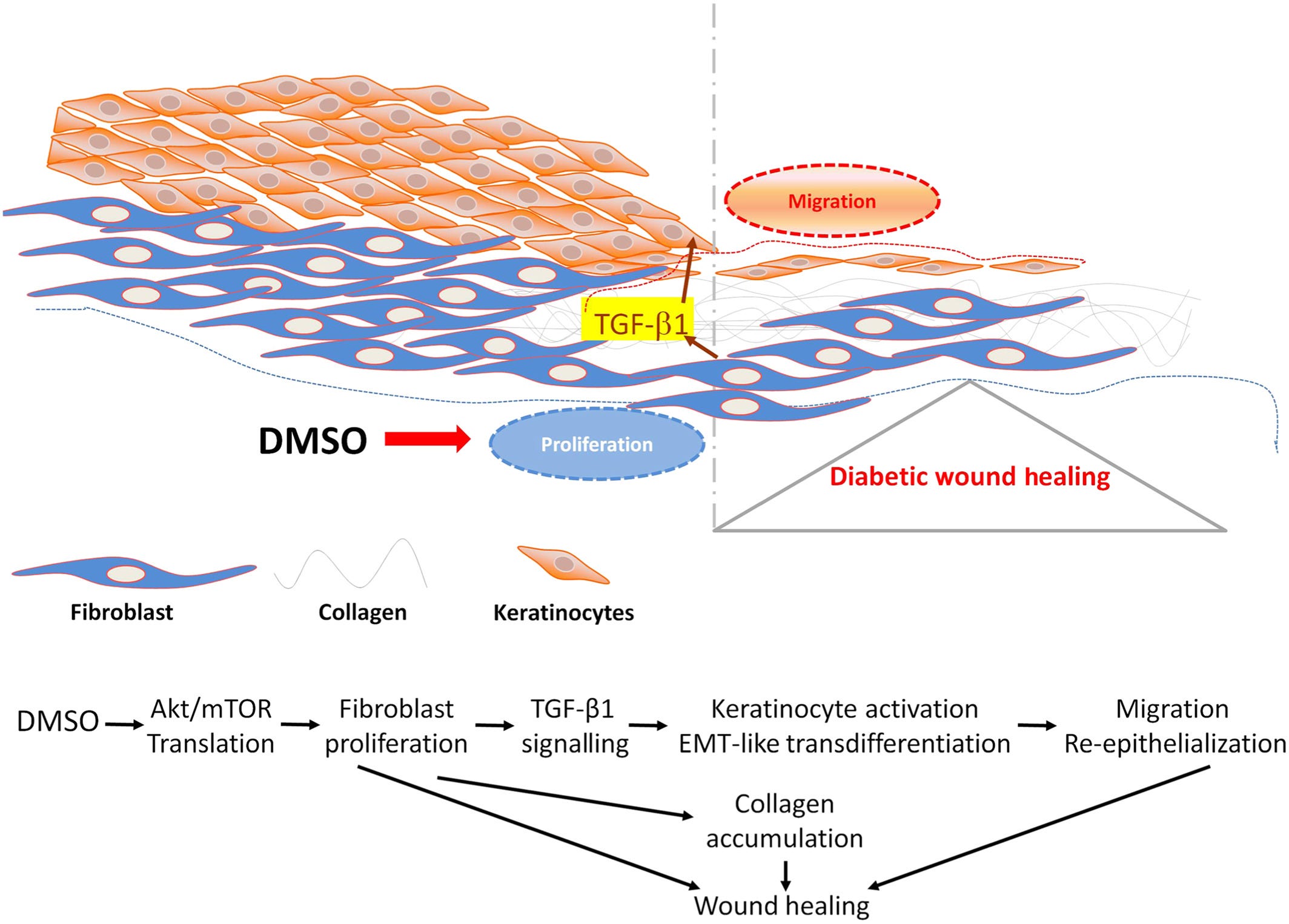


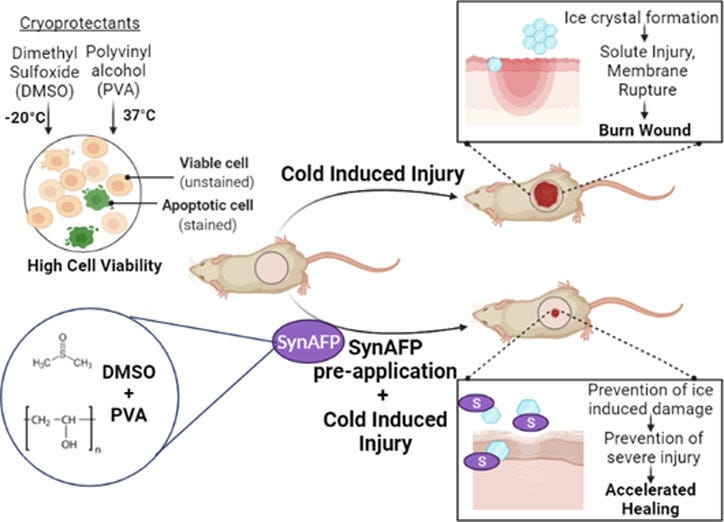

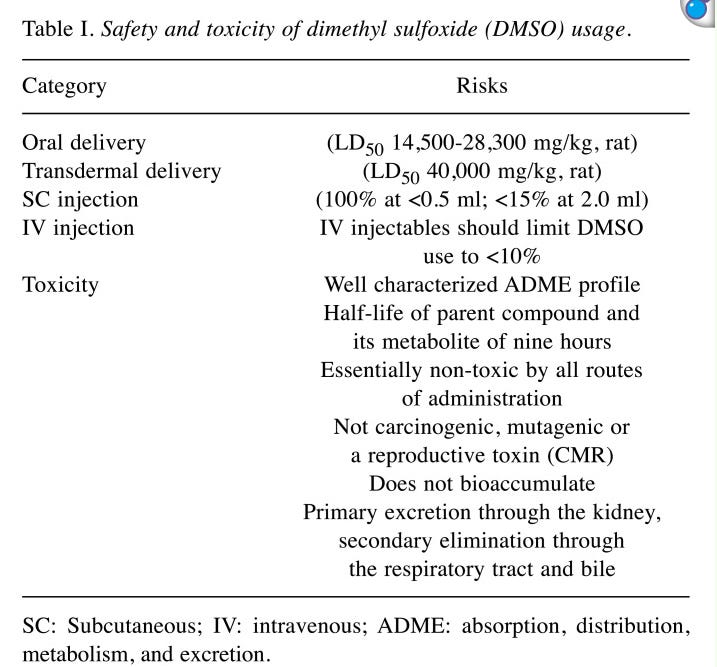


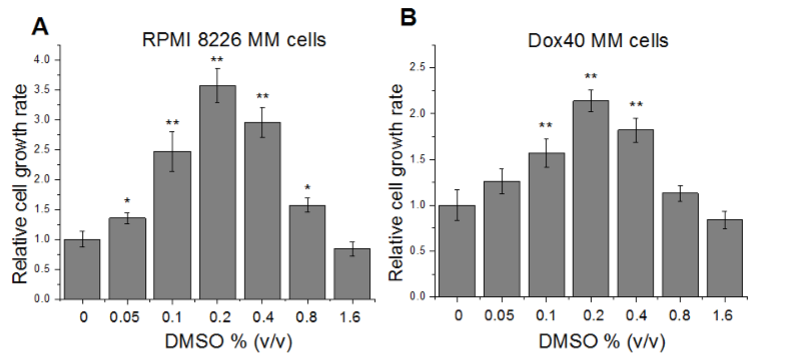
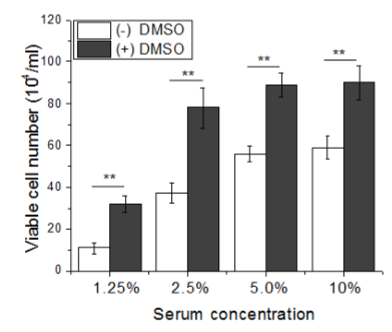
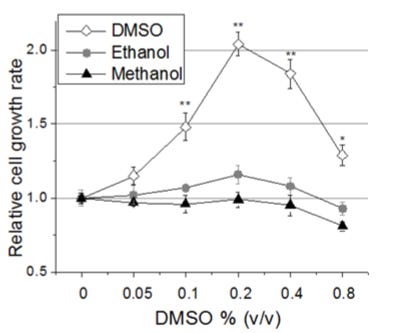








I would have to concur with these findings, and link to a pdf of 132 references is provided:
"How DMSO Naturally Eliminates Cancers
Analysis by A Midwestern Doctor"
"... In the first part of this series, I presented dozens of studies that show DMSO effectively treats cancer pain (which is often very challenging to address) and dramatically reduces many of the complications experienced from radiation therapy and chemotherapy (as it selectively protects healthy cells from those agents).
Given how debilitating each of those can be for a cancer patient, it is remarkable DMSO has not been adopted for any of those applications, particularly since addressing those does not take business from the cancer industry (and if anything would make more patients want to undergo conventional cancer care).
Note: 65% of oncologists' revenue comes from chemotherapy drugs3 (which coincidentally are by far the most profitable drug market4)."
https://articles.mercola.com/sites/articles/archive/2025/04/18/how-dmso-naturally-eliminates-cancers.aspx
While cautionary advice should be heeded in the use of any medication, it should be noted that pharmaceutical grade and uncontaminated DMSO for human use is widely available from legitimate sources and reputable companies; one needn't visit your local hardware store.