short story - novelette - novella -novel - PhD thesis - Trump’s tariff list - War and Peace - U.S. Tax Code
Any extracts used in the following article are for non-commercial research and educational purposes only and may be subject to copyright from their respective owners.
I’m writing this literature review at the suggestion of Disillusioned from X.
There is a link to the Bovaer reviews, here and here, in that both involve bovines.
In this case, the pathologies aren’t linked to toxic additives due to eco-quackery, but to contamination of DTaP vaccines with milk proteins. This isn’t novel or disputed by manufacturers, but it isn’t as widely discussed as it should be. In contrast, by now most of us are aware of adjuvant-related toxicities, such as those linked to aluminium or mercury.1
Bovine protein-related pathologies do not exclude other vaccine-related toxicologies—it’s all part of a wider problem that appears to be both insurmountable from an economically-viable process standpoint. It’s more of a feature than a bug, due to the lifelong illnesses that result. These require recurring expenditure to manage them.
Even today, more evidence emerges of this sick (pun intended) business model:
On another note, I published Bovaer Part 1 back in January, and I highlighted the hypocrisy of our esteemed leaders and how, whilst supposedly being concerned about the environment and cow farts, they were more obsessed with death and destruction.
With hindsight, my introduction was, if anything, too restrained.
Indeed, all four horses are now charging at us, full gallop:
If the Four Horsemen of the Apocalypse had a social media account, our esteemed leaders would be their paying subscribers, using them as role models and exchanging tips. They would meet up a few times a year, shake their skeletal arms, attend photocalls and make a few deals, after a cognac or three. (A sneak insight to what happens at Davos after hours? And have you ever seen a skeleton drink? I digress…)
Are we to believe that these people, who, judged by their actions, appear to worship conquest, war, famine and death and basically hate you, would these same people give a fig about climate change unless there was something in it for them? Whatever they get out of it, it’s certainly not going to be in your best interest, either now or in future.
Emphasis is mine in bold, and some passages are lightly reformatted for legibility.
2.1 What is a DTaP vaccine?
Diphtheria, tetanus, and pertussis (DTaP or Tdap) vaccines contain killed (inactivated) viruses and are given as a series of shots. They are administered to try to prevent disease, not to treat infections.
Diphtheria is a serious, transmissible infection of the throat that can block the airway and cause severe breathing problems.
Tetanus, otherwise known as lockjaw, is an infection that systemically affects the nervous system, leading to severe muscle spasms.
Pertussis (whooping cough) is a respiratory infection that leads to cold-like symptoms, severe coughing, and may lead to severe breathing problems.
Their relative efficacy at providing lifelong protection is outside the scope of this work, but, if you haven’t read them yet, I highly recommend adding these to your reading list:
There are many other great publications out there, too, and I wish I had room to link them all.
The KidsHealth site goes into some detail. Of course, it can’t help itself from repeating misinformation about vaccines and disease eradication. Note that TDaP is given during the second half of pregnancy, which makes me feel sick to the stomach, especially as it’s linked to folate pathogenicity.
The recommendation to administer acetaminophen is another red flag, as discussed here:
N.B. If you need this many doses, is it a vaccine or a prescription drug series?
… Children younger than 7 years old receive DTaP, and older children and adults receive Tdap (or sometimes Td, which only protects against tetanus and diphtheria).
When Do People Get the DTaP/Tdap Vaccine?
Kids get the DTaP immunizations as a series of 5 shots at ages:
2 months
4 months
6 months
15–18 months
4–6 years
They get Tdap vaccine (also called the adolescent booster dose) at ages 11 to 12. Older teens and adults who haven’t yet had a booster with pertussis coverage also should get it. (This is especially important for adults who will be around newborn babies, such as grandparents or other caregivers.) Then, boosters are recommended every 10 years with either Tdap or Td (only tetanus and diphtheria).
Pregnant women get the Tdap vaccine in the second half of each pregnancy, even if they’ve been vaccinated in the past. People who get a deep cut or severe burn may need to get a dose of DTaP, Tdap, or Td to prevent tetanus infection (depending on their age and when they got their last dose).
These vaccines can be given at the same time as other vaccines. DTaP is sometimes given on its own, and other times in combination (in the same shot) with other vaccines.
Why Are the DTaP and Tdap Vaccines Recommended?
Use of the DTaP and Tdap vaccines has virtually ended diphtheria and tetanus in childhood and has greatly reduced the number of pertussis cases.
What Are the Possible Side Effects of the DTaP and Tdap Vaccines?
The vaccines can cause mild side effects: fever; mild crankiness; tiredness; loss of appetite; vomiting (throwing up); and pain, redness, or swelling in the area where the shot was given.
The horrific “DTap scream”:
Rarely, a child may have a seizure, a very high fever, or uncontrollable crying after getting a vaccine. A rare reaction in older kids is swelling of the whole arm or leg where the shot was given. And as with any vaccine, there is a small risk of fainting, and a very small chance of an allergic reaction.
When to Delay or Avoid DTaP and Tdap Vaccines
Simple colds or other minor illnesses should not prevent vaccination. Your doctor might reschedule the vaccine if your child has a more serious illness.
Talk to your doctor about whether the vaccine is a good idea if your child has had any of the following:
a serious allergic reaction, or any allergic reaction after an earlier DTaP or Tdap shot
severe pain or swelling of a whole arm or leg after an earlier shot
a brain or nervous system problem, like coma or seizures
Guillain-Barré syndrome
Your doctor might give a partial vaccine or no vaccine, or may decide that the benefits of vaccinating your child outweigh the potential risks.
Caring for Your Child After DTaP and Tdap Vaccination
For pain or fever, check with your doctor to see if you can give either acetaminophenoribuprofen, and to find out the right dose.
A warm, damp cloth or a heating pad on the injection site may help reduce soreness, as can moving or using the arm or leg.
When Should I Call the Doctor?
Call your doctor if:
You aren’t sure whether the vaccine should be postponed or avoided. Children who have had certain problems with the DTaP vaccine usually can safely get the Td vaccine.
The Cleveland Clinic, ironically, calls it correctly when it advises you to contact a “poison control center” if you take too much.
When you see this many contraindications and side effects, it’s an indication that a medication may lead to unpredictable systemic side effects. Another red flag:
What should I tell my care team before I take this medication?
They need to know if you have any of these conditions:
Blood disorders, such as hemophilia
Fever or infection
Immune system problems
Neurologic disease
Seizures
An unusual or allergic reaction to other vaccines, latex, other medications, foods, dyes, or preservatives
Pregnant or trying to get pregnant
Breastfeeding
How should I use this medication?
This vaccine is injected into a muscle. It is given by your care team.
A copy of Vaccine Information Statements will be given before each vaccination. Be sure to read this information carefully each time. This sheet may change often.
Talk to your care team about the use of this medication in children. While the DTaP vaccine may be given to children as young as 6 weeks and the Tdap vaccine may be given to children as young as 10 years old, precautions do apply.
Overdosage: If you think you have taken too much of this medicine contact a poisoncontrol center or emergency room at once.
NOTE: This medicine is only for you. Do not share this medicine with others.
What if I miss a dose?
It is important not to miss your dose. Call your care team if you are unable to keep an appointment.
What may interact with this medication?
This medication may interact with the following:
Certain medications that prevent or treat blood clots, such as warfarin, enoxaparin, dalteparin
Immune globulin
Medications that lower your chance of fighting an infection, such as adalimumab, anakinra, infliximab
Medications to treat cancer
Steroid medications, such as prednisone or cortisone
This list may not describe all possible interactions. Give your health care provider a list of all the medicines, herbs, non-prescription drugs, or dietary supplements you use. Also tell them if you smoke, drink alcohol, or use illegal drugs. Some items may interact with your medicine.
What should I watch for while using this medication?
See your care team for all shots of this vaccine as directed.
Report any side effects to your care team right away.
This vaccine, like all vaccines, may not fully protect everyone.
What side effects may I notice from receiving this medication?
Side effects that you should report to your care team as soon as possible:
Allergic reactions—skin rash, itching, hives, swelling of the face, lips, tongue, or throat
Feeling faint or lightheaded
Side effects that usually do not require medical attention (report these to your care team if they continue or are bothersome):
Chills
Fever
General discomfort and fatigue
Headache
Joint pain
Muscle pain
Pain, redness, or irritation at injection site
This list may not describe all possible side effects. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
Also referred to as Autistic Spectrum Disorder, StatPearls describes it in this way:
… a neurodevelopmental condition characterized by significant and persistent challenges in social communication, social interaction, and the presence of restricted, repetitive behaviors, interests, or activities. These symptoms appear in early childhood and vary in severity, creating a heterogeneous presentation across individuals.
ASD affects critical areas of functioning, including social and occupational domains, and its impact is lifelong. Early recognition and intervention are essential to mitigate challenges, improve outcomes, and enhance the quality of life for individuals with ASD.
Diagnosis is challenging and is often made by elimination:
Symptoms must be present in the early developmental period (but may not fully manifest until social demands exceed limited capacities or may be masked by learned strategies in later life).
Symptoms cause clinically significant impairment in social, occupational, or other important areas of current functioning.
These disturbances are not better explained by intellectual developmental disorder (intellectual disability) or global developmental delay. Intellectual developmental disorder and ASD frequently co-occur. To make comorbid diagnoses of ASD and intellectual developmental disorder, social communication should be below that expected for the general developmental level.
An important aspect of the DSM-5-TR diagnostic criteria is the use of specifiers of current severity, level of intellectual impairment, level of language impairment, association with known genetic or medical conditions or environmental factors, and if comorbid catatonia is present, allowing the clinician to communicate a more detailed clinical description when diagnosing ASD.[1] See Image.
[Severity Specifiers for Autism Spectrum Disorder, Table.]
The diagnosis of ASD replaces a spectrum of conditions such as autistic disorder, Asperger disorder, and pervasive developmental disorder not otherwise specified that were previously diagnosed separately in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR).
According to the Centers for Disease Control and Prevention, 15% to 20% of theworld’s population exhibits some form of neurodivergence.[2] Neurodiversity refers to the diversity of minds and brains in the world, as each individual is unique, and there is no single “right” way of thinking.[3]
The term neurodiversity is often used for neurological and developmental conditions such as ASD, attention-deficit/hyperactivity disorder, and learning disabilities to describe non-pathological variations in the function of human brains. Neurodivergent individuals are frequently stigmatized and devalued. Neurodiversity embraces the concept that differences need not be viewed as deficits.[4]
Whether it’s due to the vaccine schedule, contaminants, adjuvants, glyphosate, or a combination of factors, cases have risen exponentially in the last forty years.
Better diagnosis can explain some of this, but from my experience of working with children on the spectrum, there is no doubting the diagnosis. I suspect that vaccine-induced encephalitis is behind a majority of cases.
I was expecting the research into folic acid (FA) and child development to be unequivocal by now, but this is not the case.
After all, the FDA mandated folic acid addition to enriched grain products some thirty years ago, and supplementation during our reproductive years has been described as “essential”. Women are strongly encouraged to take up to 400 µg of folic acid daily.23
Normally, during your first month of pregnancy, the two sides of the fetus’s spine join together to cover and protect the spinal cord, spinal nerves and meninges. At this point, the developing brain and spine are called the neural tube.
As growth continues, the top of the neural tube becomes the brain. The rest of the tube becomes the spinal cord. An NTD happens when this tube doesn’t close completely somewhere along its length.
Neural tube defects affect about 3,000 pregnancies each year in the United States.
Spina bifida is the most common type of neural tube defect (NTD). It happens when the neural tube doesn’t close completely somewhere along the spine during fetal development.
Types of spina bifida include:
Myelomeningocele (open spina bifida): This leads to a fluid-filled sac that sticks out from your baby’s back. It contains part of their spinal cord, meninges, nerves and cerebrospinal fluid (CSF).
Meningocele: This leads to a sac of fluid that sticks out through an opening in your baby’s back. But their spinal cord isn’t involved or damaged.
Spina bifida occulta: This creates a small gap in your baby’s spine. But there isn’t an opening or sac on their back. It’s the mildest form of spina bifida.
Anencephaly
Anencephaly happens when the fetus’s neural tube doesn’t close at the top. This causes the skull, scalp and brain not to develop properly. Portions of the brain and skull are missing. The brain tissue that does form is usually exposed because there isn’t enough skin and bone to cover it.
Infants with anencephaly are either stillborn or die soon after birth.
Encephalocele
Encephalocele happens when the neural tube doesn’t close near the brain. There’s also an opening in the skull. The fetus’s brain and the membranes that cover it can protrude through the skull, forming a sac-like bulge.
In some cases, there’s only a small opening in the nasal cavity or forehead area that’s not noticeable.
Iniencephaly
Iniencephaly happens when the spine is severely misshapen. It often causes a lack of a neck. The fetus’s head may be bent severely backward. The facial skin is connected to the chest. And the scalp is connected to the back.
From “Folic Acid Food Fortification—Its History, Effect, Concerns, and Future Directions“ (2011), by Crider et al.:
… The relationship between apparent folate deficiency and NTD occurrence was hypothesized as early as 1965 [7]. After a number of studies suggested that folic acid might reduce the risk of NTDs [8,9,10], a randomized control trial (RCT) to determine the effectiveness of folic acid supplementation in the prevention of the recurrence of NTDs was undertaken by the British Medical Research Council [11].
That RCT found that women with a previous history of a pregnancy affected by an NTD reduced their recurrence risk by 70% by taking 4000 micrograms (µg) of folic acid daily. The following year, in a Hungarian RCT, a 100% reduction in risk of a first occurrence of an NTD-affected pregnancy was found among women who took a prenatal vitamin containing 800 µg of folic acid daily [12].
In 1991, the Centers for Disease Control and Prevention recommended that women with a history of a prior NTD-affected pregnancy should consume 4000 µg of folic acid daily starting at the time they begin planning a pregnancy [13].
Subsequently, in 1992, the U.S. Public Health Service recommended that all women of childbearing age consume 400 µg of folic acid daily through fortification, supplementation, and diet to prevent NTDs [14].
In 1998, the Institute of Medicine (IOM) recommended that women capable of becoming pregnant should consume 400 µg of folic acid daily from fortified foods or supplements, or both, in addition to that obtained through a normal diet [15]. In 2009, the U.S. Preventive Services Task Force published updated guidelines that reinforced these recommendations [16].
Compliance with guidelines is challenging, and the temptation to use the big stick of mandation is always there:
Encouraging women to consume a supplement containing 400 µg of folic acid daily has limitations as a primary public health program. In the United States, up to 50% of all pregnancies are unplanned [17]. The neural tube closes early in embryonic development (28 days after conception), therefore a woman should begin folic acid supplementation ideally prior to becoming pregnant.
Education campaigns encouraging women to increase their use of supplements have not been effective at reaching every high-risk population [18].
To compound the problem, a recent UK cohort study showed that women planning a pregnancy only marginally increased their compliance with health behaviors and folic acid supplement use [19].
Other countries have recommendations to prevent NTDs by improving diet or encouraging supplement use, or both, but do not have mandatory fortification programs.
An evaluation of NTD trends in such countries has revealed no significant changes since recommendations were enacted [20]. It has been suggested that well-implemented mandatory fortification programs, unlike voluntary fortification programs, might help reduce disparities [21].
Given these issues, mandatory fortification programs have been implemented in many countries to maximize their effects and reduce the high costs associated with prevention programs such as education campaigns and other interventions that require behavioral change [22].
Mandatory fortification is, of course, coming to Herr Starmer’s Britain this December. That is, if there is anything left after he keeps provoking retaliation from Russia and Iran.
He’s like an annoying chihuahua that keeps trying to bite bigger dogs in the neighbourhood.
Folic acid is to be added to non-wholemeal wheat flour in the UK to help prevent birth defects.
Adding folic acid to flour could prevent around 200 cases of neural tube defects, such as spina bifida, every year, and improve the health of pregnant women, says the government, which is giving manufacturers until the end of 2026 to conform to the new legal requirement, external.
Expectant mothers and women trying to conceive should continue to take supplementary folic acid - the synthetic version of the vitamin folate - as currently advised by medical practioners.
Folic acid is particularly important in early pregnancy, aiding proper development of the baby’s brain, skull and spinal cord.
Experts, many of whom have called for the move for a number of years, have welcomed the government’s decision.
The announcement follows health improvements in other countries, such as Australia and Canada, where the practice is already carried out.
Enough is never enough for the hard-of-thinking:
Some say the change doesn’t go far enough, however, and more foods should be included.
Prof Neena Modi, professor of neonatal medicine at Imperial College London, said: “This will disadvantage groups such as women who are sensitive to gluten, eat rice in preference to bread, and products made from wholemeal flour - excluding them and their babies from benefiting, and thus adding to the considerable health inequities that already exist in the UK.”
The vitamin folate, also known as vitamin B9, is found in everyday foods such as beans and some green vegetables, meaning most people receive a sufficient dose from eating a regular, healthy diet.
In addition, the NHS recommends women who are trying for a baby take folic acid supplements for approximately three months before getting pregnant, and for at least 12 weeks after becoming pregnant. This recommendation will remain in place.
But, as is often the case in biochem, it’s not that simple:
FOLATE ACTION IN NERVOUS SYSTEM DEVELOPMENT AND DISEASE (2018)
… For more than 50 years epidemiological studies have demonstrated that periconceptional folate supplementation reduces the occurrence of one of the most common serious birth defects, called neural tube defects (NTDs).
… Strikingly, detailed understanding of the mechanisms of folate action during neural tube formation has remained elusive. Folate belongs to the vitamin B family and it participates in methylation reactions such as those necessary for nucleotide synthesis. Hence, folate supports rapid growth by enabling DNA synthesis in proliferating cells.
On the other hand, in other vertebrates like Xenopus laevis, the necessity for cell divisions during neural tube formation has been ruled out by demonstrating that blocking DNA synthesis does not interfere with neurulation (Harris and Hartenstein, 1991).
Nevertheless, folate action is necessary during Xenopus laevis neural tube formation, as recently demonstrated by our study (Balashova et al., 2017), suggesting that folate might play additional functions during neural tube formation besides its role as a vitamin for DNA synthesis.
Similarly, mutations in folate uptake systems have been reported in families with higher incidence of NTDs than the general population, including 2 SNPs in FOLR1 (O’Byrne et al., 2010).
These studies strongly indicate that folate acts as an essential regulator of neural tube morphogenesis, probably independent of nucleotide synthesis.
Here, we review the findings that address the role of folate in the development of the nervous system and folate’s effects on neural function and repair. These studies argue for specialized functions of folate in neural tissue and propose new questions that require further investigation to be answered on the mechanisms of folate action in nervous system development, disease and regeneration.
If you are deficient in other vitamins and minerals or have a genetic mutation that is associated with deficiency, then just popping a pill each day is not necessarily going to prevent birth defects.
I recommend this Substack, and Jennifer has written much more about the subject than I can cover here:
Prenatal folate and folic acid levels; NTDs, a multifactorial problem.
… Based on my review of nutrients involved in NTD risk - a well written study would need to evaluate all of the prenatal participants not only for folic acid, but also for their level of methyl folate and methyl/hydroxy B12 (is the active form present or only cyanocobalamin?), choline, vitamins B2, and B6, zinc, betaine (TMG), Dimethylglycine, and whether there is elevated homocysteine. Purine Nucleotides availability and Iron and iodine might also have impact if deficient. (Substack) An addition - cholesterol blocking drugs are likely a risk of NTDS if a premenopausal woman becomes pregnant while taking statin drugs or a newer medication affecting cholesterol metabolism (PCSK9 inhibitor). (Husten, 2016)
Multifactorial problems are complex to study because of the multiple potential causal variables. Promising someone a reduced Neural Tube Defect risk in their infant if they take a 400 or 600 mcg supplement of folic acid or active methyl folate will not guarantee that desirable outcome if the person is also low in other B vitamins and zinc or have reduced cholesterol sulfate availability.
Lack or excess of active forms of vitamin A or D could also interfere with fetal cholesterol metabolism in a way that may cause NTDs.
Mass medicating the population through fortification of food staples is not a risk-free exercise, and too much folic acid can also be harmful, especially if it’s taken without a proportionate amount of B12:
Folate, vitamin B12, one carbon metabolism and the nervous system: Excess folic acid is potentially harmful (2025)
Highlights
• Folate and vitamin B12 metabolism are fundamental to CNS development and health.
• The balance between folate and vitamin B12 is crucial to methylation, genetics and epigenetics.
• Both folate deficiency and excess are potentially harmful to the nervous system.
• Folate excess increases the demand for vitamin B12.
• The safe UL for folic acid should be reconsidered, including in fortification policies.
Abstract
Folate, vitamin B12 and one carbon metabolism are fundamental to genetics and epigenetics, and to nervous system development and brain health at all ages. The neuropsychiatric complications of deficiency or inborn errors of folate and vitamin B12 are well documented but there has been controversy about whether excess folic acid is also harmful to the nervous system, especially in the presence of vitamin B12 deficiency.
There is now substantial and consistent clinical, epidemiological and experimental evidence that excess folic acid is potentially harmful to the nervous system. Recent experimental evidence confirms that both folate deficiency and excess impair cortical neurogenesisand is greatest when vitamin B12 deficiency is combined with excess folic acid.
Excess folic acid increases the demand for vitamin B12 and aggravates the block in the folate cycle resulting from vitamin B12 deficiency. The balance between folate and vitamin B12 is crucial to methylation and to genetics and epigenetics.
Both folate deficiency and excess may impair cellular differentiation and nervous system development by hypomethylation or hypermethylation of genes. In countries with folic acid fortification policies many subjects are exposed to excess folate.
The long term genetic, epigenetic and transgenerational implications are yet to be clarified. The safe UL of folic acid should be reconsidered in relation to the vitamin B12 status of individuals and populations.
The combination of a natural folate together with vitamin B12 would greatly improve the benefits and reduce the harms of current fortification policies.
Folic acid administered by supplementation or fortification is not the same as the vitamin folate.
Both are B vitamins. Natural B9 occurs in foods like leafy greens, legumes, and citrus.
Natural B9, folate, has higher bioavailability. Folate is converted to its active form (5-MTHF) in the intestines, whereas the liver has to process the synthetic form. Conversion is a slower, more complex process.
… Depending on a person’s alleles, some supplements may be really critically helpful and others harmful - balanced function throughout the methylation cycles is the goal for restoring function for people on the autism spectrum or for people with symptoms of heart disease
… Folic acid competes with natural folate for people who can’t remethylate the inactive folic acid easily. This was somewhat confirmed in a prenatal study which showed: “#Supplementation w/ (6S)-5-MTHF appears as effective as #folic acid in maintaining #folate status while [decreasing] unmetabolized folic acid in #maternal plasma” J.P. Fanton (twitter.com/HealthyFellow) (Cochrane, et al., 2023
From: “Methylation cycle gene differences as a cause of heart disease, Dr. James Roberts.” (2023)
From: “Folate, folic acid and 5-methyltetrahydrofolate are not the same thing“ (2014), by Scaglione & Panzavolta:4
… 1. Folate, an essential micronutrient, is a critical cofactor in one-carbon metabolism. Mammals cannot synthesize folate and depend on supplementation to maintain normal levels. Low folate status may be caused by low dietary intake, poor absorption of ingested folate and alteration of folate metabolism due to genetic defects or drug interactions.
2. Folate deficiency has been linked with an increased risk of neural tube defects, cardiovascular disease, cancer and cognitive dysfunction. Most countries have established recommended intakes of folate through folic acid supplements or fortified foods.
External supplementation of folate may occur as folic acid, folinic acid or 5-methyltetrahydrofolate (5-MTHF).
3. Naturally occurring 5-MTHF has important advantages over synthetic folic acid – it is well absorbed even when gastrointestinal pH is altered and its bioavailability is not affected by metabolic defects.
Using 5-MTHF instead of folic acid reduces the potential for masking haematological symptoms of vitamin B12 deficiency, reduces interactions with drugs that inhibit dihydrofolate reductase and overcomes metabolic defects caused by methylenetetrahydrofolate reductase polymorphism. Use of 5-MTHF also prevents the potential negative effects of unconverted folic acid in the peripheral circulation.
There is evidence that, in many cases, fortification may not even work that well at improving public health. As with folic acid without B12, it can even have the opposite effect to that intended.
HICs: High-income countries.
LMICs: Low‑ and middle‑income countries.
Food Fortification: The Advantages, Disadvantages and Lessons from Sight and Life Programs (2021)
… Despite the enormous benefits of food fortification strategies on nutritional status, some studies have identified opposite results in terms of no impact of food fortification programs and of guaranteeing safe upper limits.
For example, a study conducted among Brazilian children under the age of six found no effect of iron-fortified flour on anemia prevalence. The study consisted of four population-based surveys conducted over a four-year period, and it measured dietary intake and hemoglobin levels.
The findings showed an unexpectedincrease in anemia among children. Despite the average intake of fortified flour detected by the study amounting to 100 g per day, the poor diets quality of children with low bioavailability of iron compromised the benefits of fortified flour [41].
Furthermore, a systematic review performed in both HICs and LIMCs did not find any significant association between the effect of multiple micronutrient fortification on child growth outcomes such height/length-for-age z-score (HAZ/LAZ)) (MD 0.09, 95% CI 0.01 to 0.18; 8 studies, 2889 participants; low-quality evidence) and zinc deficiency (RR 0.84, 95% CI 0.65 to 1.08; 5 studies, 1490 participants; low-quality evidence) [20].
Fortified complementary foods had a small effect on children’s anemia but had no impact on their growth and in some cases, they were associated with more diarrhea episodes [42].
A research paper from 2024 by Wells et al. discusses how autoimmune antibodies to the folate receptor may contribute to ASD in the newborn.
Key takeaways from “Folate Receptor Alpha Autoantibodies in the Pediatric Acute-Onset Neuropsychiatric Syndrome (PANS) and Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS) Population“: 5
The folate receptor alpha autoantibodies (FRAAs) are associated with cerebral folate deficiency (CFD) and autism spectrum disorder (ASD). Both of these syndromes have overlapping characteristics with Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS) and Pediatric Acute-Onset Neuropsychiatric Syndrome (PANS).
Thus, we propose that the FRAAs may contribute to the symptomatology of PANS/PANDAS. To test this hypothesis, 1 mL of serum from 47 patients (age range = 6–18 years old) clinically diagnosed with PANS/PANDAS was sent to Vascular Strategies (Plymouth Meeting, PA, USA) for analysis of FRAAs.
Moreover, 63.8% of PANS/PANDAS patients (male = 15; female = 15) were found to have either the blocking and/or blinding FRAAs, with 25 (83.3%; male = 14; female = 11) having binding FRAAs, two (6.7%; all female = 2) having blocking FRAAs, and 3 (10%; male = 1; female = 2) having both binding and blocking.
“Surprisingly”—one of my favourite words to see in a paper.
In this case, it’s because the authors unexpectedly found a significant correlation between ASD and how weakly folate binds to the folate receptor alpha (FRɑ), whereas severe tics were associated with a higher binding titre.
Furthermore, surprisingly, ASD was associated with a 0.76 lower binding titer (p = 0.02), and severe tics were associated with a 0.90 higher binding titer (p = 0.01).
Leucovorin is also known as folinic acid. Both this and synthetic folic acid are distinct types of vitamin B9, but they differ in that bioconversion follows different metabolic pathways.
Folinic acid is a pre-activated, reduced, bioavailable form of B9 that doesn’t require the liver’s MTHFR enzyme to become effective. This means that it can bypass genetic MTHFR metabolic blocks or manage toxicity from medications like methotrexate.6
MTHFR gene
methylenetetrahydrofolate reductase
The MTHFR gene provides instructions for making an enzyme called methylenetetrahydrofolate reductase. This enzyme plays a role in processing amino acids, the building blocks of proteins.
Methylenetetrahydrofolate reductase is important for a chemical reaction involving the vitamin folate (also called vitamin B9).
Specifically, this enzyme converts a form of folate called 5,10-methylenetetrahydrofolate to a different form of folate called 5-methyltetrahydrofolate.
This is the primary form of folate found in blood, and is necessary for the multistep process that converts the amino acid homocysteine to another amino acid, methionine. The body uses methionine to make proteins and other important compounds.
There is an obvious mnemonic to use for the MTHFR gene, but I will leave that to your imagination.
A case of a FRAA-positive patient is provided to illustrate that a treatment plan including leucovorin can result in symptom improvement in patients with PANS/PANDAS who are FRAA-positive. These data, for the first time, demonstrate that PANS/PANDAS is associated with FRAAs and suggest folate metabolism abnormalities may contribute to PANS/PANDAS symptomatology. Further studies investigating the therapeutic nature of leucovorin in the treatment of PANS/PANDAS are needed.
Another case where a clinical test cannot identify localised deficiencies, and you may test normal despite being deficient in a critical location:
In patients with CFD, normal levels of 5-methyltetrahydrofolate (5MTHF) are found in serum despite below-normal concentrations of 5-methyltetrahydrofolate (5MTHF) in the cerebrospinal fluid (CSF) [15,16].
This is caused by dysfunction of the folate receptor alpha (FRɑ), the main transporter of folate into the brain [16].
In healthy conditions, folate binds to the FRɑ, which then undergoes endocytosis to actively transport folate across the blood–brain barrier.
One of the main causes of FRɑ dysfunction are FRɑ autoantibodies (FRAAs), which bind to the FRɑ and inhibit folate transport into the CSF [6,17].
There are two kinds of autoantibodies of interest, and both stop the folate receptor from binding correctly:
Two FRAAs have been described, i.e., the blocking and binding FRAAs. The blocking FRAA binds specifically to the site where folate binds to the FRα, thereby preventing folate from binding to the FRɑ, while the binding FRAA binds to other regions of the FRɑ and interferes with its ability to function optimally.
To determine the presence of CFD, standard practice utilizes lumbar punctures to measure the 5MTHF concentration in the CSF. Since the lumbar puncture is invasive [12] and generally requires a general anesthetic [14], it has become common practice to measure FRAAs using the folate receptor autoantibody test (FRAT).
Studies suggest that central folate abnormalities play an essential role in the pathogenesis and exacerbation of ASD [12,17].
Successful treatment of CFD and FRAA-positive ASD patients provides a basis for believing that central folate abnormalities are a treatable condition. Similar to ASD, it is believed that the etiology of the majority of PANS/PANDAS cases includes triggers from environmental factors, including factors that induce the production of FRAAs [17].
Although correlation doesn’t equal causation, if this has been confirmed, then it should be shouted from the rooftops:
A meta-analysis estimates the prevalence of FRAAs in ASD to be 71% [11]. Leucovorin treatment (folinic acid) in FRAA-positive ASD patients results in improvements in ASD symptoms, including speech, communication, and repetitive behaviors [18].
Based on the overlap between PANS/PANDAS symptoms and CFD/ASD, such as repetitive behaviors, tics, depression, neurodevelopmental regression, and speech disfluency, we propose that FRAAs may play a role in the symptomatology of PANS/PANDAS.
Note: “Refractory to treatment” means a disease or condition does not respond to initial or standard therapies, remaining stubbornly persistent.
If FRAAs were found in patients with PANS/PANDAS, leucovorin or other reduced folate may provide symptomatic relief for many of the symptoms that often remain refractory to treatment.
3.2. Prevalence of FRAAs
As seen in Figure 1, out of 47 patients, 30 individuals (63.8%; male = 15; female = 15) had folate receptor autoantibodies in their serum, while 17 individuals (36.2%; male = 14; female = 3) did not have any autoantibodies in their serum.
Of the 30 patients with autoantibodies, 25 (83.3%; male = 14; female = 11) patients had binding autoantibodies, two (6.7%; male = 0; female = 2) patients had blocking autoantibodies, and three (10%; male = 1; female = 2) had both binding and blocking autoantibodies.
Figure 1. Prevalence of folate receptor alpha antibodies in patients. (a) Positive or negative status of all study participants. (b) Prevalence of specific FRAA for those that were FRAA positive. Double+ signifies positivity for both blocking and binding FRAA.
3.3. Association of Symptoms with FRAAs
The presence or absence of ASD was found to be significantly related to the binding FRAA, such that the presence of ASD was more likely to be associated with a lower binding FRAA [Χ2 (1) = 8.67, p < 0.01; OR = 0.13 (0.01, 0.93)].
Tics were also found to be significantly related to the binding of FRAA, such that those having tics were more likely to have a high FRAA binding titer [Χ2 (1) = 6.24, p = 0.01; OR = 3.53 (2.97, 4.20)].
For tics, this was most significant for severe tics [Χ2 (1) = 18.62, p < 0.001 OR = 13.1 (4.01, 42.52)] and borderline significant for moderate tics [Χ2 (1) = 3.29, p = 0.07; OR = 2.16 (0.93, 5.01)].
The authors provide a case report from their clinic. The results were remarkable.
GAS: Group A Streptococcal infection.
3.4. Case Study of a FRAA-Positive PANS Patient
An 18-year-old male was previously diagnosed with PANS and autoimmune encephalitis at 13 years of age due to a sudden onset of anxiety, refusing to go to school, frequent urination, OCD, and repeated strep infections.
Antibiotic treatment for GAS resulted in a 30% improvement in symptoms. IVIG treatment resulted in a 60–70% improvement in symptoms. Symptoms were manageable for several years with prophylactic antibiotics.
The patient then developed mycoplasma pneumonia, resulting in an exacerbation of anxiety and OCD. Plasmapheresis decreased mycoplasma titers, but the titers remained elevated.
Two years later, he developed an Epstein-Barr virus (EBV) infection, which was treated with antivirals and other supplements. Since then, he has been unable to tolerate interventions such as antibiotics, herbals, and supplements due to negative reactions and continued to experience severe anxiety and OCD.
Other interventions included cognitive behavioral therapy, antipsychotics, and selective serotonin reuptake inhibitor medications.
He also had a defective gene for the folic acid-converting MTHFR enzyme, as well as a pan-nutritional inadequacy. These probably contributed to the persistent mycoplasma infection.
Important findings from laboratory work included persistent mycoplasma IgG, IgM, and MTHFRC677T homozygous defects, as well as low normal levels of vitamin D (32) and vitamin A (30), IgG subclass 2 (118), red blood cell (RBC), magnesium (3.8), and RBC zinc (7.67).
Interventions tried without improvements in symptoms included antivirals, immune, mitochondrial, and metabolic support. Vitamins D and A, zinc, and magnesium were added to treat mild deficiencies.
The patient also had a positive binding FRAA autoantibody. To address this, leucovorin (5 mg/day) was added. The patient was instructed to increase leucovorin weekly by 1 pill (5 mg) up to 30 mg per day (6 pills per day) as tolerated and helpful. Additionally, further antimicrobials were prescribed to treat mycoplasma. However, the patient did not take them due to a past history of symptom exacerbations.
Upon implementation of the above, OCD and anxiety improved by 50%, and daily function improved by 70%.
Dreams were no longer obsessive, his ability to take care of hygiene improved, and his personality started to come back, but social anxiety persisted.
After further implementation of leucovorin and despite persistent mycoplasma titers and no antimicrobial therapy, the patient’s symptoms improved by 90%.
One of the Bradford Hill criteria (experimental evidence/cessation of exposure):
He noted that when he neglected to take his leucovorin, his anxiety and OCD symptoms worsened.
With leucovorin treatment, the patient is currently excelling academically at a four-year university with honors, has friends, enjoys multiple hobbies, lives independently, and no longer experiences significant social anxiety or OCD.
Dissillusioned also had an equally positive outcome:
PINK1 is a gene that works with Parkin to maintain mitochondrial health via mitophagy—the identification and removal of damaged mitochondria. PINK1 acts as a detector, and Parkin does the removal:
Biochemical and genetic studies reveal that the products of two genes that are mutated in autosomal recessive Parkinsonism, PINK1 and Parkin, normally work together in the same pathway to govern mitochondrial quality control, bolstering previous evidence that mitochondrial damage is involved in Parkinson's disease.
PINK1 accumulates on the outer membrane of damaged mitochondria, activates Parkin's E3 ubiquitin ligase activity and recruits Parkin to the dysfunctional mitochondrion. Then, Parkin ubiquitinates outer mitochondrial membrane proteins to trigger selective autophagy.
From: “The Roles of PINK1, Parkin and Mitochondrial Fidelity in Parkinson’s Disease” (2016)
I’m sure that Dissillusioned already made the connection, but I always like to cross-reference studies, as we often find that metabolic pathways intersect in biochemistry. It’s why many allopathic drugs lose efficacy or induce unexpected side effects.
We can thank a study of fruit flies (Drosophila) for linking PINK1 and PARKIN gene mutations to folic acid-associated metabolic pathways and disease.
Exogenous administration of folic acid helped to restore mitophagy and protective one-carbon metabolism:
Some autosomal recessive forms of Parkinson's (PD) disease are caused by mutations in PINK1 or PARKIN, two genes involved in mitochondrial quality control (reviewed in Celardo et al.4).
In Drosophila melanogaster, mutations in either pink1 or parkin cause mitochondrial dysfunction linked to the accumulation of defective organelles. Studies in this fly model showed that mitochondrial stress in pink1 mutant results in the transcriptional activation of mitochondrial folate-mediated one-carbon metabolism genes as a protective response through an unknown mechanism.5
Folate one-carbon metabolism shuttles one-carbon units for biosynthetic pathways, including nucleotide biosynthesis and methylation reactions.
Enhancing one-carbon metabolism by exogenous administration of folic acid rescued mitochondrial defects in both flies and cultured human cells.5
The mitochondrial one-carbon metabolism was remodelled following mitochondrial dysfunction caused by defects in the replication of mitochondrial DNA (mtDNA) in mice.6
From “dATF4 regulation of mitochondrial folate-mediated one-carbon metabolism is neuroprotective” (2017)
It was thought that folate receptor alpha (FRα) only acted as a folate transporter, but research from 2017 found that it also acts as a transcription factor (TF). In other words, FRα regulates gene expression by binding to specific DNA sequences:
Folate receptor alpha is more than just a folate transporter (2017)
… a novel role of FRα as a transcription factor was reported by our lab. More recently our lab showed a novel pleiotropic role of FRα: (a) direct transcriptional activation of Oct4, Sox2, and Klf4 genes; and (b) repression of biogenesis of miRNAs that target these genes or their effector molecules.
These observations beg a question: “Can a simple molecule such as folate be used to manipulate the production and/or differentiation of endogenous neural stem cells (NSCs), which may hold promise for future therapies?”
Conditions such as spinal cord injury, motor neuron diseases, Alzheimer's disease and multiple sclerosis may benefit from increasing stem cell pool and promoting specific pathways of differentiation.
On the flip-side, these NSCs may also contribute to some CNS tumors therefore promoting differentiation could prove more beneficial. FRα may hold promises for both since it has the potential to remodel chromatin in a context dependent manner.
These genes and microRNAs (miRNAs) all play a key part in neurogenesis and embryonic development:
OCT4
Stem cell maintenance and regulation of differentiation is a key aspect to neuronal generation during both embryonic development and in adulthood. An improved understanding of the stem cell microenvironment to be targeted by exogenous stimulators such as folate is critical for our ability to predict responses of endogenous cells to drugs or biologicals.
Our recent work has demonstrated folate’s ability, via the receptor protein folate receptor alpha (FRα), to regulate expression of genes such as Hes1, Oct4, Sox2, Klf4, and TRIM71, which all work to maintain the stem cell pool.5,6
KDM6B
Earlier we7 showed that folate downregulates the miRNAs (miR-138, miR-148a, miR-185, miR-339-5p) which target H3K27 demethylase KDM6B levels, indirectly upregulating KDM6B and decreasing the methylation on H3K27.
KDM6B was associated with Hes1 promoter during cell proliferative stages (E10.5) and Neurog2 promoters at the start of neurogenesis (E12.5) during murine embryonic development.
Park and colleagues8 showed that KDM6B activation is required for post-natal and adult neurogenesis.
Referenced previously, Ramaekers et al. (2007) found a significant correlation between ASD and folate receptor autoimmune antibodies.
Folinic acid supplementation led to normal CSF 5MTHF and partial or complete clinical recovery after 12 months:
Folate receptor autoimmunity and cerebral folate deficiency in low-functioning autism with neurological deficits
Abstract
Reduced folate transport to the CNS was identified in two autism spectrum disorders, i.e., Rett syndrome and infantile low-functioning autism with neurological abnormalities.
Twenty-five patients with early-onset low-functioning autism with or without neurological deficits, were evaluated for serum folate, cerebrospinal fluid (CSF) 5-methyltetrahydrofolate (5MTHF), and serum FR autoantibodies of the blocking type to determine the significance of folate receptor (FR) autoantibodies with respect to folate transport across the blood-CSF barrier.
In spite of normal serum folate, CSF 5MTHF was low in 23 of 25 patients. The reduced CSF folate in 19 of these 23 patients could be explained by serum FR autoantibodies blocking the folate binding site of the membrane-attached FR on the choroid epithelial cells.
Oral folinic acid supplements led to normal CSF 5MTHF and partial or complete clinical recovery after 12 months. Serum FR autoimmunity appears to represent an important factor in the pathogenesis of reduced folate transport to the nervous system among children with early-onset low-functioning autism associated with or without neurological deficits.
Early detection of FR autoantibodies may be a key factor in the prevention and therapeutic intervention among this subgroup of patients with autism.
The NHS’s Big Pharma sponsors cannot profit from this, but they can from sales of drugs such as the stimulant Ritalin (methylphenidate), which are commonly used to treat patients with ASD and attention-deficit/hyperactivity disorder (ADHD).
Note: 50-70% of individuals with ASD also have ADHD.7
Methylphenidate is a widely used medication for treating attention deficit hyperactivity disorder (ADHD) and narcolepsy. The Methylphenidate Market is expected to grow from USD 2 Billion in 2023 to USD 2.5 Billion by 2031, at a CAGR of 1.84% during the forecast period.
Alternative drugs, such as Concerta, Vyvanse, Adderall, Atomoxetine, Viloxazine, Guanfacine, Modafinil, and Armodafinil, further help to ring the cash register.
Returning to the Willie Sutton rule for following the money, there is no incentive to promote cheap and effective alternatives:
ADHD Therapeutics Market Report Scope & Overview:
TheADHD Therapeutics Marketsize is valued at USD 14.96 Billionin 2025 and is expected to reach USD 23.89 Billionby 2035 and grow at a CAGR of 4.80% over the forecast period 2026-2035.
The ADHD Therapeutics market is anticipated to witness significant growth due to the increasing prevalence and diagnosis of attention deficit hyperactivity disorder across children, adolescents, and adults worldwide.
Rising awareness of mental health conditions, improved access to psychiatric care, and expanding treatment acceptance are encouraging the adoption of both stimulant and non-stimulant medications.
Advancements in long-acting drug formulations, personalized treatment approaches, and the integration of behavioral and cognitive therapies are improving treatment effectiveness and patient adherence.
According to industry studies, over 70% of ADHD Therapeutics demand is driven by stimulant medications, fueled by their high clinical effectiveness, rapid symptom control, and widespread prescription for managing attention deficit hyperactivity disorder across children, adolescents, and adults.
A 58-year-old woman developed a severe autoimmune cerebral folate deficiency.
Once again, serum levels of folate were normal, but her CSF was deficient in 5-methyltetrahydrofolate (5MTHF), as well as tetrahydrobiopterin (BH4).
BH4 is an essential enzyme cofactor that enables the metabolism of phenylalanine and the synthesis of key neurotransmitters, including serotonin, dopamine, norepinephrine, and nitric oxide.
She had a history of rheumatoid arthritis (RA) and migraines.
There is a link between folate deficiency and a higher risk of migraine, due to elevated levels of the pro-inflammatory amino acid homocysteine.8
With RA, folate deficiency is often exacerbated by methotrexate (MTX) treatment, which acts as a folate antagonist. Elevated homocysteine also contributes to chronic inflammation.9
Adult-Onset Cerebral Folate Deficiency (2012)
Abstract
Objective To report new manifestations of cerebral folate deficiency, a rare metabolic autoimmune syndrome, in an adult.
Design Case report.
Setting University teaching hospital.
Patient A 58-year-old woman with progressive memory loss and myoclonus presented for medical attention. Results of cerebral spinal fluid analysis showed low levels of tetrahydrobiopterin and 5-methyltetrahydrofolate. The patient’s serum folate level was normal. Serum contained folate receptor 1 blocking and binding antibodies.
Results The patient was treated successfully with folinic acid supplementation, and after 6 months of treatment, clinical symptoms had resolved.
Conclusions To our knowledge, we report the first case of adult-onset cerebral folate deficiency. Furthermore, this condition could represent a treatable form of early-onset dementia.
Typical autoimmune cerebral folate deficiency is characterized by normal early development followed by abrupt neurological regression. At approximately 4 months, affected children develop marked irritability, decelerated head growth, psychomotor retardation, ataxia, spasticity, dyskinesia (choreoathetosis and ballismus), visual loss, hearing loss, and myoclonic epilepsy.
Report of a case
A 58-year-old woman presented to the neurology clinic at The University of Texas at Houston, with progressive memory loss and myoclonus. The myoclonus consisted of brief jerks to the arms and legs that did not result in disability. She had a history of rheumatoid arthritis and migraine headaches.
On physical examination, no neurological deficits other than mild myoclonus and impairment of short-term recall (formal neurocognitive testing was not performed) were noted.
Results of cerebrospinal fluid (CSF) analysis showed low levels of tetrahydrobiopterin (8 nmol/L; reference, 10-30 nmol/L) and 5-methyltetrahydrofolate (29 nmol/L; reference, 40-120 nmol/L).
The patient’s serum folate level was normal (20.4 ng/mL; reference, >5.4 ng/mL [to convert to nanomoles per liter, multiply by 2.266]). Serum contained a folate receptor 1–blocking antibody titer of 0.41 pmol/mL (reference, <0.2 ML/mL) and an folate receptor 1–binding antibody titer of 0.81 ML IgG/mL (reference, <0.5 ML IgG/mL).
Our patient was treated successfully with folinic acid (25 mg/d), a stable form of metabolically active reduced folate that can access the CSF by the alternate folate carrier receptor.1
After 6 months of treatment, a second CSF 5-methyltetrahydrofolate level was 68 nmol/L (reference, 40-120 nmol/L), and clinical symptoms had resolved.
Comment
Folate is essential for the formation of biogenic amines and pterins in the central nervous system. Folate deficiency produces a variety of neurologic symptoms, including neuropsychiatric disturbances and movement disorders. In healthy adults, CSF folate levels do not decline with age,1 but CSF folate levels have been found to be lower in patients with late-onset Alzheimer disease than in age-matched control subjects.1
Folate is absorbed into the bloodstream via the gastrointestinal tract. In the bloodstream, folate binds to the folate receptor 1 on the basolateral endothelial surface of the choroid plexus. Through receptor-mediated endocytosis, folate is then transported across the blood-brain barrier into the CSF. Binding of the folate receptor 1 autoantibody to this receptor blocks the ability of the receptor to bind and transport folate.2
Classic autoimmune cerebral folate deficiency is characterized by normal early development followed by abrupt neurological regression. At approximately 4 months, children develop marked irritability, decelerated head growth, psychomotor retardation, ataxia, spasticity, dyskinesia (choreoathetosis and ballismus), visual loss, hearing loss, and myoclonic epilepsy.3,4
The NHS remains ignorant of an accepted treatment protocol:
Treatment is with reduced folate in the form of folinic acid. Dose is titrated to maintain normal CSF 5-methyltetrahydrofolate levels. The optimal length of treatment is unknown.
Another case study should have helped to raise awareness, instead of reaching for the Ritalin bottle:
A recent case report described a 15-year-old girl with cerebral folate deficiency and rheumatoid arthritis and no history of developmental abnormalities.5 The current case reported herein further defines the syndrome of autoimmune cerebral folate deficiency to include adult onset presenting with symptoms of dementia and myoclonus.
This case highlights the importance for clinicians to consider CSF analysis, including 5-methyltetrahydrofolate levels, in all patients with a history of autoimmune disease and dementia.
A study from 2023 by Bobrowski-Khoury et al. using rats helped to confirm the hypothesis and the preferential administration of folinic acid over other forms of vitamin B9.
If you are going to mandate medications for the public, perhaps folinic acid fortification might be the better choice? This might explain the lack of opposition to the inclusion of the synthetic form by Big Pharma, as it lacks treatment value for individuals who would truly benefit.
It’s difficult to be too critical of their business model. If folinic acid fortification were mandated, then the parties involved in the decision would never hear the end of it.
Key takeaways from “Brain Uptake of Folate Forms in the Presence of Folate Receptor Alpha Antibodies in Young Rats: Folate and Antibody Distribution“10
In a rat model, following exposure to rat folate receptor alpha antibodies (FRαAb) during gestation, FRαAb accumulates in the placenta and the fetus and blocks folate transport to the fetal brain and produces behavioral deficits in the offspring.
These deficits could be prevented with folinic acid. Therefore, we sought to evaluate folate transport to the brain in young rat pups and determine what effect FRαAb has on this process, to better understand the folate receptor autoimmune disorder associated with cerebral folate deficiency (CFD) in autism spectrum disorders (ASD).
When injected intraperitoneally (IP), FRαAb localizes to the choroid plexus and blood vessels including the capillaries throughout the brain parenchyma.
Biotin-tagged folic acid shows distribution in the white matter tracts in the cerebrum and cerebellum. Since these antibodies can block folate transport to the brain, we orally administered various folate forms to identify the form that is better-absorbed and transported to the brain and is most effective in restoring cerebral folate status in the presence of FRαAb.
The three forms of folate, namely folic acid, D,L-folinic acid and levofolinate, are converted to methylfolate while L-methylfolate is absorbed as such and all are efficiently distributed to the brain.
However, significantly higher folate concentration is seen in the cerebrum and cerebellum with levofolinate in the presence or absence of FRαAb.
Our results in the rat model support testing levofolinate to treat CFD in children with ASD.
Graphical Abstract
A further study, from 2012, also supported the link between FR autoAbs and ASD:
Cerebral folate receptor autoantibodies in autism spectrum disorder
… In this study, serum FRA concentrations were measured in 93 children with ASD and a high prevalence (75.3%) of FRAs was found. In 16 children, the concentration of blocking FRA significantly correlated with cerebrospinal fluid 5-methyltetrahydrofolate concentrations, which were below the normative mean in every case.
Children with FRAs were treated with oral leucovorin calcium (2 mg kg−1 per day; maximum 50 mg per day). Treatment response was measured and compared with a wait-list control group.
Compared with controls, significantly higher improvement ratings were observed in treated children over a mean period of 4 months in verbal communication, receptive and expressive language, attention and stereotypical behavior.
We know from previous studies that efficacy is higher when leucovorin is administered to younger vs older children, i.e. the sooner the better.
Approximately one-third of treated children demonstrated moderate to much improvement. The incidence of adverse effects was low.
This study suggests that FRAs may be important in ASD and that FRA-positive children with ASD may benefit from leucovorin calcium treatment.
Given these results, empirical treatment with leucovorin calcium may be a reasonable and non-invasive approach in FRA-positive children with ASD.
DTap vaccines are derived from broths containing casamino acids derived from cow’s milk. These aren’t just linked to folate receptor alpha autoantibodies, but to severe allergic reactions (anaphylaxis) to vaccination of children with milk allergies.
Cause and effect have been questioned (e.g. children with milk allergies were more likely to attend the clinic involved)11, but it is harder to dispute the link between milk proteins and allergies, and the temporal relationship between vaccination and allergic reactions.
The clinic also used Enzyme-linked Immunosorbent Assay (ELISA) to identify the milk proteins in the vaccine:
Allergic Reactions to Diphtheria, Tetanus, and Acellular Pertussis Vaccines Among Children with Milk Allergy (2011)
RATIONALE:
Vaccines containing diphtheria, tetanus, and acellular pertussis are processed in medium containing casamino acids derived from cow’s milk; several milk allergic children have reported allergic reactions following administration of these vaccines.
METHODS:
This was a chart review of patients seen in our practice who had reported allergic reactions after receiving tetanus vaccines (primary or booster doses) from September 2007 to March 2010. An inhibition-ELISA was performed to determine the presence of milk protein in the vaccines.
RESULTS:
We identified seven patients (5 male, 2 female; median age 11 years; range: 5-17), who reported convincing allergic reactions to tetanus vaccines.
Six patients had prior allergic reactions to cow’s milk, including severe reactions (5) and or reactions to trace exposures (4); one was diagnosed with milk allergy based on serologic testing.
All patients had elevated milk specific IgE levels documented within 2 years of their reactions to the vaccine: 59, 96, and 5 patients >100 kUA/L.
Each reported symptoms consistent with a diagnosis of anaphylaxis promptly after receiving the vaccine.
Treatments included antihistamines (5/7), epinephrine (3/7), inhaled beta-agonists (3/7), and corticosteroids (2/7). Assays were performed on 2 different lots of the tetanus, diphtheria, and acellular pertussis vaccine, confirming the presence of milk protein in one lot (30 ng/mL).
CONCLUSIONS:
Vaccines containing tetanus, diphtheria, and acellular pertussis derived from broths containing casamino acids may present a risk to persons with severe milk allergy.
Another Bradford Hill test, research from 2009 by Ramaekers et al., found that a milk-free diet helps to reduce levels of folate receptor autoimmunity.
Vaccine poisoned? This may help
I previously viewed “lactose-free” diets as something of a marketing fad, but it may indeed help many individuals, albeit unrelated to the absence of lactose!
A milk-free diet downregulates folate receptor autoimmunity in cerebral folate deficiency syndrome (2009)
Abstract
In cerebral folate deficiency syndrome, the presence of autoantibodies against the folate receptor (FR) explains decreased folate transport to the central nervous system and the clinical response to folinic acid.
Autoantibody crossreactivity with milk FR from different species prompted us to test the effect of a milk-free diet.
Intervention with a milk-free diet in 12 children (nine males, three females; mean age 6y [SD 4y 11mo], range l–19y), decreased autoantibody titer significantly from 2.08pmol of FR blocked per ml of serum (SD 2.1; range 0.24–8.35) to 0.35pmol (SD 0.49; range 0–1.32; p=0.012) over 3 to 13 months, whereas FR autoantibody titer increased significantly to 6.53 (SD 6.08; range 0.54–14.07; p=0.013) in nine children who were reexposed to milk for 6 to 14 weeks.
In 12 children on a normal diet (eight males, four females; mean age 5y 5mo [SD 4y 1mo], range 1y 6mo–16y 4mo), the antibody titer increased significantly from 0.84pmol of FR blocked per ml (SD 0.39; range 0.24–1.44) to 3.04pmol (SD 1.42; range 0.84–6.01; p=0.001) over 10 to 24 months.
Decreasing the autoantibody titer with a milk-free diet in conjunction with folinic acid therapy may be advocated for these patients.
From 2019, a further study linked vaccines with proteins derived from cow’s milk with IgE-mediated cow’s milk allergy (CMA):12
Disguised Dairy: Anaphylaxis to “Hidden” Allergens in Routine Vaccinations in Child with Severe Cow’s Milk Allergy
Rationale
IgE-mediated cow’s milk allergy (CMA) affects 2-3% of children under the age of 3. Allergic reactions to vaccines have been documented in egg allergic patients, however sparsely reported in the CMA population.
Methods
A 5-year-old male with severe IgE-mediated CMA was evaluated for anaphylaxis following two routine vaccinations. The patient received Adacel-Polio (TDaP-IPV) and Priorix-Tetra (MMR-V) as per immunization schedule. Within minutes of being immunized, the patient developed itchy eyes, sneezing, and facial swelling. The patient was treated and recovered.
Allergen investigation in vaccines identified casamino acids and lactose in the Adacel-Polio and Priorix-Tetra, respectively. Skin prick testing (SPT) to common allergens followed by SPT to full strength and intradermal testing (IDT) to 1/100 concentrations of Adacel-Polio and Priorix-Tetra vaccination were carried out.
Results
Milk protein was positive (15 mm). Very high levels of sIgE to total cow’s milk (>100 kU/L) and casein (79.80 kU/L) were found. Positive SPTs were identified to Adacel-Polio (7 mm) and Priorix-Tetra (5 mm). IDT were positive to Adacel-Polio (10 mm flare) and Priorix-Tetra (15 mm flare). Immunological assays (ELISA) for presence of cow’s milk protein in both vaccinations are pending.
Conclusions
TDaP-IPV and MMR-V vaccinations are generally well tolerated in children with food allergies. However, both vaccines have derivatives of cow’s milk protein that may pose as an allergenic source in certain children with severe CMA. It is important to educate physicians of potential reactions as neither vaccine’s product monograph identifies any risk of allergic reaction in this population.
Being more specific, the hypothesis is that some DTaP vaccines contain traces of bovine folate binding protein (bFBP). You do not need to be exposed to high titres of an antigen to prime the immune system towards an autoimmune response.
With DTaP vaccines, first exposure can be in the womb, as autoantibodies freely cross the placenta.13 The developing child is then exposed to another 5-6 doses, as part of the vaccination schedule.
Trace amounts of lactose hydrate in a routine Japanese encephalitis (JE) vaccine were sufficient to induce anaphylaxis in a 3-year-old boy:14
Vaccine-induced anaphylaxis in a child with cow’s milk allergy: Lactose hydrate was the culprit (2022)
Lactose hydrate was the cause of vaccine-induced anaphylaxis in a child with severe milk allergy. Although the amount of milk protein in lactose-containing vaccines is extremely small, physicians administering such a vaccine must be prepared for the potential risk of severe milk allergy.
Japanese encephalitis (JE) virus is the cause of the potentially fatal viral encephalitis that is endemic in the Southeast Asia and Western Pacific regions. Although JE vaccines are generally safe, sporadic cases of anaphylaxis as a vaccine adverse event (ie, 0.42 cases per million vaccinations in 2013-2020) have been reported in Japan.1 The cause of anaphylaxis, however, has not been well described.
Here, we report a case of anaphylaxis following JE vaccination of a child with cow’s milk allergy, and by using the basophil activation test (BAT), we confirmed the lactose hydrate in the vaccine as the culprit allergen.
The patient was a 3-year-old boy with milk allergy, egg allergy, and allergic rhinitis. He avoided milk from the age of 7 months, at which time he had manifested symptoms of urticaria after eating a food containing skimmed milk powder.
At the age of 3 years, he was able to consume a bread containing a small amount of milk (about 0.1 mL of milk per slice) without any symptoms. However, 1 month later, he started to feel itching of the tongue after eating the same bread.
At the age of 3 years and 6 months, he received the first dose of a JE vaccine (ENCEVAC [Chemo-Sero-Therapeutic Research Institute, Kumamoto, Japan]) at a local clinic.
He developed a cough and generalized urticaria 40 minutes after the vaccination. He was transferred to an emergency hospital, and anaphylaxis was diagnosed. Intramuscular epinephrine and an intravenous corticosteroid alleviated the symptoms. Later, he was referred to our department to determine the cause of the anaphylaxis.
Cow’s milk contains antigenic folate receptor alpha (FOLR1) protein, and it has been studied in detail, as folate-binding proteins help to improve the bioavailability of folate in milk.
The authors found that high-temperature treatment to pasteurise (373 K) and ultra-heat treatment (UHT, 408 K) of milk was sufficient to cause folate to disintegrate, leading to a lower folate concentration in UHT milk and dairy products.
Key takeaways from “Structural and dynamic investigation of bovine folate receptor alpha (FOLR1), and role of ultra-high temperature processing on conformational and thermodynamic characteristics of FOLR1–folate complex” (2014), by Sahoo et al:15
FBPs evolved this way in milk due to their ability to transport essential folate to the developing foetus:
… The folate binding proteins (FBPs) are present in the plasmalemmal vesicles of many epithelial cells binds to folic acid. Three major classes of proteins FBPs have been reported in various organisms in the plasma membrane and cytoplasm of cells [1]. The folate-binding proteins have been identified in the milk of different mammals that nourishes the infants [2].
Folate is a natural occurring B-vitamin with similar biological activity like folic acid. Natural occurrence of folate is very rare, but its reduced state is found in different body tissues. This plays an important role in cell replication because of its requirement for the synthesis of purines and pyrimidines [3,4], and DNA methylation [5].
The folate absorption is accomplished by two different classes of proteins such as folate carrier membrane proteins and FBP [6]. Three different types of homologues FBP receptors are presented in different organisms such as α, β and γ [7,8].
The high affinity FBP shows a close interaction with folates and consists of water-soluble and membrane-associated forms. The soluble forms FBPs are present in the serum and milk, and the membrane associated forms are observed on the surface of various cells and tissues [1,9,10].
Bovine is the most common and largest domestic animal with a wide livestock for milk and dairy products. The milk production accelerates the national economy and so occupies a high research interest in government and corporate sectors. The bovine milk contains high affinity FBPs and is a chief source of folate.
The folate binding protein 1 alternatively known as FOLR1 or milk FBP is a member of alpha folate receptor family, and constituted of 241 amino acids and functions as binding to folate and reduced folic acid derivatives such as 5-methyltetrahydrofolate, tetrahydrofolate, 5-formyltetrahydrofolate, etc. [11–13].
The binding affinity of folic acid to FBP in raw and processed milk varies in terms of folate concentration [2]. Folate deficiency in foods leads to several disorders and need to be explored.
The FBPs are associated with ovarian cancer that causes fatality with less survival rate, and its deficiency is associated with many diseases like leukemia, tumors, gastric cancers, rheumatoid arthritis, neurodegenerative disorders, etc. [14–18].
The brain-specific folate deficiency in breast feeding period of a child causes several neurodegenerative disorders. The crystal structures of FOLR-α in human bound to folate and antifolate (PDB ID: 4LRH, 4KMX, 4KM6 and 4KM7) have very recently been solved [19,20].
Different structural arrangements depending on the pH, binding modes of folate and antifolate have recently been presented suggesting the folate-based drug designing for the treatment of FOLR related disorders.
Previous studies have reported the effect of temperature on folate binding stability in FOLR1. A significant decrease in folate concentration in pasteurized milk processed by ultra-high temperature (UHT) processing has also been shown [2].
Picking up on the association with cancer, from their references, we learn that overexpression of FBP is a marker for ovarian and other cancers.16
… folate receptor levels effectively differentiate ovarian carcinoma from other cancers affecting the serosal cavities and that folate receptor genes are coexpressed in this tumor. The high expression of folate receptors in ovarian carcinoma supports their validity as molecular therapeutic targets in this disease.
… FR members are differentially expressed in normal and tumor tissues. FR-α, the most extensively studied family member, is expressed in urogenital organs, the female genital tract, salivary and bronchial glands, the choroid plexus, retinal pigment cells, and the placenta.
High FR-α levels have been detected in different carcinomas, including nonmucinous ovarian carcinoma (OC), endometrial carcinoma, and cervix carcinoma, as well as in nongenital tumors [1], [2].
The high expression of FR-α in cancer has led to extensive research regarding its potential role as a target for molecular therapy, as modulator of the immune system, and as a diagnostic marker in imaging (reviewed in Salazar & Ratnam [1]).
FR-β is expressed by hematopoietic cells and the placenta, as well as by leukemia and lymphoma cells.
FR-γ has been detected in normal and malignant hematopoietic cells, as well as carcinomas of the ovary, endometrium, and cervix (reviewed in References [1], [2]).
The presence of cancer cells within the serosal (peritoneal, pleural, or pericardial) cavities, with the accumulation of serous effusions, is most frequently encountered as part of metastatic dissemination from OC, breast carcinoma, or lung carcinoma.
It additionally occurs in most patients diagnosed with primary cancers of the serosal cavities, malignant mesothelioma (MM), and primary peritoneal carcinoma (PPC) [3]. The presence of cancer cells at this anatomic site is associated with poor prognosis [3].
“Expression of the folate receptor genes FOLR1 and FOLR3 differentiates ovarian carcinoma from breast carcinoma and malignant mesothelioma in serous effusions” (2009)
It would be interesting to study the effects of FRα autoantibodies on cancer, to find some benefit to DTaP vaccination, and there is ongoing research into this.
However, you probably wouldn’t use DTaP vaccines as they haven’t been optimised for this:
Review
Folate receptor alpha for cancer therapy: an antibody and antibody-drug conjugate target coming of age (2025)
… Folate receptor alpha (FRα) has long been the focus of therapeutics development in oncology across several solid tumors, notably ovarian, lung, and subsets of breast cancers. Its multiple roles in cellular metabolism and carcinogenesis and tumor-specific overexpression relative to normal tissues render FRα an attractive target for biological therapies.
Here we review the biological significance, expression distribution, and characteristics of FRα as a highly promising and now established therapy target.
We discuss the ongoing development of FRα-targeting antibodies and antibody-drug conjugates (ADCs), the first of which has been approved for the treatment of ovarian cancer, providing the impetus for heightened research and therapy development.
Novel insights into the tumor microenvironment, advances in antibody engineering to enhance immune-mediated effects, the emergence of ADCs, and several studies of anti-FRα agents combined with chemotherapy, targeted and immune therapy are offering new perspectives and treatment possibilities.
… In normal physiology, FRα is predominantly expressed in the apical or luminal surfaces of polarized epithelia that do not have direct access to circulating folate. Tissues known to express FRα include the choroid plexus, lung, thyroid, retina, and placenta.Citation16–18 In addition, expression within the kidney is restricted to the proximal tubule, where FRα is thought to help reabsorb folate back into the circulation prior to urinary excretion.Citation19
Figure 2. Proposed FRα-mediated endocytosis and signaling pathways in cells. GPI-anchored FRα is invaginated into caveolae vesicles and forms early-to-late endosomes, which undergo increasing acidification and subsequent fusion with lysosomes to release non-anchoring FRα and folate/drugs. Alternatively, the GPI-anchored FRα is recycled from late endosomes to cell membrane. Proposed signaling pathways associated with FRα are presented in ①-④. ①The GPI-specific phospholipase D cuts off the GPI anchor of FRα in lysosomes, resulting in the free FRα translocating into nucleus and acting as a transcription factor. ②FRα physically interacts with the Progesterone Receptor (PR) and the cellular proto-oncogene tyrosine-protein kinase (cSrc) in a trimeric complex. cSrc auto-phosphorylates to activate itself and promotes the phospho-activation of ERK. Activated ERK induces the transcription of TP53 to regulate cell cycle progression. ③Folate binding to FRα can induce the activation of the JAK/STAT3 signaling pathway via the gp130 co-receptor, leading to cell proliferation. ④FRα may upregulate the expression of cell-cell adhesion molecule E-cadherin to promote cell migration. Created with BioRender.com. Abbreviations: FRα, folate receptor alpha; GPI, glycosylphosphatidylinositol; RFC, reduced folate carrier; PCFT, proton-coupled folate transporter; PR, progesterone receptor; JAK, Janus kinase; cSrc, cellular proto-oncogene tyrosine-protein kinase; STAT3, signal transducer and activator of transcription 3.
In the first instance, FRα, as an important folate transporter, appears to promote tumorigenesis by supplying folate to fuel cancer cell metabolism. Bistulfi et al. showed that mild folate depletion induces genetic and epigenetic instability in prostate cancer cells compared with those supplemented with higher levels of folate.Citation29
As ever, it’s not that simple, as dietary intake of folate is associated with a lower cancer risk, and DTaP vaccines also activate the same oncogenic STAT3, MAPK and ERK signalling pathways.
The pertussis toxin (PTx) component, in particular, has been shown to activate STAT3.1718
Unintended activation of oncogenic signalling pathways is one of the reasons why cancer vaccines are an oxymoron. If you need to use adjuvants, then you have already failed.19
However, as folate homeostasis is predominantly controlled by RFC, the importance of FRα in mediating this phenotype remains controversial. A meta-analysis suggested dietary folate intake may reduce the risk of developing breast cancer risk, complicating this relationship further.Citation30
Alternatively, it has been proposed that the contributions of FRα in cancer development are primarily driven by its transcription factor function. Nuclear translocation of FRα is associated with increased proliferation and reprogramming toward a ‘cancer stem cell’ through activation of numerous transcription factors, including OCT4/SOX2 (regulating stemness), KLF4 (regulating cell reprogramming), HES1 (regulating metastasis and multidrug resistance), and FGFR4 (regulating cellular proliferation).Citation22,Citation23
Finally, emerging evidence suggests that FRα directly interacts with signaling pathways that promote tumorigenesis (Figure 2). For example, folate-FRα complexes can activate oncogenic STAT3 in a JAK-dependent manner with the aid of the co-receptor gp130.Citation31
FRα is also thought to interact with the serine/threonine kinases ERK1/2, core mediators of the mitogen-activated protein signaling pathway. This pathway was proposed by Lee and colleagues, who described a direct interaction between FRα and cSrc (cellular proto-oncogene tyrosine-protein kinase) with the aid of the progesterone receptor in colon cancer cell lines.
This Trimeric complex promotes the activation of ERK signaling pathway and thus may regulate TP53 gene transcription.Citation32 In addition, in ovarian cancer, knockdown of FRα abrogates cellular proliferation and migration, potentially through downregulation of the cell–cell adhesion molecule E-cadherin.Citation33 These data suggest that the oncogenic functions of FRα extend well beyond its canonical role in metabolism.
They’ve already clinically tested an FRα vaccine in combination with a PD-L1 inhibitor antibody, but unfortunately, it failed. Only one patient demonstrated a short-term partial response:
… In addition to anti-FRα ADCs, FRα vaccines have also been considered to help overcome PD-1/PD-L1 therapy resistance in advanced ovarian cancer. One such Phase 2 clinical trial in patients with recurrent ovarian cancer (NCT02764333) combined TPIV200, a peptide vaccine composed of five immunogenic peptide epitopes of FRα, with durvalumab, a PD-L1 inhibitor antibody.Citation110
Although treatment was well tolerated and increased early T cell responses were observed, only one patient demonstrated a partial response, and all patients ultimately progressed. Nevertheless, the overall survival duration was notably longer than expected for such a heavily pretreated patient cohort. These data suggest that vaccine approaches are worthy of further investigation, although their role relative to better-established strategies remains uncertain.
Key takeaways from “High milk consumers have an increased risk of folate receptor blocking autoantibody production but this does not affect folate status in Spanish men and women” (2009), by Berrocal-Zaragoza et al.20
I’m including this paper in the review as they confirmed the correlation, despite only measuring serum folate levels, and there being no discussion about possible CSF folate deficiency. They only analysed blood samples.
tHcy: Total homocystein.
We investigated their prevalence and association with folate status and milk intake in adults unexposed to folic acid fortification. A cross-sectional study of a randomly selected representative sample of a Spanish population (aged 18–75 y) stratified by age and gender was performed.
Lifestyle data were collected and milk intake estimated from a 3-d dietary record. FR-autoantibody prevalence was 7.2% [0.30 ± 0.27 nmol (mean ± SD) FR blocked/L], equally affecting men and women of all ages.
Plasma and red cell folate and tHcy did not differ between carriers and noncarriers of FR-autoantibodies.
Milk intake was higher in carriers (225 ± 199 g/d) than in noncarriers (199 ± 147 g/d) (P < 0.01).
The risk of having FR-autoantibodies increased progressively with increasing quintile of milk intake and was significant in the highest quintile (≥307 g/d) compared with the lowest (≤67 g/d) [odds ratio (OR), 2.41 [95% CI: 1.02, 5.69]; P < 0.05; linear trend, P = 0.02].
We concluded that FR-autoantibodies occur in men and women of all ages and do not affect indicators of folate status such as plasma and red cell folate and tHcy.
Higher milk intake is associated with increased risk of having FR-autoantibodies.
Our final paper in this Substack review is from 2014, by Cabrera et al.21
Whether these autoAbs are due to dietary milk intake or vaccination, I consider it reckless to administer a DTaP shot during pregnancy. This is typically administered between 16 and 32 weeks.
Parentally administered antigens are much more immunogenic than swallowed peptides, which gastric acid and enzymes can denature. This is why DTaP and other vaccines aren’t given orally, as a capsule or a liquid.
Getting vaccinated in pregnancy is important
The protection you receive from the whooping cough vaccine passes to your unborn baby and helps protect them in the first few weeks of their life, until they have their first routine immunisation when they are eight weeks old.
The vaccine also protects you from getting whooping cough and lowers the risk of you passing it on to your baby.
There is no vaccine that only protects against whooping cough. The vaccine you will be given is a combined vaccine that protects against different diseases, including whooping cough. The vaccine is not live, and it cannot cause whooping cough. You will be offered one dose of the vaccine, which is given as an injection in the upper arm.
From: “Whooping cough (pertussis) vaccination in pregnancy: How to protect your baby against whooping cough”
Autoantibodies to folate receptor during pregnancy and neural tube defect risk (2014)
Periconceptional folic acid can reduce the occurrence of neural tube defects (NTDs) by up to 70%, and autoantibodies for folate receptors (FRs) have been observed in serum from women with a pregnancy complicated by an NTD.
This population-based cohort study has examined serum from pregnant mothers for autoantibodies to FRs, antibodies to bovine folate binding protein (FBP), and inhibition of folic acid binding to FR and FBP in association with NTD risk.
This overlaps with the early vaccination window. Specimens collected later would have been of particular interest, in that correlations with ASD and ADHD could have been analysed.
The mid-gestational maternal serum specimens used for this study were collected during the 15th–18th week of pregnancy. Samples were obtained from the California Birth Defects Monitoring Program; 29 mothers had a pregnancy complicated by spina bifida and 76 mothers had unaffected children.
The presence of IgG and IgM antibodies to human FR, bovine FBP, and inhibition of folic acid binding to FR and FBP was determined.
Higher activity of IgM to FBP in cases verses controls was observed(P=.04). Higher activity of IgM and IgG autoantibodies to FR was observed (P<0.001 and P=.04, respectively).
Risk estimates at two standard deviations above average control antibody concentrations were OR=2.07 (CI=1.02, 4.06) for anti-FBPIgM, OR=2.15 (CI=1.02, 4.69) for anti-FRIgG and OR=3.19 (CI=1.47, 6.92) for anti-FR IgM.
These data support the hypothesis that high titers of antibodies and blocking of folic acid binding to FRs by maternal serum should be regarded as risk factors for NTDs.
… Rothenberg et al. (2004) reported autoantibodies to the FR in 75% of 12 mothers who had given birth to NTD-affected infants, but in only 8.3% of mothers of 24 non-malformed infants.
Unfortunately, this provocative but small study examined only three women during pregnancy, all of whom had a pregnancy complicated by an NTD. Maternal autoantibodies to FR that produce immune responses against, or inhibit folate uptake by, the developing embryo may explain the beneficial effect of periconceptional folic acid supplementation on NTD risk.
That is, supplemental folic acid may reduce the level of serum autoantibodies or compensate for blocking of the receptors caused by FR autoantibodies.
Figure 1. Antibody detection and folic acid binding inhibition. Images show the functional testing results of the assay. The vertical axes of the graphs represent detected signal intensities (8-bit). (A) A serial dilution (1:10 to 1:640) of a positive serum sample is shown for IgG antibodies against bovine folate binding protein (FBP). Fluorescent intensities were extracted and plotted against a regression line with standard errors to generate the graph. (B) Results are displayed for folic acid binding to FBP. A dilution series of folic acid was used to quantify interactions. Fluorescent intensities were extracted, log-transformed and fitted against a sigmoid regression curve for the graph (GraphPad Software, San Diego, CA).
… During the fourth week of gestation, the neural tube closes and the human embryo is interstitially implanted into the uterine wall, and migration of syncitiotrophoblasts and cytotrophoblasts has formed chorionic villi that cover the entire surface of the blastocyst (Cross et al., 1994). The cytotrophoblasts of these villi have been observed to function as a barrier to the transport of IgG during this stage of development (Bright and Ockleford, 1995).
AutoAbs shouldn’t be able to reach the embryo, yet they can still affect folate transportation:
.These observations suggest that, during neural tube closure, IgM and IgG antibodies are prohibited from reaching the embryo. However, autoantibodies may indirectly influence neural tube closure and NTD risk.
These indirect influences would include IgG or IgM immune responses at the maternal-embryonic trophoblast interface and inhibition of nutrient transport to the blastocyst.
In support of inhibition of nutrient transport, we observed also that the serum from mothers who delivered an NTD-affected child significantly blocked higher concentrations of folic acid from binding to FBP and FR versus serum from mothers of an unaffected child.
However, several samples with high titers of antibodies allowed FR and FBP still to bind folic acid. This may indicate that the antibodies can bind FR and FBP at different locations, but they must interact with specific epitopes in order to inhibit folic acid binding.
In support of direct and indirect influences, binding to or blocking of folic acid to FR increased NTD risk estimates to the greatest extent. Specifically, IgM autoantibodies, folic acid blocking and IgG autoantibodies against FR had the highest estimates of NTD risk at two standard deviations (Table 2).
This hints at epigenetics and other factors involved in triggering autoimmunity during pregnancy:
… The forbidden clone hypothesis indicates that autoimmunity is mitigated by clonal selection (Burnet, 1972) but, if proteins expressed by developmental tissues undergo modification during periods of inflammation or metabolic stress, an immune response may be activated against the modified forms (McCully, 1993,1994; Undas et al., 2004).
The link between dietary folate and coronary artery disease (CAD) is discussed, and how the authors suspect that autoAbs against homocysteinylated serum proteins may cross-react against native folate receptors:
Folic acid supplementation has been reported to lower homocysteine, homocysteine thiolactone and autoantibodies against homocysteinylated serum proteins in a majority of patients with coronary artery disease (Undas et al., 2006).
Based on these observations, we suspect that the etiology of FR autoantibodies may be due in part to post-translation modification of proteins by homocysteine thiolactone in vivo and that autoantibodies produced against homocysteinylated FRs may cross-react with native FR and increase the risk for folate responsive birth defects, such as NTDs.
In conclusion, they suspect that the low incidence of NTDs observed was due to folic acid fortification, but that not all NTDs are folate-responsive. However, they do not discuss DTap vaccination during pregnancy and its association with autoantibodies to bovine milk proteins:
This study was conducted during a time period when the food supply was fortified with folic acid, so this may explain the low ~1/4700 incidence of NTDs and also makes it unlikely that all of the observed NTDs are folate-responsive. However, if folic acid supplementation reduces the homocysteinylation of other proteins critical for embryonic development, antibodies against these proteins may also modify birth defect risk.
Despite raised awareness to get diagnosed, there is no significant increase in the number of cases or fatality rates linked to bacterial meningitis in the UK:
Even if there were, vaccination is not the answer. In fact, it’s one of the best ways to induce antigenic sin, to break the dominance of your cross-reactive T cell clonotypes, and to paradoxically risk an increased future likelihood of infection.
At least 10% of us are asymptomatic carriers of the bacterium Neisseria meningitidis (also known as meningococcus)22, which means that, unless you live permanently in perfect isolation, most of us are regularly exposed to a sufficient non-infectious dose of the bacterium to maintain a degree of long-term immunity to the current strains in circulation. We see the same with many other aerosolised pathogens.
Those most at risk of death through septicaemia are strongly immunosuppressed. The “vaccine paradox” is that if your immune system is strong enough to generate the required robust immune response to the vaccine, then you probably don’t need it. Whereas those most at risk of the disease get the least benefit.
COVID vaccines were always so far behind the current variant that the strain was frequently functionally extinct by the time they became commercially available. With Neisseria meningitidis, vaccine escapeis worse still.
It’s so bad that only a bunch of clowns and fraudsters could be promoting vaccination as a public health measure.
Talking of which, it follows that Clueless Wes stood before parliament this week, and did exactly that.
What a dipstick.
Wes Streeting tells House of Commons meningitis outbreak is unprecedented
Wes Streeting tells the House of Commons the deadly meningitis outbreak in Kent is ‘unprecedented.’
Tuesday 17 March 2026 13:56, UK
The health secretary warns the symptoms can be confused for a hangover and stressed the importance of vaccinations and antibiotics.
From 2023, Mikucki & Kahler threw a few truth bombs:23
Microevolution and Its Impact on Hypervirulence, Antimicrobial Resistance, and Vaccine Escape in Neisseria meningitidis
Abstract
Neisseria meningitidis is commensal of the human pharynx and occasionally invades the host, causing the life-threatening illness invasive meningococcal disease.
The meningococcus is a highly diverse and adaptable organism thanks to natural competence, a propensity for recombination, and a highly repetitive genome.
These mechanisms together result in a high level of antigenic variation to invade diverse human hosts and evade their innate and adaptive immune responses. This review explores the ways in which this diversity contributes to the evolutionary history and population structure of the meningococcus, with a particular focus on microevolution.
It examines studies on meningococcal microevolution in the context of within-host evolution and persistent carriage; microevolution in the context of meningococcal outbreaks and epidemics; and the potential of microevolution to contribute to antimicrobial resistance and vaccine escape.
A persistent theme is the idea that the process of microevolution contributes to the development of new hyperinvasive meningococcal variants.
As such, microevolution in this species has significant potential to drive future public health threats in the form of hypervirulent, antibiotic-resistant, vaccine-escape variants. The implications of this on current vaccination strategies are explored.
… Nme normally colonises the nasopharyngeal epithelium in humans and is transmitted by aerosolised droplets or contact with infected fluids such as saliva.
IMD occurs when the meningococcus crosses the nasopharyngeal epithelium and enters the bloodstream, resulting in the rapid onset of septicaemia and/or meningitis [7]. Since infection of neither the blood nor meninges improves the transmission of the meningococcus, IMD is considered to be an evolutionary dead end for this organism [8].
The events which initiate the development of IMD from carriage are not fully understood but include host factors such as viral infection and environmental factors such as climate [9].
The meningococcal population itself is not uniform in its ability to cause disease, with some isolates being associated entirely with carriage and others being associated more commonly with disease.
The ability of a given meningococcal lineage to cause disease can be given by the odds ratio of the association of that lineage with disease over carriage (defined as the disease/carriage ratio, D/C ratio) [10]. Large studies assessing meningococcal carriage and disease across multiple countries have found a broad diversity in D/C ratio among meningococcal genetic lineages, with some being exclusively associated with carriage and others frequently causing disease.
… Concerns about vaccine escape have also been raised in the context of meningococcal vaccinations. Capsule switching is of primary concern for the conjugate polysaccharide vaccines, whereas antigen variation and/or loss of expression of the major components may lead to escape from MenB vaccination.
Of particular concern is the potential for the emergence of a hypervirulent MenB lineage (for example, cc41/44, cc32, or a capsule-switched cc11) which could potentially undergo antigenic shift to escape coverage by the MenB vaccines [164].
Despite these concerns, relatively few studies have inspected the genomic changes which occur in the meningococcal population under high levels of vaccine selective pressure.
One consideration for the potential of meningococcal vaccine escape is that vaccines must place a selective pressure on carried meningococci since isolates causing IMD do not take part in transmission.
Prevention of meningococcal carriage is established for conjugate polysaccharide vaccines but not for the MenB-targeting protein vaccines [212]. Since meningococci are able to downregulate capsule expression or switch capsules entirely [92], vaccine escape might be expected to occur.
Similarly, high levels of variation are observed in the major components of both the Bexsero® (fHbp, NadA, NHBA, and PorA [213]) and Trumenba® (fHbp [214]) vaccines within the meningococcal population [67,215,216,217,218,219,220].
If you are seriously concerned about infection, then eat an egg yolk and oily fish each day, along with a source of minerals and vitamins—especially vitamins A and D3:
Vitamin A deficiency and T-cell subpopulations in children with meningococcal disease (1996)
Abstract
Although group A meningococcal disease is a major cause of child morbidity and mortality in sub-Saharan Africa, little is known about vitamin A status and T-cell subpopulations in affected children.
A prospective study of vitamin A levels and T-cell subpopulations was conducted in 41 children hospitalized for meningococcal meningitis in Butare, Rwanda, during an epidemic from September through November, 1992.
The mean age of cases was 3.6 +/- 2.7 years (range 0.5-16 years). The case-fatality rate was 20 per cent; 73 per cent of the children had serum vitamin A levels consistent with subclinical deficiency (< 0.7 mumol/l), and 27 per cent had levels consistent with severe deficiency (< 0.35 mumol/l).
Mean CD4 per cent was higher and CD8 per cent was lower among children with meningitis compared with known reference populations. These results suggest that meningococcal disease is characterized by T-cell subpopulation alterations and vitamin A deficiency.
Vitamin D deficiency decreases survival of bacterial meningoencephalitis in mice (2008)
Abstract
Background
Meningoencephalitis caused by Escherichia coli is associated with high rates of mortality and risk of neurological sequelae in newborns and infants and in older or immunocompromised adults. A high prevalence of neurological disorders has been observed in geriatric populations at risk of hypovitaminosis D.
Methods
In vivo, we studied the effects of vitamin D3 on survival and the host’s immune response in experimental bacterial meningoencephalitis in mice after intracerebral E. coli infection. To produce different systemic vitamin D3 concentrations, mice received a low, standard, or high dietary vitamin D3 supplementation. Bacterial titers in blood, spleen, and brain homogenates were determined. Leukocyte infiltration was assessed by histological scores, and tissue cytokine or chemokine concentrations were measured.
Results
Mice fed a diet with low vitamin D3 concentration died earlier than control animals after intracerebral infection. Vitamin D deficiency did not inhibit leukocyte recruitment into the subarachnoid space and did not lead to an increased density of bacteria in blood, spleen, or brain homogenates.
The release of proinflammatory interleukin (IL)-6 was decreased and the release of anti-inflammatory IL-10 was increased in mice fed a diet with high vitamin D3 supplementation.
Conclusion
Our observations suggest a detrimental role of vitamin D deficiency in bacterial central nervous system infections. Vitamin D may exert immune regulatory functions.
The novel role of vitamin D in the fight against gram negative bacterial meningitis (2008)
Gram negative bacterial meningitis with consequent meningeal inflammation is a major cause of death and morbidity worldwide. Meningitis denotes infection of the blood brain barrier (BBB) including the choroid plexus (CP), the site of secretion of cerebrospinal fluid (CSF).
We propose that 1α 25-dihydroxyvitamin D3 (1α25-(OH)2D3), an important immunomodulator, may suppress CP inflammation thereby reducing morbidity. We aimed to assess the effects of 1α25-(OH)2D3 in a primary human choroid plexus epithelial (HCPEpi) cell line in the context of gram negative bacterial infection, simulated by using lipopolysacharide (LPS) endotoxin.
HCPEpi cells were incubated with 1 μgml−1 LPS in the presence and absence of 1 μM 1α25-(OH)2D3 for 4, 8 and 12 h. Expression of key elements of the vitamin D pathway (toll like receptor 4 (TLR4), vitamin D receptor (VDR), 25-hydroxyvitamin D3−1α hydroxylase (1αOH), 25-hydroxyvitamin D3-24 hydroxylase (24OH), interleukin (IL)-6, IL-8 and IL-1β) were confirmed using reverse transcription polymerase chain reaction (PCR).
Treatment with LPS and 1α25-(OH)2D3 demonstrated induction of IL-6, IL-8 and IL-1β mRNA using real-time PCR. Analysis of these cell culture supernatants using multiplex bead immunoassays illustrated up-regulation of IL-6, tumour necrosis factor α (TNFα) and interferon γ (IFNγ) protein.
We have identified that 1α25-(OH)2D3 induces early pro-inflammatory actions in HCPEpi cells immediately following LPS recognition. The late actions of 1α25-(OH)2D3 in meningitis remain to be explored.
The early inflammatory reaction may represent an important step in mounting an immune response against gram negative pathogens. Manipulation of local production of vitamin D may therefore have a role in the treatment of gram negative bacterial meningitis.
DTaP vaccination during pregnancy is strongly skewed towards risk without benefit, as the mother already shares relevant antibodies to the circulating strains of the day with the developing baby. This acts as an immunological bridge until the newborn has developed its own immune system. If this weren’t the case, then mammals would have become extinct aeons ago.
Not medical advice, but if you or your child suffers from a neurological or behavioural disorder, then several months on a milk-free diet, combined with supplementation with folinic acid MAY be of benefit. Consult a qualified dietician so that other deficiencies or side effects aren’t an unintended consequence. Folinic acid is also more likely to prevent NTDs than the synthetic version, but no regimen is 100% effective.
Similarly, if you have Parkinson’s or a mutation in genes like PINK1, PARKIN, FOLR1or MTHFR, then a diet that is skewed towards folinic acid instead of synthetic folic acid may be of benefit.
Therapeutic Leucovorin (calcium folinate) is a prescription-only medicine (POM) in the UK. It’s used to treat the side effects of chemotherapy and megaloblastic anaemia, whereas the less effective, and potentially harmful, synthetic form of vitamin B9 is being forced on the population.
If you plan to source it yourself or reside in a country where folinic acid is available without a prescription, then please note that Leucovorin is also not free of potential side effects or drug interactions. See here.
Look after your microbiome with prebiotics and probiotics such as kefir. Bifidobacteria are particularly useful, as they produce folate in the gut. This has been extensively researched.24
DoorlessCarp’s Scientific Literature Reviews is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
This site is strictly an information website reviewing research into potential therapeutic agents. It does not advertise anything or provide medical advice, diagnosis, or treatment. This site does not promote any of these as potential treatments or offer any claims for efficacy. Its content is aimed at researchers, registered medical practitioners, nurses, or pharmacists. This content is not a substitute for professional medical advice, diagnosis, or treatment.
Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Always consult a qualified health provider before introducing or stopping any medications, as any possible drug interactions or effects will need to be considered.
Any extracts quoted in the previous article are for non-commercial research and educational purposes only and may be subject to copyright from their respective owners.
Today’s Substack has been brought to you by the letters F U B A and R.
Scaglione F, Panzavolta G. Folate, folic acid and 5-methyltetrahydrofolate are not the same thing.Xenobiotica. 2014;44(5):480-488. doi:10.3109/00498254.2013.845705
Wells L, O’Hara N, Frye RE, Hullavard N, Smith E. Folate Receptor Alpha Autoantibodies in the Pediatric Acute-Onset Neuropsychiatric Syndrome (PANS) and Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS) Population.Journal of Personalized Medicine. 2024;14(2). doi:10.3390/jpm14020166
Luwen H, Ping C, Qing-Rong O, Lei X, Linlin L, Yu M. Association between serum folate levels and migraine or severe headaches: A nationwide cross-sectional study.Medicine (Baltimore). 2024;103(45):e40458. doi:10.1097/MD.0000000000040458
Sonawane K, Zhu Y, Chan W, Aguilar D, Deshmukh AA, Suarez-Almazor ME. Association of Serum Folate Levels With Cardiovascular Mortality Among Adults With Rheumatoid Arthritis.JAMA Netw Open. 2020;3(2):e200100. doi:10.1001/jamanetworkopen.2020.0100
Bobrowski-Khoury N, Sequeira JM, Quadros EV. Brain Uptake of Folate Forms in the Presence of Folate Receptor Alpha Antibodies in Young Rats: Folate and Antibody Distribution.Nutrients. 2023;15(5):1167. doi:10.3390/nu15051167
Slater JE, Rabin RL, Martin D. Comments on cow’s milk allergy and diphtheria, tetanus, and pertussis vaccines.Journal of Allergy and Clinical Immunology. 2011;128(2):434. doi:10.1016/j.jaci.2011.06.028
Scheffler SA, Vakaljan SL, Wu V, Ohayon JA. Disguised Dairy: Anaphylaxis to “Hidden” Allergens in Routine Vaccinations in Child with Severe Cow’s Milk Allergy.Journal of Allergy and Clinical Immunology. 2019;143(2):AB57. doi:10.1016/j.jaci.2018.12.175
Palmeira P, Quinello C, Silveira-Lessa AL, Zago CA, Carneiro-Sampaio M. IgG Placental Transfer in Healthy and Pathological Pregnancies. Clin Dev Immunol. 2012;2012:985646. doi:10.1155/2012/985646
Yoshino S, Hiraguchi Y, Tatekawa M, et al. Vaccine-induced anaphylaxis in a child with cow’s milk allergy: Lactose hydrate was the culprit.Journal of Allergy and Clinical Immunology: Global. 2022;1(2):87-89. doi:10.1016/j.jacig.2022.01.003
Sahoo B, Maharana J, Patra M, et al. Structural and dynamic investigation of bovine folate receptor alpha (FOLR1), and role of ultra-high temperature processing on conformational and thermodynamic characteristics of FOLR1–folate complex.Colloids and surfaces B: Biointerfaces. Published online June 23, 2014. doi:10.1016/j.colsurfb.2014.05.028
Karassek S, Starost L, Solbach J, et al. Pertussis Toxin Exploits Specific Host Cell Signaling Pathways for Promoting Invasion and Translocation of Escherichia coli K1 RS218 in Human Brain-derived Microvascular Endothelial Cells.J Biol Chem. 2015;290(41):24835-24843. doi:10.1074/jbc.M115.650101
Gillard J, Suffiotti M, Brazda P, et al. Antiviral responses induced by Tdap-IPV vaccination are associated with persistent humoral immunity to Bordetella pertussis.Nat Commun. 2024;15(1):2133. doi:10.1038/s41467-024-46560-w
Berrocal-Zaragoza MI, Murphy MM, Ceruelo S, Quadros EV, Sequeira JM, Fernandez-Ballart JD. High milk consumers have an increased risk of folate receptor blocking autoantibody production but this does not affect folate status in Spanish men and women.J Nutr. 2009;139(5):1037-1041. doi:10.3945/jn.108.102475
Mikucki A, Kahler CM. Microevolution and Its Impact on Hypervirulence, Antimicrobial Resistance, and Vaccine Escape in Neisseria meningitidis.Microorganisms. 2023;11(12):3005. doi:10.3390/microorganisms11123005
A life changing article and I hope it’s okay if I bring parts of it to the pediatric neurologist of my daughter. I cannot tell you how much of my little free time I have spent trying to unlock the mysteries of “leucovorin”. I looked everywhere for studies with every search word you can imagine, it took months to find even that meta data study (which is actually only based on 2 studies) and the adult onset Cerebral Folate Deficiency study. I was baffled at how this stuff was memory holed. Then I watched in real time as my favorite recent study, which was double blind and randomized (the gold standard for the credentialist doctors) was retracted! I still don’t know what data was “falsified” (that is how Cremieux on X described it- outrageous) so that I could see whether the retraction was justified or not.
On a personal note, my other daughter with high functioning autism (mostly crippling anxiety) has been taking folinic acid (the over the counter version is only .8mg so I have to give many) and she has explained to me how it has been life changing with so much of her anxiety drifting away. She is SO much better. Also, my mother and maternal grandmother both died of ovarian cancer. So we quite obviously have an FRAA problem.
I am eternally grateful for you doing this deep dive, it’s mentally crippling to have this information and see how many people could be benefiting from folinic acid and know that you will never be heard. I hope many people read you article and try it, its water soluble so the excess should be easily excreted. Thank you from the bottom of my heart, I’m not crazy.







: Causes & Prevention")
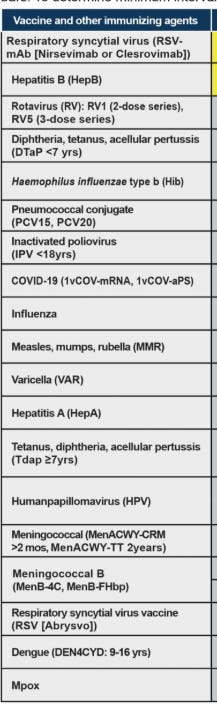
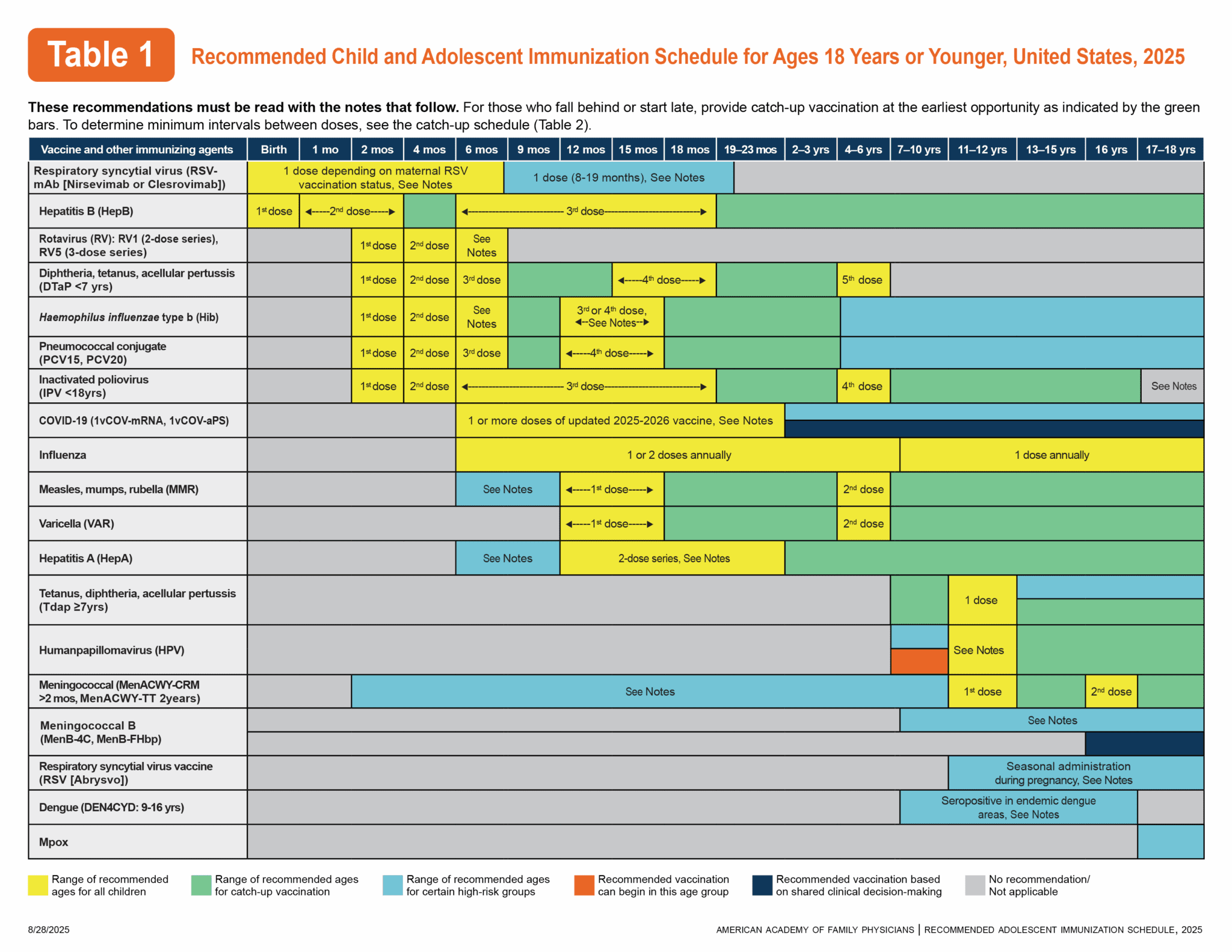






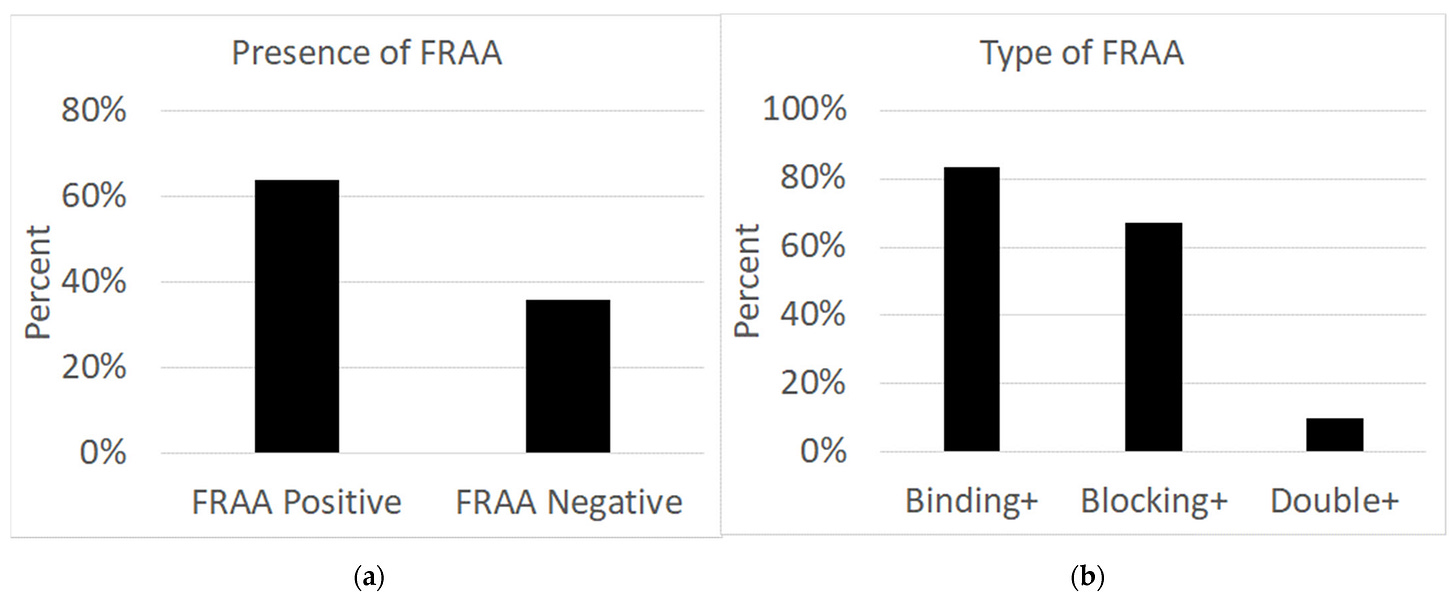
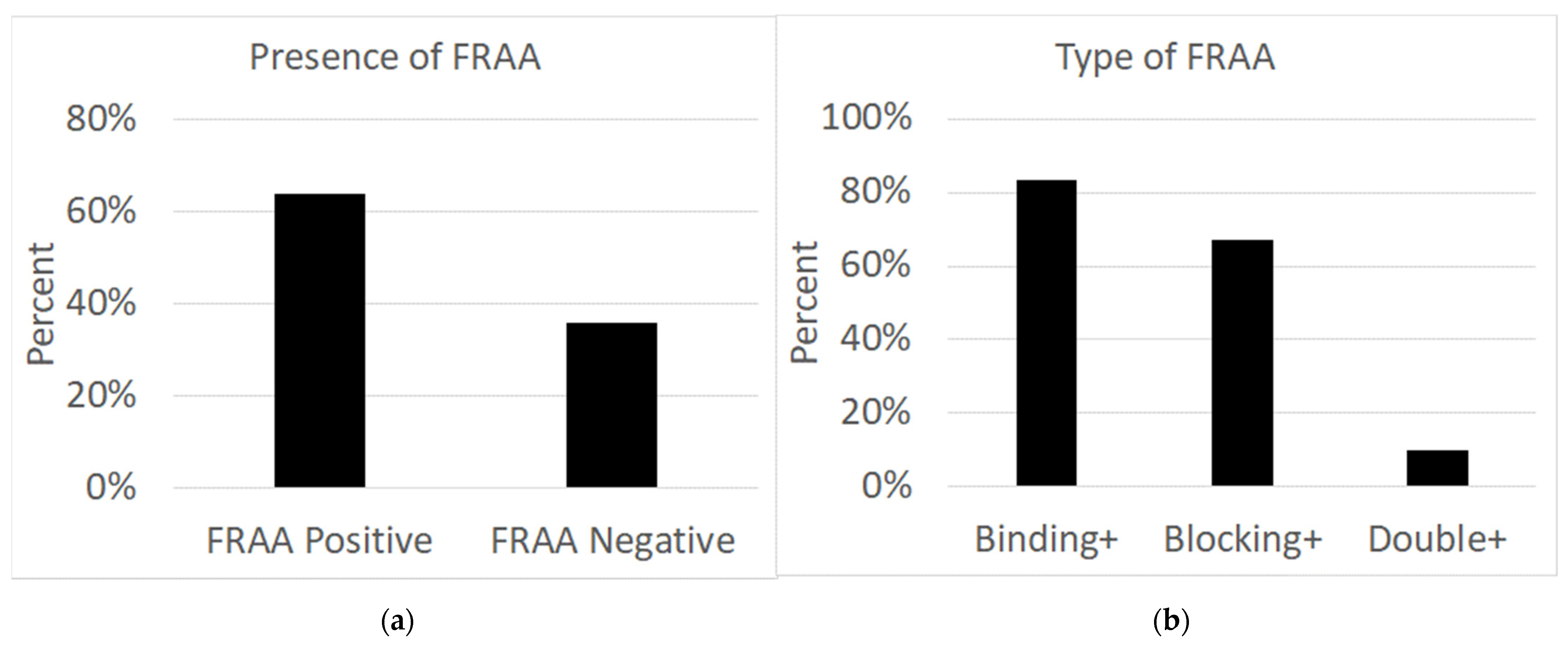
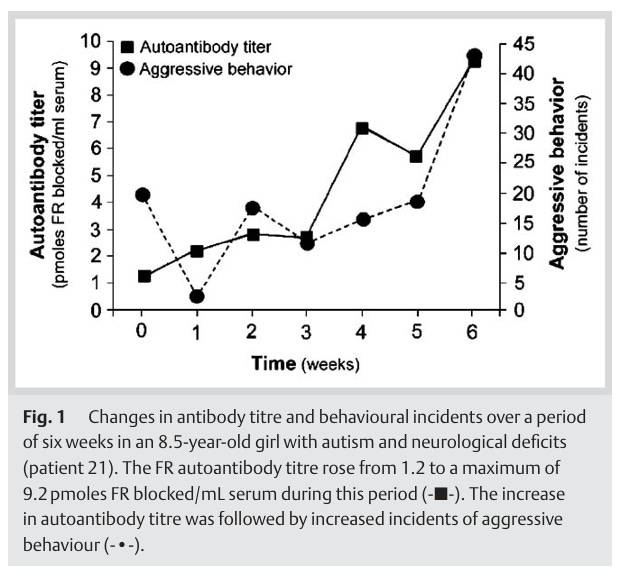
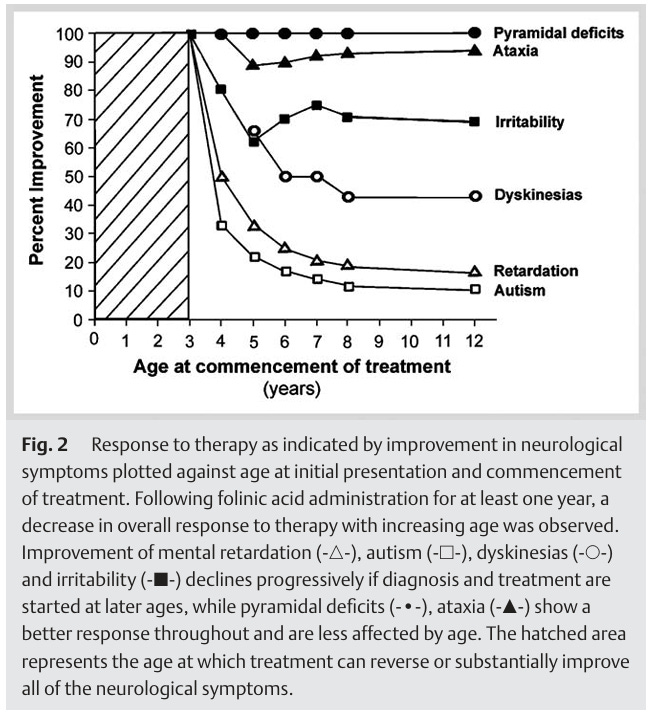




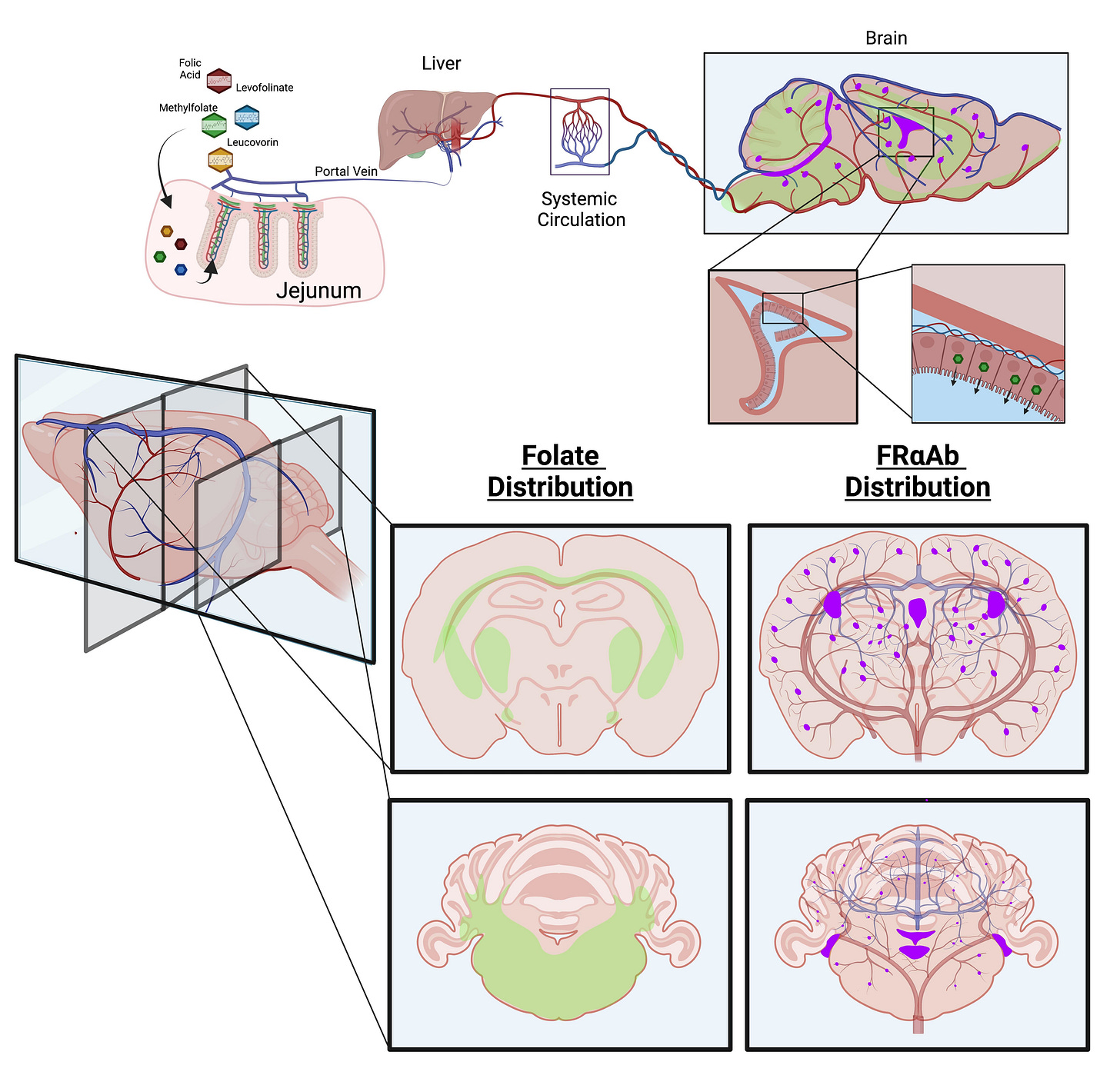
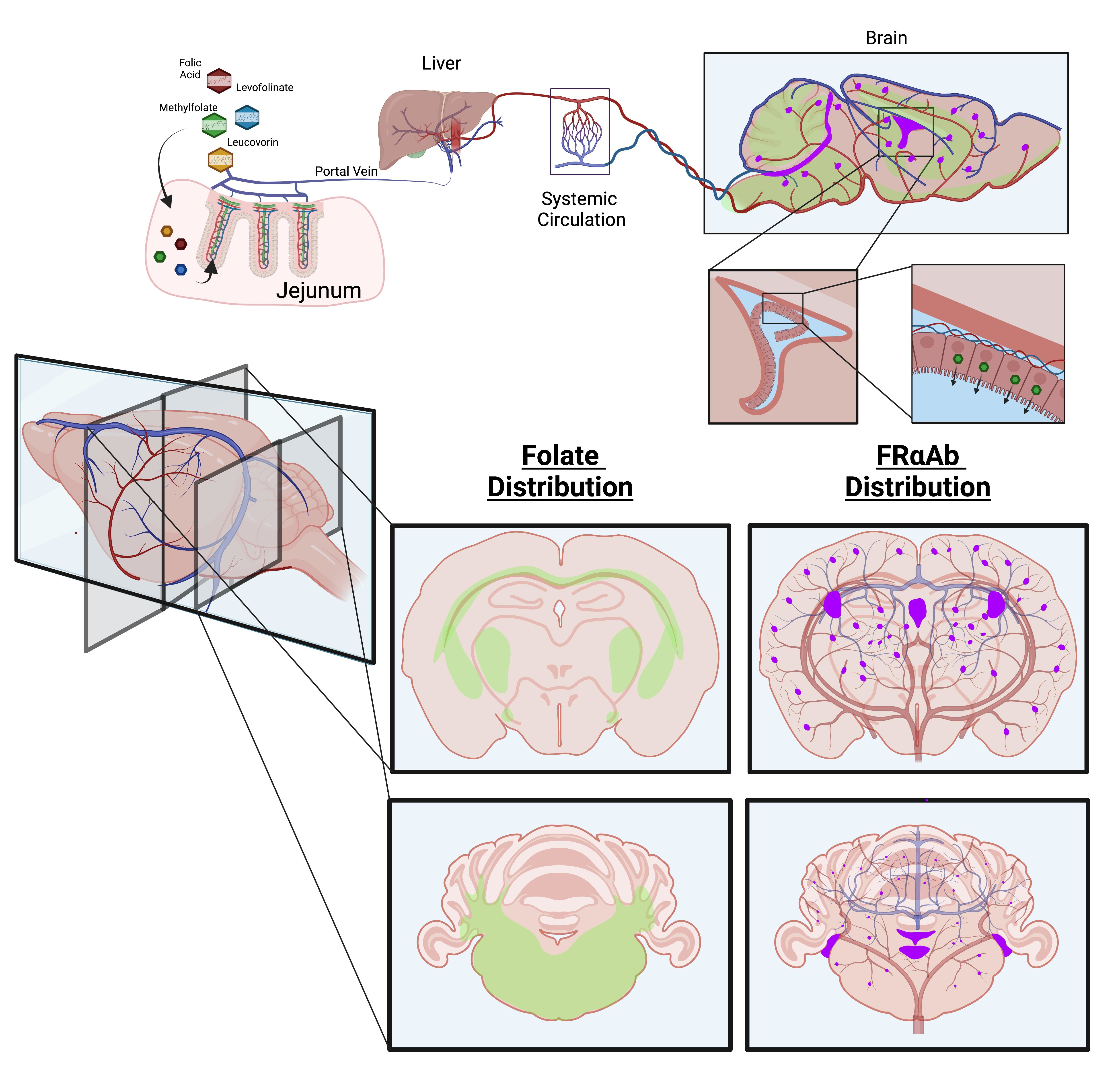

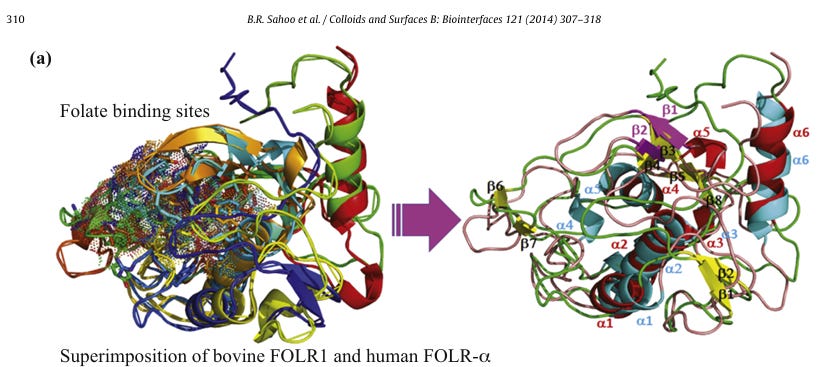
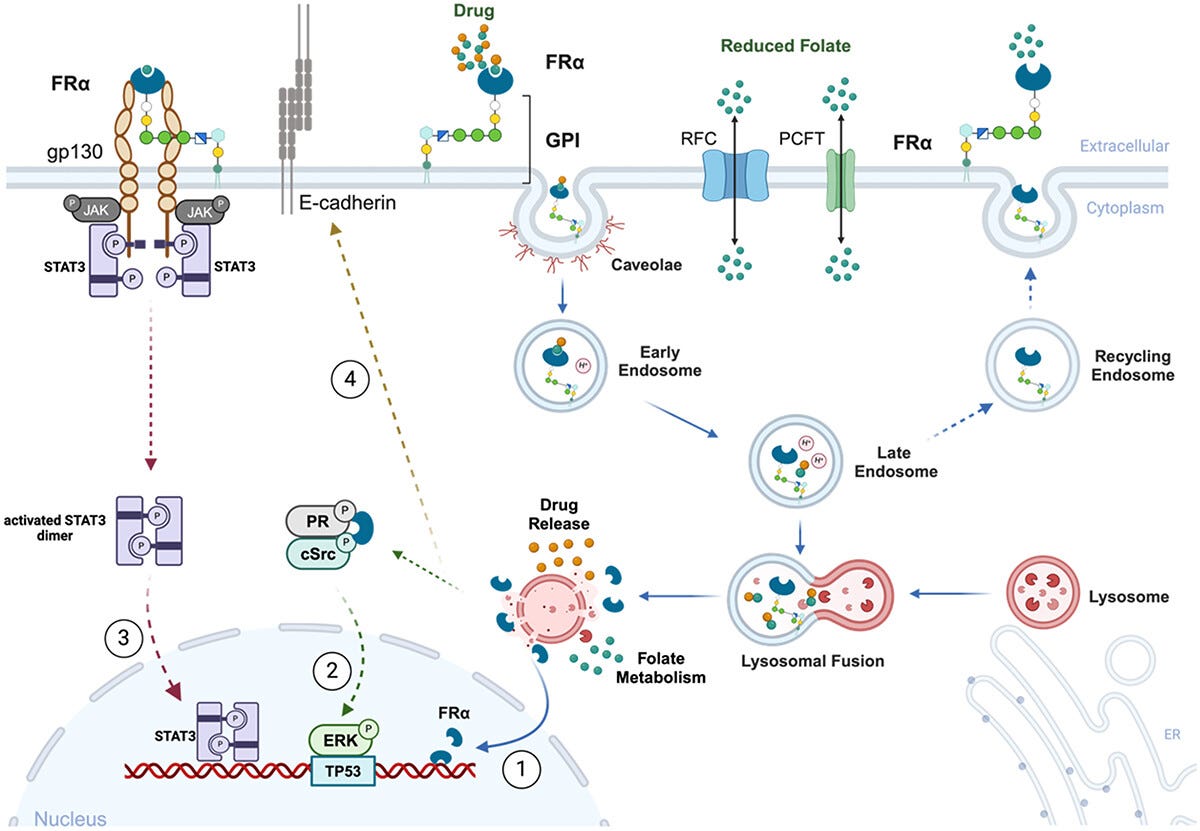



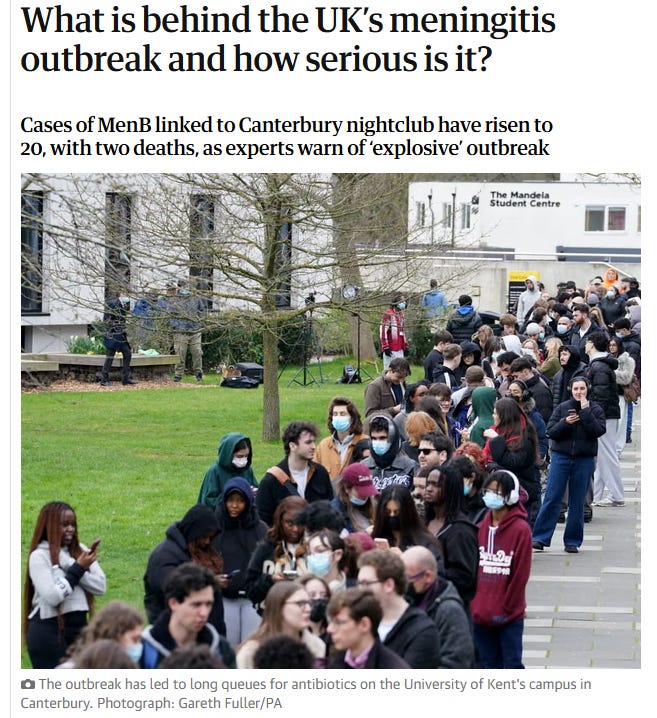


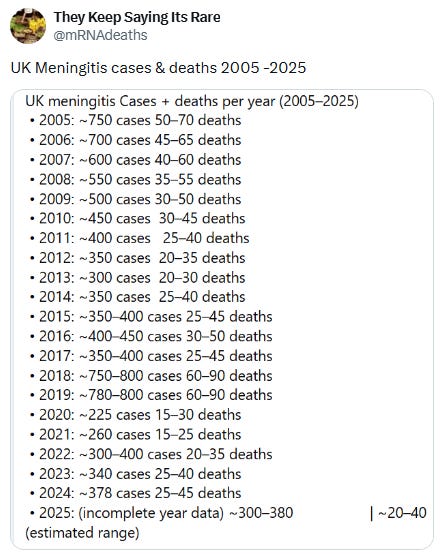


OurWorldinData.org/causes-of-death | CC BY
KENT
BBC Kent
@BBCRadioKent · Mar 20
A meningitis vaccination programme has been
expanded following a deadly outbreak in
Canterbury - with university students queuing for
hours for jabs.
...
BBC
RADIO KENT
Filmed on 19.02.2026
so - when the girl was in
there who had it.
The girl was there who had it
11 0:52
cc
10:23 PM · Mar 21, 2026 · 1,922 Views")




Cow's milk protein contaminated vaccines cause 75% of autism cases
https://vinuarumugham.substack.com/p/cows-milk-protein-contaminated-vaccines
Vaccines cause Autoimmune Diseases and Autism
https://zenodo.org/records/14942329
Autism pathogenesis: Piecing it all together, from end to beginning …
https://zenodo.org/records/2054221
A life changing article and I hope it’s okay if I bring parts of it to the pediatric neurologist of my daughter. I cannot tell you how much of my little free time I have spent trying to unlock the mysteries of “leucovorin”. I looked everywhere for studies with every search word you can imagine, it took months to find even that meta data study (which is actually only based on 2 studies) and the adult onset Cerebral Folate Deficiency study. I was baffled at how this stuff was memory holed. Then I watched in real time as my favorite recent study, which was double blind and randomized (the gold standard for the credentialist doctors) was retracted! I still don’t know what data was “falsified” (that is how Cremieux on X described it- outrageous) so that I could see whether the retraction was justified or not.
On a personal note, my other daughter with high functioning autism (mostly crippling anxiety) has been taking folinic acid (the over the counter version is only .8mg so I have to give many) and she has explained to me how it has been life changing with so much of her anxiety drifting away. She is SO much better. Also, my mother and maternal grandmother both died of ovarian cancer. So we quite obviously have an FRAA problem.
I am eternally grateful for you doing this deep dive, it’s mentally crippling to have this information and see how many people could be benefiting from folinic acid and know that you will never be heard. I hope many people read you article and try it, its water soluble so the excess should be easily excreted. Thank you from the bottom of my heart, I’m not crazy.