


Nuclear medicine: 18F-FDG PET/CT for the detection of vaccine-induced pathologies

Reading time: novelette
TL;DR: PET scans have revealed that mRNA shot induced heart damage is in fact very common. Post shot or infection induced chronic inflammation may persist for years, contributing to the symptoms of “long Covid” and with elevated cardiovascular & cancer risk. A majority of deaths recorded as “natural causes” were associated with a shot in the last 30 days.
Explain it like I'm five: The doctor puts a magic sugar in you that makes your poorly bits glow so that he can see them.
Also available in:
Any extracts used in the following article are for non-commercial research and educational purposes only and may be subject to copyright from their respective owners.

Contents
18F-FDG uptake at PET/CT as a tool to detect vaccine induced pathologies
What diseases are 18F-FDG PET/CT scans an important diagnostic tool for?
How did they conduct the study of 18F-FDG uptake in mRNA transfected and non-transfected patients?
Persistent endothelial dysfunction in post-COVID-19 syndrome (PCS)
Chronic inflammation is linked to sudden adult death due to atrial fibrillation
mRNA “vaccine” persistence and cardiac involvement
Myocardial LNP infiltration & reperfusion injury
Cancer risk from chronic and sustained stimulation of the immune system
Somatic mutations: cancer is a continuum
Introduction
Back on 23rd December I reviewed an abstract by R Gundry “Correction to: Abstract 10712: Mrna COVID Vaccines Dramatically Increase Endothelial Inflammatory Markers and ACS Risk as Measured by the PULS Cardiac Test: a Warning”.
The title tells the story:
Study of clinical data finds that experimental mRNA shots increase your 5yr risk of acute coronary syndrome (ACS) from 11% to 25%

Any extracts used in the following article are for non-commercial research and educational purposes only and may be subject to copyright from their respective owners. Substack limitations Once Substacks’ support the use of internal hyperlinks I will add them to the abstract. Otherwise please use a “Find In Page” keyword search to navigate or click on the …
Acute coronary syndrome (ACS) refers to a group of conditions that include ST-elevation myocardial infarction (STEMI), non-ST elevation myocardial infarction (NSTEMI), and unstable angina. It is a type of coronary heart disease (CHD), which is responsible for one-third of total deaths in people older than 35. Some forms of CHD can be asymptomatic, but ACS is always symptomatic
From: “Acute Coronary Syndrome” (2023)
The so called “fact checkers” attacked the piece. All they could manage was a lot of arm waving without striking a blow.
Even so, without access to the full paper we really needed more data. We needed to know about subsets and their proportional risk - young, old, male, female, how many boosters? Do the markers (and damage) self resolve after a few months?
We got some answers in July from a study of Swiss hospital employees: "Sex-specific differences in myocardial injury incidence after COVID-19 mRNA-1273 booster vaccination”, published by Buergin et al.1
Its useful to describe what a troponin test is measuring:
…The Troponin T test is a simple blood test that is performed to measure the level of troponin in the blood. Troponin is a protein that is found in the heart muscles and not in the blood. The level of troponin increases in the blood only if the heart muscles are damaged, like during a heart attack.
There are several other reasons as well that may cause elevated Troponin T levels in the blood, but a heart attack is the most common among them.
…Understanding the Troponin T Test Results
Generally, the troponin T levels in the blood are undetectable with regular blood tests, as the protein is normally present in trace amounts in the blood. The normal value of troponin T in the blood is generally less than 0.04 ng/ml. However, the normal range of troponin T levels is different for men and women and may also vary from one lab to another. A value above 0.40 ng/ml may indicate elevated risks of an individual having a heart attack.
From: “Troponin T Test Results, Normal Range and More” (2022)
https://www.apollodiagnostics.in/blog/troponin-t-test-results-normal-range-and-more
Key takes from "Sex-specific differences in myocardial injury incidence after COVID-19 mRNA-1273 booster vaccination”:
Oligosymptomatic: Having few symptoms.
Aims
To explore the incidence and potential mechanisms of oligosymptomatic myocardial injury following COVID-19 mRNA booster vaccination.
Methods and results
Hospital employees scheduled to undergo mRNA-1273 booster vaccination were assessed for mRNA-1273 vaccination-associated myocardial injury, defined as acute dynamic increase in high-sensitivity cardiac troponin T (hs-cTnT) concentration above the sex-specific upper limit of normal on day 3 (48–96 h) after vaccination without evidence of an alternative cause.
hs-cTnT: high-sensitive cardiac troponin T. Normal range <14 ng/L2.
To explore possible mechanisms, antibodies against interleukin-1 receptor antagonist (IL-1RA), the SARS-CoV-2-nucleoprotein (NP) and -spike (S1) proteins and an array of 14 inflammatory cytokines were quantified. Among 777 participants (median age 37 years, 69.5% women), 40 participants (5.1%; 95% confidence interval [CI] 3.7–7.0%) had elevated hs-cTnT concentration on day 3 and mRNA-1273 vaccine-associated myocardial injury was adjudicated in 22 participants (2.8% [95% CI 1.7–4.3%]).
Twenty cases occurred in women (3.7% [95% CI 2.3–5.7%]), two in men (0.8% [95% CI 0.1–3.0%]). Hs-cTnT elevations were mild and only temporary. No patient had electrocardiographic changes, and none developed major adverse cardiac events within 30 days (0% [95% CI 0–0.4%]). In the overall booster cohort, hs-cTnT concentrations (day 3; median 5, interquartile range [IQR] 4–6 ng/L) were significantly higher compared to matched controls (n = 777, median 3 [IQR 3–5] ng/L, p < 0.001). Cases had comparable systemic reactogenicity, concentrations of anti-IL-1RA, anti-NP, anti-S1, and markers quantifying systemic inflammation, but lower concentrations of interferon (IFN)-λ1 (IL-29) and granulocyte-macrophage colony-stimulating factor (GM-CSF) versus persons without vaccine-associated myocardial injury.
“Mild and transient”? I would take issue with this generalisation - how can they know the long term prognosis?
Conclusion
mRNA-1273 vaccine-associated myocardial injury was more common than previously thought, being mild and transient, and more frequent in women versus men. The possible protective role of IFN-λ1 (IL-29) and GM-CSF warrant further studies.
You may have shot induced heart damage, but no abnormal symptoms to warn you to not drink excessively and avoid competitive sports and exercise3:
None of the participants with elevated markers of myocardial injury related to mRNA vaccination had a history of cardiac disease (online supplementary Table S5). Eleven participants (50%) had unspecific symptoms including fever and chills, two had chest pain, and none had ST-segment depression or T-wave inversion (online supplementary Table S5). Pre-defined and prospectively recorded symptoms occurred with comparable frequency in participants developing mRNA-1273 vaccine-associated myocardial injury versus those that did not.
No definitive case of myocarditis was found. However, the two participants (both women) with vaccine-associated myocardial injury and chest pain met the Brighton Collaboration case definition Level 2, indicating probable myocarditis in those patients (0.3% [95% CI 0.1–0.9%]).13
In other words, this study found evidence of “vaccine-associated myocardial injury” in just under 3% of employees after only 2 doses of Moderna mRNA-1273. Another 2% of employees had markers for myocardial muscle damage.
An analysis of new onset cardiac symptoms after the trivalent influenza vaccine also found that 2.8% had been vaccine injured, 1% seriously. I would expect the new quadrivalent annual boosters to be worse still due to the inclusion of more epitopes, i.e. increased immunogenicity:
Would care workers with fluvax induced heart damage have been excluded from this study? Only if a cardiac event or surgery occurred in the 30 days prior to mRNA transfection. The patients’ histories made picking out the signal from the noise quite challenging:
In the absence of a baseline hs-cTnT concentration immediately prior to the vaccination, strict criteria were applied in the adjudication of COVID-19 mRNA-vaccine-associated myocardial injury. For the differentiation of acute COVID-19 mRNA-vaccine-associated myocardial injury versus possible chronic preexisting myocardial injury, four criteria were used.
No dosing adjustments are ever used, other than for child formulations.
+ See “How Do We Determine The Correct Dose of a Treatment?”: https://www.midwesterndoctor.com/p/how-do-we-determine-the-correct-dose?utm_source=profile&utm_medium=reader2
The significantly higher rate of mRNA-1273 booster vaccination-associated myocardial injury in women versus men may at least partly be related to the higher vaccine dose per body weight or myocardial mass in women and therefore dose-dependent toxic effects. Clinically overt severe vaccination-associated myocarditis may then occur following a second hit, possibly mediated by neutralizing autoantibodies targeting IL-1RA, microvascular thrombosis, or direct cardiac myocyte injury unrelated to inflammation.8, 23
Other studies also found a relatively high incidence of myocardial injury:
Our findings following mRNA-1273 booster vaccination extend and corroborate observations in two recent active surveillance studies after BNT162b2 vaccination.24, 25 Among 324 healthcare workers (mean age 51 years, 59.2% women) who received a fourth dose of BNT162b2 in Israel, two participants (one woman and one man) developed vaccine-related myocardial injury on day 3 (incidence 0.6%, maximum hs-cTnI concentration 22.1 ng/L). One had mild symptoms including fever and chest pain, one was asymptomatic. Both had a normal ECG and echocardiography.24
Among 301 adolescents in Thailand (mean age 15 years) receiving the second dose of BNT162b2, five participants (incidence 1.7%), all boys, developed vaccine-related myocardial injury on either day 2 or day 3.25 One of them had very high hs-cTnT concentrations (593 ng/L) and late gadolinium enhancement indicating myocarditis on cardiac magnetic resonance (CMR) imaging. When comparing these studies, it is important to highlight major differences in the study population and study methodology.
Therefore, the main finding of this study, that subclinical mRNA vaccine-associated myocardial injury is much more common than estimated based on passive surveillance, has been confirmed and generalized in these complimentary cohorts of slightly older healthcare workers in Israel and adolescents in Thailand. Additional active surveillance studies are needed to externally validate two specific findings of this study: the even higher rate of mRNA-1273 booster vaccination-associated myocardial injury overall, and particularly in women.
On this last point, the reason for this Substack is that on 19th September an additional study was published. Highlighting the value of PET/CT scans as a diagnostic tool, this study provides further strong evidence that some degree of heart damage is being induced in almost all those boosted at least twice.
Hat tip to Dr. Janci, microbiologist and toxicologist, for posting the link4.

18F-FDG uptake at PET/CT as a tool to detect vaccine induced pathologies
Nuclear medicine techniques are non-invasive tools that can early detect pathophysiological changes in affected tissues in patients with inflammatory or infectious diseases. These changes usually occur before clinical onset of symptoms and before the development of anatomical changes detected by radiological techniques [1, 2].
From: “Evidence-Based PET for Infectious and Inflammatory Diseases” (2020)
https://link.springer.com/chapter/10.1007/978-3-030-47701-1_12
In July I reviewed a case report of a 66 year old man who was diagnosed with new-onset cervical lymphadenopathies in 2021 after being administered two doses of BNT162b2 mRNA.
Detailed in the case report, a 18F-FDG PET/CT scan detected multiple, enlarged hypermetabolic lymphadenopathies above and below the diaphragm as well as several hypermetabolic lesions outside of the lymph nodes. As this had all the signs of a stage IV lymphoma they performed a biopsy.
Follicular helper T cell marker findings and next generation sequencing (NGS) performed on the biopsy sample detected genetic mutations and unambiguously established the diagnosis of AngioImmunoblastic T cell Lymphoma (AITL), pattern 2.
There was no significant medical history or indications of cancer prior to this, but the authors speculate that these mutations put him at risk of lymphoma induction.
The authors of the paper were perplexed by the lack of interest in their findings. And with such dismissive studies as “PET findings after COVID-19 vaccination: “Keep Calm and Carry On””5 you can see their point. Dreadful.

From “Rapid Progression of Angioimmunoblastic T Cell Lymphoma Following BNT162b2 mRNA Vaccine Booster Shot: A Case Report”6 (emphasis mine):
…Interestingly, in none of these studies, the possibility that the mRNA vaccines could have played a role in the development of malignant lymph nodes was considered. Indeed, the consensus so far is that the occurrence of hypermetabolic lymphadenopathies should not question the safety of mRNA vaccines, neither in healthy individuals nor in patients with neoplastic conditions.
mRNA gene agent induced turbo-cancer:
…the dramatic speed and magnitude of the progression manifested on two 18F-FDG PET-CT performed 22 days apart. Such a rapid evolution would be highly unexpected in the natural course in the disease.
…In fact, the supposed enhancing action of the vaccine on AITL neoplastic cells is fully consistent with previous observations identifying TFH cells within germinal centers as key targets of nucleoside-modified mRNA vaccines both in animals and in man (1, 2). Malignant TFH cells, the hallmark of AITH, might be especially sensitive to mRNA vaccines when they harbor the RHOA G17V mutation which was present in our case. Indeed, this mutation facilitates proliferation and activation of several signaling pathways in TFH cells (16).
…Our case first raises the question of the COVID-19 prevention strategy to be used in this patient which is currently poorly protected against COVID-19…On the longer term, the use of mRNA vaccines should clearly be avoided while other types of vaccines might be considered.
Full review:
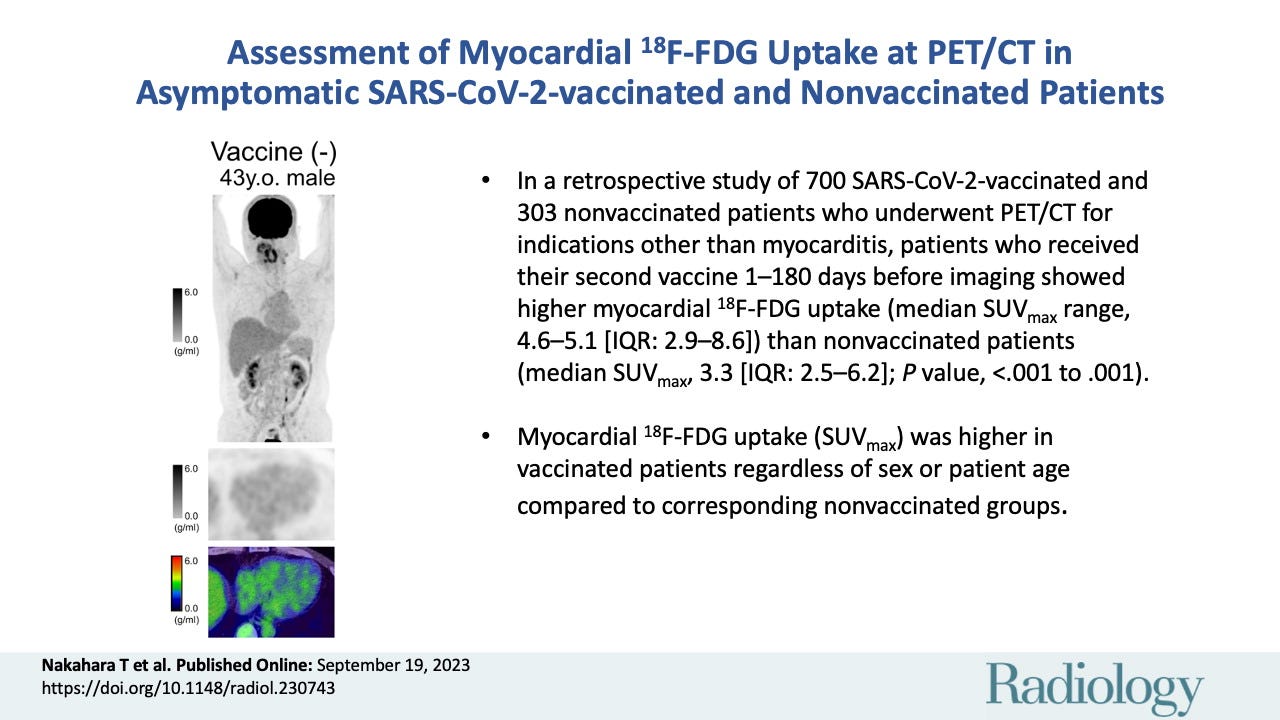
Our new study by Nakahara et al: "Assessment of Myocardial 18F-FDG Uptake at PET/CT in Asymptomatic SARS-CoV-2-vaccinated and Nonvaccinated Patients" was published on 19th September ‘23 in volume 308 of “Radiology”7.
As my specialism concerned plant pathology & biochem many years ago I will walk through with questions that I have as a layman to nuclear medicine.
What is a PET/CT scan?
A positron emission tomography (PET) scan produces detailed 3D images of the inside of the body. A PET scanner works by detecting the radiation given off from a radiotracer as it collects in different tissues and organs.
What is 18F-FDG?
18F-FDG, or 18Fluorine-fluorodeoxyglucose has similar pharmacokinetic properties to glucose, i.e. it acts as a glucose analogue. 18F denotes an isotope of Fluorine, which gives FDG its properties as a radiotracer.
Decaying by positron emission to yield stable 18oxygen,18F has a short half life of only 20 minutes8. You won’t be glowing afterwards unless you’ve been double vaxxed first:

What is a positron?
A positron or antielectron is the antiparticle or antimatter counterpart of the electron. It has the same mass but the opposite charge. If a positron collides with its antimatter nemesis then the two are annihilated, but at lower energies a collision results in photons being emitted9.


Scintillation crystals in the PET cameras absorb energy from these photons, producing light that is converted into an electrical signal:


How does it work?
A kinase reversibly adds a phosphate group (PO4) to the polar group R of various amino acids. This is an important cellular regulatory mechanism as many enzymes and receptors are activated/deactivated by phosphorylation and dephosphorylation events. In turn, a phosphatase (-ase = enzyme) can remove or dephosphorylate the target and deactivate it10.
The initial enzyme of glycolysis, hexokinase, catalyses the conversion of glucose to glucose-6-phosphate (G6P). The concentration gradient from this reaction facilitates the diffusion of glucose via the glucose transporters GLUT1-13.
Rapid phosphorylation traps the glucose molecule inside the cell as the cell membrane is impermeable to G6P.
Healthy cells then metabolize the G6P in different ways, according to energy demands and regulatory mechanisms.
18F-FDG is analogue of the glucose molecule but instead of a hydroxyl group (-OH) it has the radioactive tracer Flourine-18:
 - Wikipedia")
So we can picture an equilibrium level of 18F-FDG in a healthy cell as it builds to a level until glucose-6 phosphatase (G6Pase) action allows GLUT2 to release it from the cytosol to the bloodstream (cytosol is a semi-fluid substance filling the interior of the cell and embedding the other organelles and subcellular compartments).
G6Pase is only expressed in the liver, kidneys, and intestine11.
But tumour cells typically lack sufficient G6Pase so the radioactive 18F tracer accumulates relative to healthy tissue. A high rate of glycolysis and excessive expression of glucose transporters further increases the concentration, which is then detected by the PET scanner.
Tumour cells are often metabolically highly active and hungrier for energy than efficient oxidative phosphorylation (OXPHOS) can provide via the glycolytic pathway, so they switch to the pentose phosphate pathway (PPP). The PPP does not use ATP or oxygen, even in aerobic conditions.
This may be likened to setting the frying pan on fire instead of using an efficient blue flame.

In reality, cancers are extremely diverse diseases with each having its own metabolic features. This differentiation exists right down to individual tumour cell phenotypes. OXPHOS still contributes to energy production and may play a major role in some cancers12.
There are a few more steps involving intermediate metabolites than are illustrated, but this is a useful overview of the pathways:

The Warburg Effect (WE) is defined as “an increase in the rate of glucose uptake and preferential production of lactate, even in the presence of oxygen”13 and discussed along with the Kynurenine pathway in a Substack from July ‘22.
One hypothesis is that some of the pathophysiology of COVID-19 is because SARS-CoV-2 mimics the WE:
Both John Paul and Jennifer Depew (R.D) have written some excellent Substacks relating to this and metabolism1415.
PET scanning the accumulation of 18F-FDG is a useful cancer diagnostic tool as glycolysis is associated with a tumour microenvironment (TE) that is conducive to cancer progression:
Many studies have found that glycolysis promotes tumor growth, metastasis, and chemoresistance, as well as inhibiting the apoptosis of tumor cells. In addition, lactic acid, a metabolite of glycolysis, can also accumulate in the TME, leading to reduced extracellular pH and immunosuppression, and affecting the TME.
From: “The significance of glycolysis in tumor progression and its relationship with the tumor microenvironment” (2022)
What diseases are 18F-FDG PET/CT scans an important diagnostic tool for?
Neoplasms
FDG/PET can detect metabolic changes in neoplastic cells even before the tumour size has increased.
Cancer cells require a high level of a cofactor called nicotinamide adenine dinucleotide phosphate (NADPH) to produce the fats and proteins needed for rapid cell division. The increased demand for NADPH requires activation of the Warburg Effect or aerobic glycolysis as it is derived from the PPP.
Spike protein, both viral and synthetic, can also deplete NADPH.
The mechanism involved is S protein binding to ACE2, which leads to increased concentration of Ang II as ACE2 is no longer available to convert Ang II to Ang 1-7.
The resultant Ang II then binds to the angiotensin type 1 receptor (AT1R) which stimulates NADPH activity, resulting in excessive superoxide production (ROS) and consumption of NADPH as it is an electron donor16. NADPH is the unique provider of antioxidative defence systems in a cell.
A paper I would like to see would investigate the effects of spike protein induced NADPH deficiency on the tumour TME, as competition should lead to more cells switching to glycolysis, with associated immunosuppression and disease progression.
So I did a quick search of PubMed and Malkani & Rashid also discussed the hypothesis back in 2021, but relating specifically to lung cancer.
Unfortunately they don’t provide experimental data:
Several SARS-Co-V2 proteins can modulate the lung TME by disrupting the fragile immune mechanisms contributing to cytokine storming and cellular metabolic variations. We also discussed the impact of medication used for lung cancer in the scenario of this infection. Since other respiratory infections can be a risk factor for lung cancer, COVID-19 recovered patients should be monitored for tumor development, especially if there is genetic susceptibility or it involves exposure to other risk factors.
…SARS-CoV-2 proteins might interact with the components of TME and may support tumor growth or cause resistance to the ongoing therapy.
From: “SARS-COV-2 infection and lung tumor microenvironment” (2021)
They mention “…the abundance of viral spike protein binding receptors to the host cells in the lungs” - why don’t they suggest monitoring mRNA transfected patients for tumour development too?
I think we know the answer.
Myocarditis
Free fatty acids are the primary energy source for heart muscle (myocardium). But if inadequate blood flow occurs (ischemia) then myocardium metabolism changes to anaerobic glucose metabolism.
A key point is that injured myocytes that may recover can use glucose, but irreversibly injured myocytes cannot. In other words FDG accumulation is associated with reversible heart injury once the blood flow is restored.
Irreversible loss of systolic function with a reduced accumulation of FDG indicates a low likelihood of recovery after revascularisation surgery.
A timely diagnosis of myocarditis assisted by FDG PET can change case management decisions, limiting further damage and improving the quality of life and prognosis17. You will also know to cut down on your drinking and heavy workouts.
Atherosclerosis
Increased metabolic activity of macrophages in the atherosclerotic plaque, particularly in large vessels like the aorta are responsible for FDG uptake. Smooth muscles in artery walls can also take-up FDG and become visible with PET18.
Infections and inflammation
The high rate of glycolysis of inflammatory cells leads to FDG uptake and FDG-PET can be used to detect sites of infection and inflammation. It has particular value in the diagnosis of orthopaedic infections related to osteomyelitis or implanted prostheses.
FDG-PET is also useful for detecting inflammation associated with sarcoidosis, vasculitis, rheumatological diseases and regional ileitis (Crohn’s).
How did they conduct the study of 18F-FDG uptake in mRNA transfected and non-transfected patients?
Their analysis was conducted retrospectively, investigated asymptomatic patients and took advantage of a large repository of 18F-FDG PET-CT scans. These were taken not to investigate myocarditis or vaccines but for other reasons - primarily oncological evaluation.
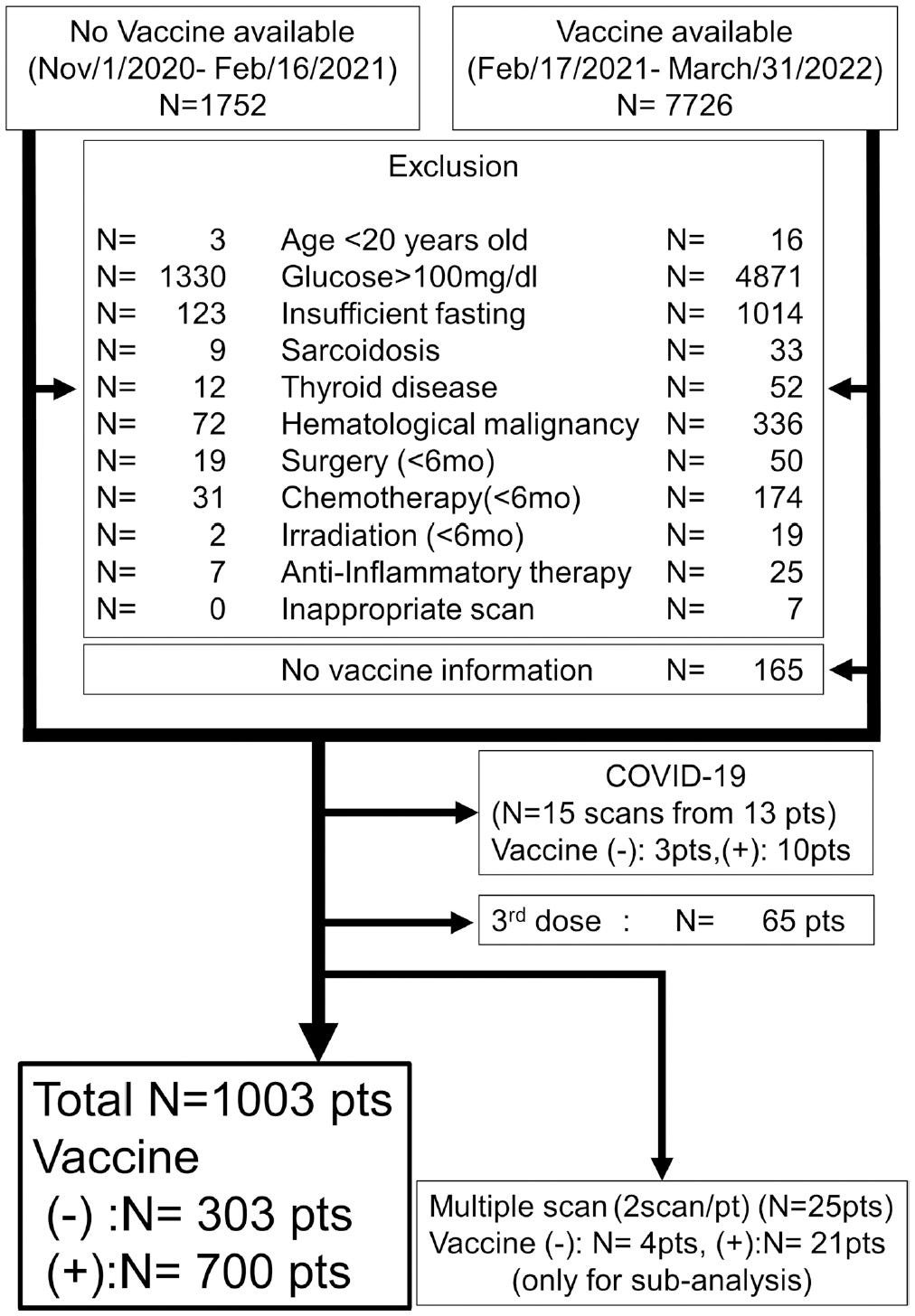
Starting out with records from 9,478 patients who had PET/CT over about 16 months many scans were excluded due to a variety of reasons:
Those with high overall cardiac metabolic activity despite fasting before the scan. Myocardium can use alternate energy sources than glucose after this is exhausted: ketones, amino acids and free fatty acids - lipids being preferred over glucose. This is important so that glucose from the tracer has more chance of accumulating and being detected in inflamed myocardium, due to the increased metabolic rate. Without prior fasting the metabolic rate would be too high due to ordinary glucose being used and you wouldn’t get a good contrast.
6,201 patients with blood glucose levels greater than 100mg/dl at the time of the scan.
1,137 patients due to insufficient fasting before the scan.
Others due to confounders including sarcoidosis, chemo or radiotherapy that might have also increased tracer activity. 19 patients were excluded as being < 20 years old - the age group at most risk of myocarditis.
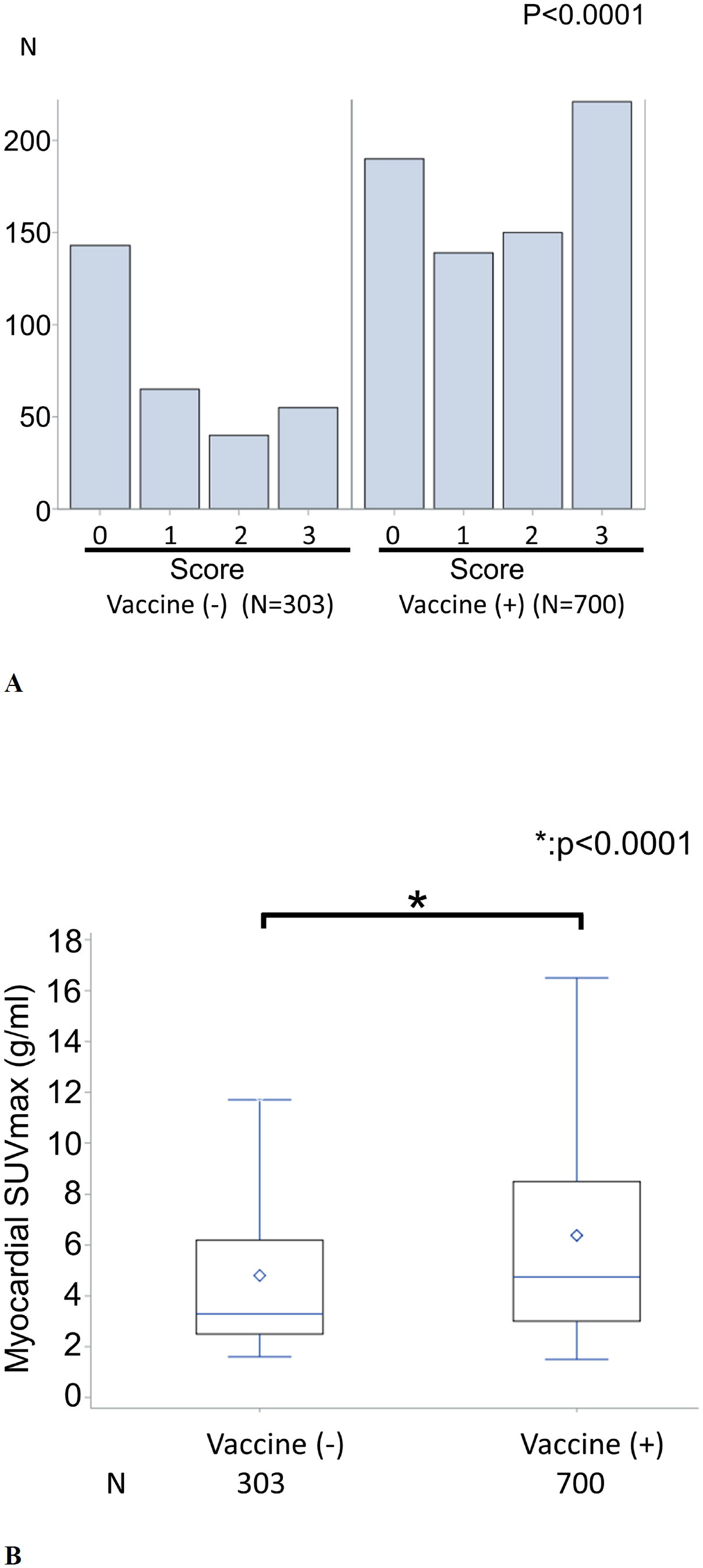
This led to the final study group of 1003 patients. 303 were unvaccinated before PET and 700 vaccinated - 660 of these with two doses. Myocardial visual scores were then applied ranging from 0 (minimal tracer uptake) to 3 (homogeneous uptake):
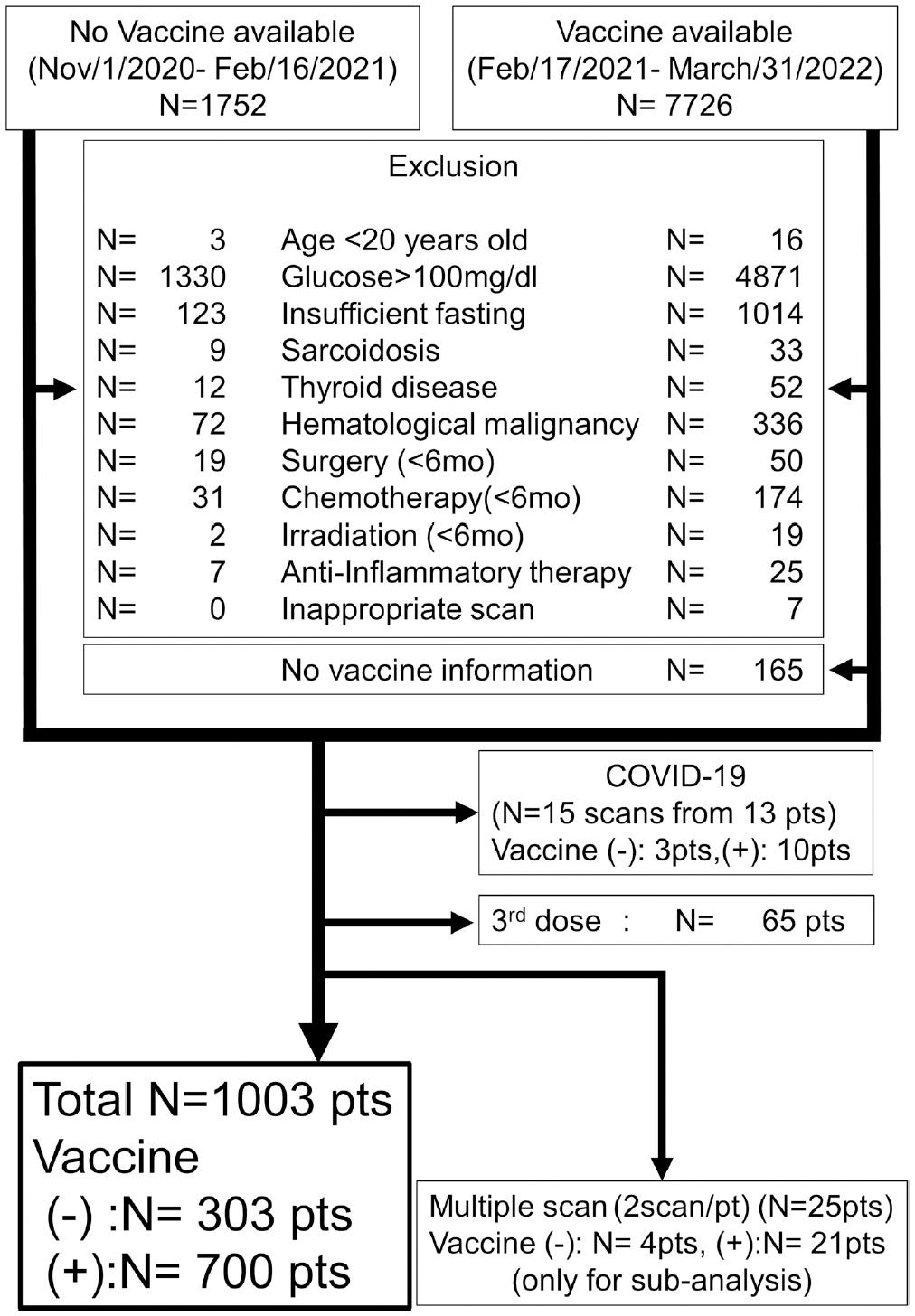
From: “Figure 1: Flow diagram of patient exclusion”. Source: https://pubs.rsna.org/doi/10.1148/radiol.230743
After uploading to a workstation the scans were reconstructed into different views using “Universal Viewer” by two observers and inspected by an expert in nuclear medicine, also under independent and blinded observation.

Statistical analysis techniques were then applied to calculate the myocardial maximum standardized uptake value (SUVmax). This is also widely used for measuring the uptake of FDG by malignant tissue19.
What were the key findings?
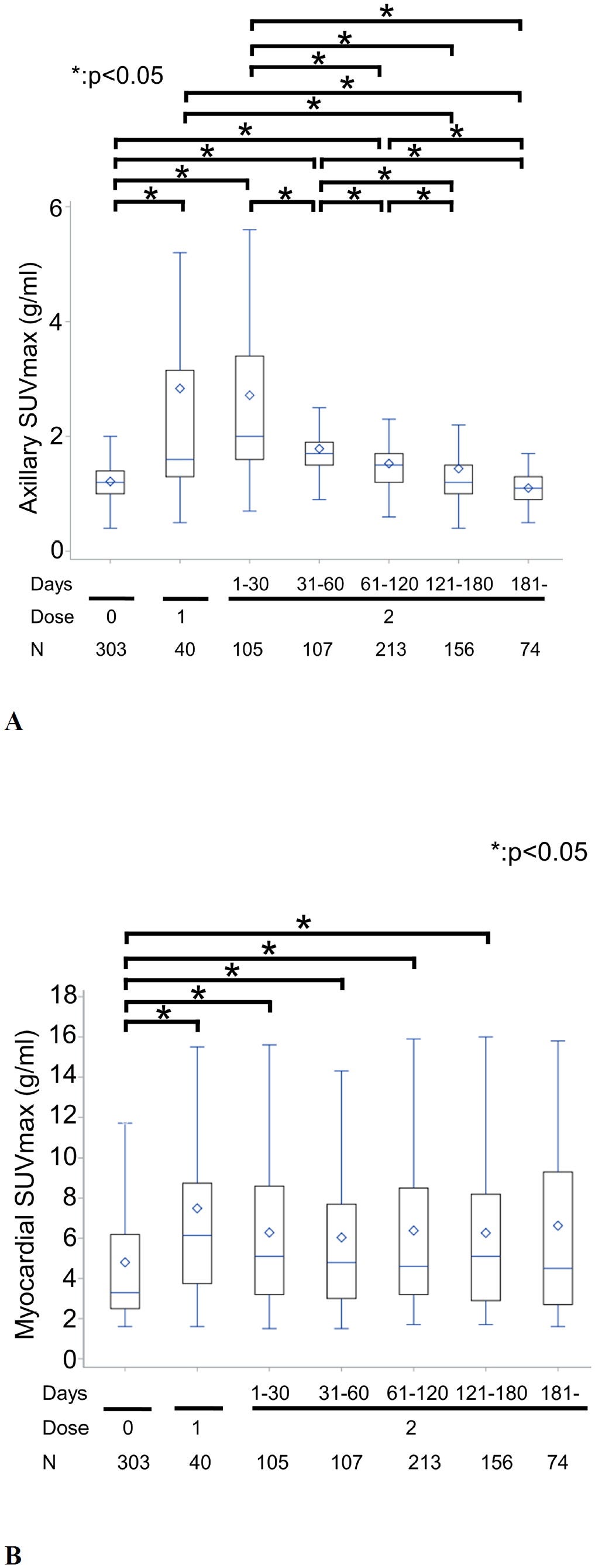
A key finding was that asymptomatic patients transfected 1-180 days before PET had a 39-55% higher myocardial 18F-FDG uptake than the un-transfected (median SUVmax range 4.6-5.1 vs a median SUVmax range 3.3-3.3).
Although described as “asymptomatic”, absence of evidence is not evidence of absence,20 - it may simply have been unreported or ascribed to other causes.
The interquartile range (IQR) measures the spread of the middle half of the data, ie the range for the middle 50% of values.
The low P value indicates a less than 1 in 10,000 chance of these results occurring by chance:
The axillary lymph nodes or armpit lymph nodes are lymph nodes in the human armpit. Between 20 and 49 in number, they drain lymph vessels from the lateral quadrants of the breast, the superficial lymph vessels from thin walls of the chest and the abdomen above the level of the navel, and the vessels from the upper limb. They are divided in several groups according to their location in the armpit. These lymph nodes are clinically significant in breast cancer, and metastases from the breast to the axillary lymph nodes are considered in the staging of the disease.
From: “Axillary lymph nodes”
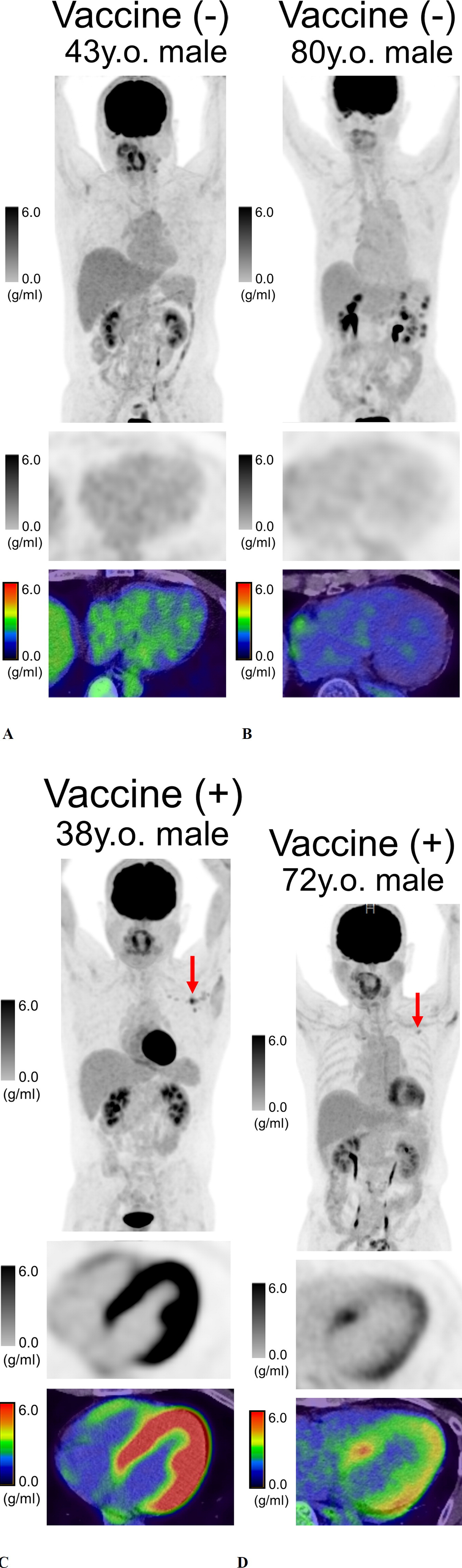
From “Figure 2”, A and B are un-transfected, C and D are transfected.
Comparative SUVmax scores:
A: (43 y/o male, medical checkup): myocardial 2.0; axillary 0.6; liver 2.8; spleen 2.1
B: (80 y/o male, pancreatic cancer): myocardial 2.2; axillary 1.1; liver 2.2; spleen 1.5
C: (38 y/o male, medical checkup): myocardial 14.6; axillary 2.0; liver 2.0; spleen 2.1
D: (72 y/o male, medical checkup): myocardial 5.9; axillary 2.7; liver 2.6; spleen 2.1
From “Figure 3” we see an overview of findings.
in A we see on the left “unvaccinated” myocardial FDG uptake visual scores and on the right “vaccinated”, with N denoting the number of patients. Lower scores are better.
In B we see the same stratification, but showing myocardial FDG uptake as measured by SUVmax. Lower is better.
Horizontal bars represent the median SUVmax value and whiskers the interquartile range. The blue diamond represents the average value:
From “Figure 4”, A shows boxplots of axillary 18F-FDG uptake in the transfected. Dose 0 is the un-transfected group.
Lymph node 18F-FDG uptake above 2.5 is often used as a cut off value for malignancy21.
B shows boxplots of myocardial 18F-FDG uptake in the transfected.
Horizontal bars represent the median SUVmax value and whiskers the interquartile range. The blue diamond represents average - in both cases it remained above control to 180 days.
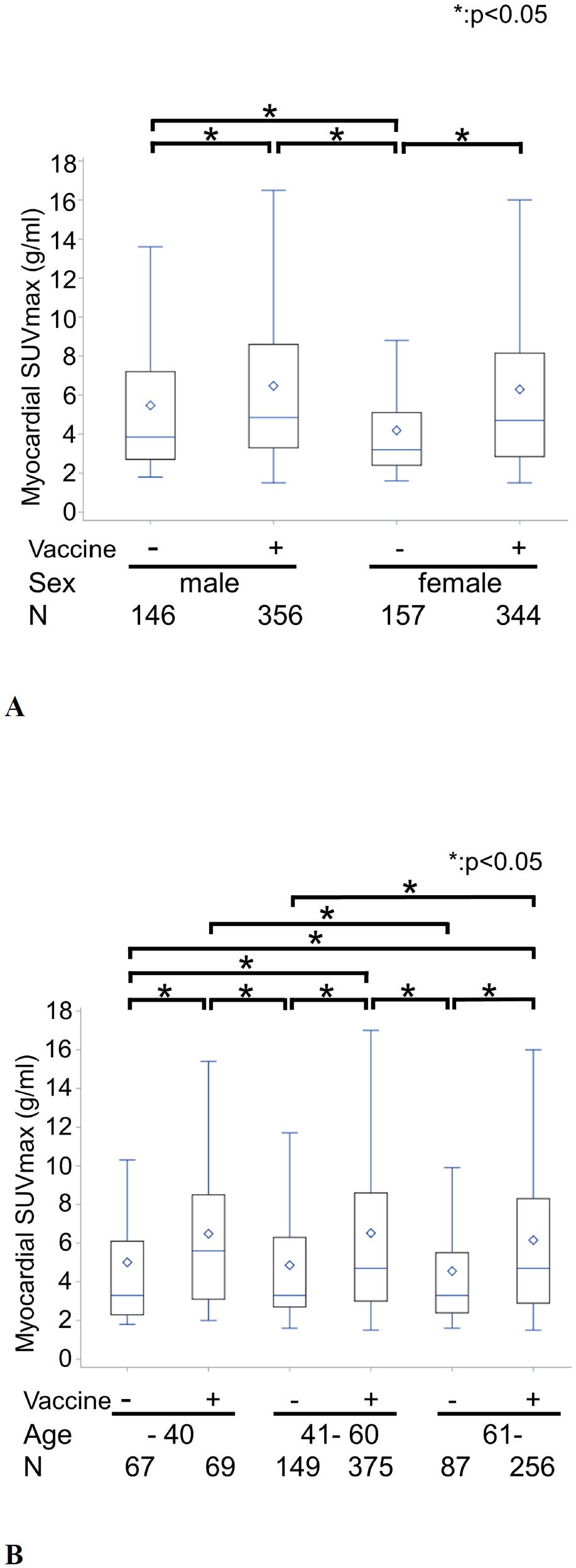
As for differences due to age or sex, “Figure 5” shows that myocardial FDG uptake was higher in every case in transfected vs un-transfected groups. Age made relatively little difference to outcomes, but males had a higher baseline SUVmax. After transfection this distinction was greatly reduced (4.9 vs 4.7).
What are we missing from the age groups? Although only 3 in number, those less than 20 y/o were excluded. You would expect a higher SUVmax in the young as post vax myocarditis cases are highest in those under 4022.
Axillary uptake was also higher in transfected males and females.
SUVmax before transfection: Males: 1.2; Females: 1.2
SUVmax after transfection: Males: 1.4 (+17%); Females: 1.5 (+25%)
From the “Figure 6” before-after comparisons the changes were as follows:
Comparative SUVmax scores:
A: 54 y/o female, vaginal cancer, before mRNA-1273 (Moderna):
Myocardial FDG uptake visual score: 1; myocardial SUVmax: 4.8
107 days after second dose of mRNA-1273:
Myocardial FDG uptake visual score: 3; myocardial SUVmax: 8.2
B: 67 y/o male, lung cancer, before BNT162b2 (Pfizer):
Myocardial FDG uptake visual score: 1; myocardial SUVmax: 4.8
72 days after second dose of BNT162b2:
Myocardial FDG uptake visual score: 3; myocardial SUVmax: 18.0

Closing comments
What we see from these studies are markers of a degree of medium to long term morphological changes, sustained up to the 180 day cut-off. Changes were seen in the axillary lymph nodes and especially the myocardium of the majority of those transfected.
More follow up studies are needed to determine the long term significance of this and to replicate the results. This may be challenging due to the lack of control groups but I consider possible consequences from other studies to conclude this Substack.
The authors would also like to see future comparisons of cardiac enzyme, cardiac function and non-mRNA vaccination. I would certainly agree with the latter, and I would like to see more oncological comparisons too.
We must also consider the risk of cumulative damage due to further booster doses (up to 6 at time of writing) or the annual flu and other shots.
Other studies and reports
Do the findings from the last study matter? After all the patients were reported as “asymptomatic”. Health service demand data shows that these results from studies like these do matter when extrapolated over time and to the wider population.
For example, on 24th September ‘23 “The Guardian” reported responses to freedom of information requests by the Liberal Democrats party:
The government is opening new community diagnostic centres but many patients face waits of several weeks for tests despite this additional investment.
The biggest increase was in the number of patients waiting for MRI scans, where the waiting list has jumped by a third and now stands at 280,000. For CT scans, it has shot up by 40,000 to 180,000.
The Lib Dems’ FoI request to NHS trusts found that the longest time for standard diagnostic scans was at Sandwell and West Birmingham NHS trust, where someone waited 914 days for an MRI scan, 665 days for a non-urgent X-ray, 693 days for an ultrasound and 367 days for a CT scan.
One person at Wye Valley NHS trust waited 49 weeks for an echocardiogram, while for an angiography, the longest reported wait was 475 days at Milton Keynes University hospital foundation trust.
From: “NHS England patients wait up to two-and-a-half years for an MRI”
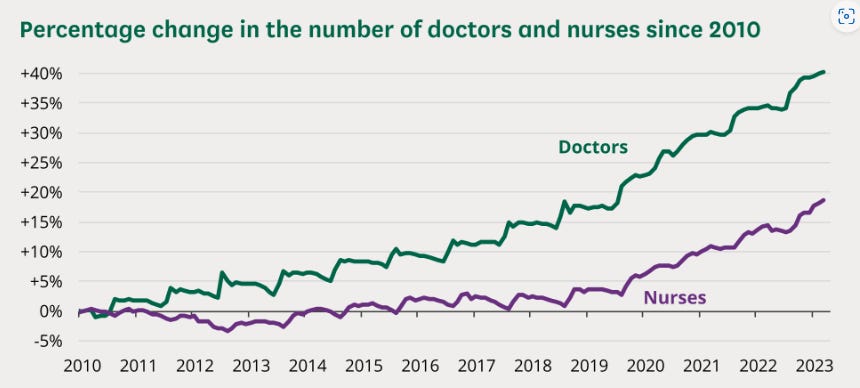
I reported on cancer waiting lists blowing out in the last Substack. Many services appear to be suffering from high demand which, although seasonal in nature, is feeding through to waiting lists despite an increase in doctors and nurses. They just cannot keep up with demand and many staff are on sick leave too:




Reports are coming in almost faster than I can type. This is tragic, doubly so if the cause is what I suspect it might be:

Persistent endothelial dysfunction in post-COVID-19 syndrome (PCS)
Published 28th July ‘23 and updated with funding information 23rd August ‘23, “Persistent endothelial dysfunction in post-COVID-19 syndrome and its associations with symptom severity and chronic inflammation” by Kuchler et al used Retinal Vessel Analysis (RVA) in a trial of 41 patients affected by PCS.
PCS is not an identifiable disease, it is a syndrome - “a recognizable complex of symptoms and physical findings which indicate a specific condition for which a direct cause is not necessarily understood”23. It may otherwise be referred to as “long Covid”, post-acute sequelae of COVID-19 (PASC), “VAIDS” or even “long vax”.
Prolonged endothelial dysfunction is a hallmark of PCS, atherosclerosis, hypertension and heart failure24. By studying the blood vessels of the eye they hypothesise that impairments of the microcirculation may explain persistent symptoms of PCS. These can include cardiovascular, metabolic and neurological related shortness of breath, chest pain, cognitive dysfunction, fatigue and palpitations.
You can use RVA parameters as clinical biomarkers to monitor disease progression and response to therapeutics.

What were the key findings?
Vax status was not given.
Patients who had been hospitalized with acute infection showed a tendency towards higher PCS severity scores (34.6 ± 9.3 vs. 45.6 ± 8.5, p = 0.07).
The median duration of PCS was ten months (7.0–18.0 months) with a mean PCS severity score of 35.7 (± 9.7). Fatigue (95.1%), exercise intolerance (90.2%), and brain fog (90.2%) were the three most abundant symptoms.
Eight (19.5%) patients were laid off, and the median cumulative time off sick leave was 122.0 days (4.0–291.0 days).
In our cohort, 60.9% (25/41) of PCS patients met the Canadian Consensus Criteria for ME/CFS. PCS patients with CFS were more obese (12.5% vs. 52.0%, p = 0.02); other CV factors were not different.
We observed significantly narrower retinal arterioles in PCS patients with CFS, indicated by lower CRAE (183.5 [177.4–197.0] vs. 174.0 [161.5–181.0], p = 0.03)
One study reported changes in retinal vessel diameters in acute SARS-CoV-2 infected patients, which resolved in non-severely affected patients after six months [48]. We could now show that PCS patients cannot restore primary damage to the endothelium. Since retinal vessel integrity is a surrogate of pan-endothelial health, persistent ED could partly answer persisting symptoms in PCS.
Elevated chemokine CXCL10 (also known as interferon γ-induced protein 10 or IP-10) is also associated with diseases such as HIV, hepatitis B, tuberculosis, cancer, diabetes and autoimmune disorders25. HIV gp120 also promotes CXCL10 expression26.
We showed that higher levels of CXCL10 and IL-6 both amplify the observed association between PCS severity and lower CRAE and AVR. CXCL10 binds to CXCR-A expressed by leukocytes and the isoform CXCR3-B expressed by epithelial and endothelial cells. Binding to CXCR-B inhibits cell migration and stimulates cell apoptosis [59]. CXCL10 has been associated with alterations of neuroendocrine regulation and alterations in cognitive function [60].
The connection between the retinal microvasculature and the brain lies in the concept of the "retina-brain axis".
In a preliminary preprint study, Bramante et al. demonstrated a protective effect of metformin in the development of PCS [65]. Metformin improves endothelial function via increased NO production, preventing endothelial cell injury and reducing leukocyte adhesion [66].
Chronic inflammation is linked to sudden adult death due to atrial fibrillation
C-reactive protein (CRP) is made by the liver and increases when there’s inflammation in the body. A high-sensitivity C-reactive protein (hs-CRP) blood test can be used to evaluate the risk of a heart attack due to coronary artery disease27.
A healthy study published in 2023 by Aviles et al found that CRP is not only associated with the presence of atrial fibrillation (AF), but may also predict patients at increased risk of developing AF in the future.
We need to take the findings from the PET/CT and other studies very seriously.
At baseline, 315 subjects (5%) had AF. Compared with subjects in the first CRP quartile (<0.97 mg/L), subjects in the fourth quartile (>3.41 mg/L) had more AF (7.4% versus 3.7%, adjusted OR 1.8, 95% CI 1.2 to 2.5; P=0.002). Of 5491 subjects without AF at baseline, 897 (16%) developed AF during follow-up. Baseline CRP predicted higher risk for developing future AF (fourth versus first quartile adjusted hazard ratio 1.31, 95% CI 1.08 to 1.58; P=0.005). When treated as a continuous variable, elevated CRP predicted increased risk for developing future AF (adjusted hazard ratio for 1-SD increase, 1.24; 95% CI 1.11 to 1.40; P<0.001).
…Atrial fibrillation (AF) is the most common arrhythmia in clinical practice, affecting 2.3 million people in the United States.1 A major cause of stroke, AF is also associated with a 2-fold increase in mortality.2,3 Although a number of risk factors have been associated with AF, acute or chronic hemodynamic, metabolic, or inflammatory stressors may lead to structural remodeling of the atria that may promote progression and persistence of AF.
…We hypothesized that nonpostoperative forms of AF may also be related to inflammation. Supporting this hypothesis is the observation of inflammatory infiltrates, myocyte necrosis, and fibrosis in atrial biopsies of patients with lone AF refractory to antiarrhythmic drug therapy
From: “Inflammation as a Risk Factor for Atrial Fibrillation” (2003)
mRNA “vaccine” persistence and cardiac involvement
Another study published whilst I was researching this Substack found that synthetic mRNA “vaccine” was detected in the axillary lymph nodes in the majority of patients dying in the 30 days after transfection.
It was also detected in the myocardium of a subset of patients transfected within 30 days of death. Cardiac ventricles in which “vaccine” was detected had more myocardial macrophages than those without “vaccine”.
It was not detected in the mediastinal lymph nodes, spleen or liver.
Hence we have more evidence from pathologists that links the PET/CT study findings with increased risk of death.
From “Duration of SARS-CoV-2 mRNA vaccine persistence and factors associated with cardiac involvement in recently vaccinated patients” by Krauson et al (27th Sept. ‘23)28.
As ever, all these deaths were recorded as natural causes or non-vaccine, prior injury, unrelated. I would have to disagree with this and underreporting must be widespread. Hiding excess deaths isn’t so easy though.
Patients analyzed
Tissues were obtained at autopsy from 20 post-vaccinated patients and 5 non-vaccinated control patients. The patient characteristics are shown in Supplementary Table 1. There were no significant differences between the vaccinated and non-vaccinated groups. In none of the vaccinated patients was the cause of death linked to the vaccine (Supplementary Table 1). Seven of the vaccinated patients had received mRNA-1273 and 13 had received BNT162b2. Six of the vaccinated patients received only one vaccine injection, 12 patients received two injections, and two patients received three injections.
ALN = “axillary lymph nodes”:

Key takes: (emphasis mine)
SARS-CoV-2 mRNA vaccine in the heart is associated with myocardial injury.
While all three of the patients with vaccine in the heart had received BNT162b2, this was not statistically significant. Upon evaluating the histologic slides, none of the patients had myocarditis.
However, all three (100%) of the patients with vaccine in the heart had healing myocardial injury which initiated before or at the time of the most recent vaccine injection compared with only 2 (22%) of the 9 patients without vaccine in the heart (Fig. 3a).
Considering the specific location of the myocardial injury (left ventricle vs right ventricle) in these patients, vaccine was detected in 4 (57%) of 7 ventricles with myocardial injury at the time of vaccination compared with none (0%) of 17 ventricles without myocardial injury at the time of vaccination
Healing myocardial injury is associated with macrophage infiltration of the myocardium. Those patients with vaccine in the heart had more macrophages in the myocardium than those patients dying within 30 days of vaccination without vaccine in the heart (Fig. 3c, d, Supplementary Fig. 1, P = 0.0003, t test).
Although not described as having myocarditis, macrophages with the CD68 protein marker are clinically well recognised as being associated with histiocytic inflammatory myocardial disease (HMID), heart failure and death.
Regardless of historic myocarditis due to comorbidities, the presence of CD68 macrophages at death may well be causative, not just coincidence.
Indeed, the authors here propose that HMID should be recognized as a type of acute myocarditis:

(1) Heart failure with CD68 predominant inflammation (“histiocytic” myocardial inflammatory disease, HMID) occurs with variable clinical presentation and outcome; (2) HMID may be primary or secondary; (3) some cases of HMID show features suggestive of antibody and/or complement mediated myocardial injury, and (4) HMID is a diagnosis distinct from those in classification systems currently in use.
…Myocarditis is an important consideration in the differential diagnosis of unexplained heart failure, and endomyocardial biopsy (EMB) results are integral both in directing treatment and in determining prognosis.
…Since 2019 we have seen 6 cases of fulminant heart failure in which endomyocardial biopsy showed inflammation with an infiltrate composed predominantly of macrophages (histiocytes), identified by immunohistochemistry for CD68.
…Macrophage predominant inflammation may be seen in endomyocardial biopsies of patients with acute heart failure, and we propose that HMID be recognized as one morphological subtype of acute myocarditis that may present in a variety of clinical contexts.

…As only case 1 had angiography showing normal coronary arteries, we cannot completely exclude the possibility that coronary artery disease played a role in the myocardial inflammation and injury that we identified. However, the acute clinical presentations and courses of our cases did not prompt a clinical suspicion of ischemic heart disease, and for this reason we believe that our cases represent acute immune-mediated myocardial injury.
From “The spectrum of macrophage-predominant inflammatory myocardial disease presenting as fulminant heart failure” (2022)
https://www.sciencedirect.com/science/article/abs/pii/S1054880721000776
It won’t come as much surprise that CD68+ macrophage infiltration was significant, as marked by the brown staining in the pathology reports of the transfected (C, left column):

Myocardial LNP infiltration & reperfusion injury
I thought things were dark enough with these findings, but a post about vaccinal lipid nanoparticle (LNP) induced pathologies by @NarfGB prompted me to search on Substack for the involvement of LNPs in myocardial injuries.
The synopsis is that not only can synthetic mRNA agents induce systemic inflammatory immune responses, myocarditis and cardiac arrest they may mediate reperfusion injuries too as the circulation is restored. LNPs may remain in the plasma for at least 2 weeks before being removed by the kidneys or endocytosed into cells2930.
Lacking any therapeutic payload - quite the opposite - an accumulation of LNPs at the site of the damaged myocardium could impede recovery or induce HMID related heart failure.
And if you had “healing myocardial injury” then death could result:
Lipid Nanoparticles (LNPs) are a promising drug delivery vehicle for clinical siRNA delivery. Modified mRNA (modRNA) has recently gained great attention as a therapeutic molecule in cardiac regeneration. However, for mRNA to be functional, it must first reach the diseased myocardium, enter the target cell, escape from the endosomal compartment into the cytosol and be translated into a functional protein. However, it is unknown if LNPs can effectively deliver mRNA, which is much larger than siRNA, to the ischemic myocardium. Here, we evaluated the ability of LNPs to deliver mRNA to the myocardium upon ischemia-reperfusion injury functionally. By exploring the bio-distribution of fluorescently labeled LNPs, we observed that, upon reperfusion, LNPs accumulated in the infarct area of the heart.
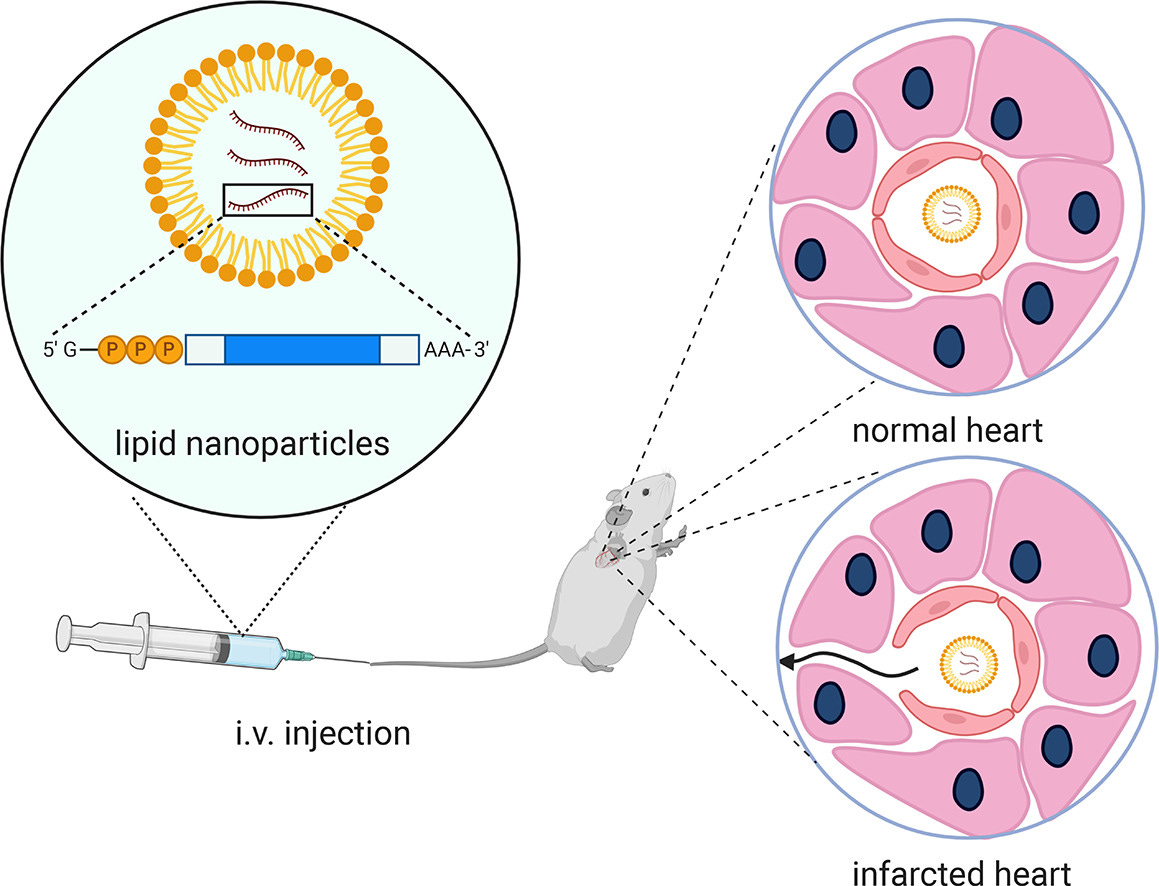
The occlusion of the coronary artery results in vascular endothelium leakage, which enables nanoparticles to extravasate from the circulation in the ischemic area [23]. In line with these findings, we have shown that a lipid-based nanoparticle can access the myocardium after myocardial infarction, probably due to damage-induced vascular permeability: a phenomenon that is not observed in the healthy myocardium [24].
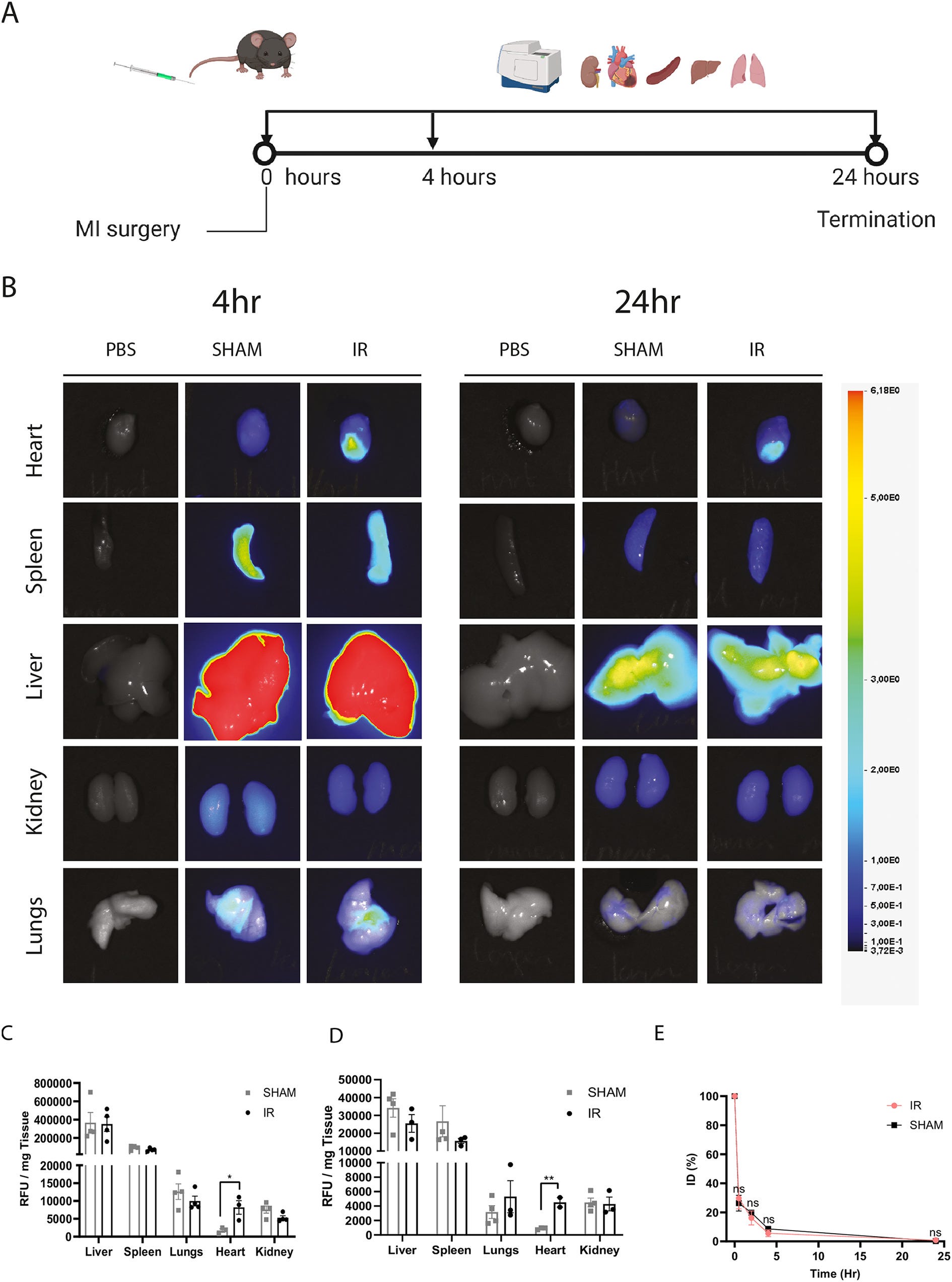
Imaging of indicated organs showed the accumulation of fLNPs in the heart upon ischemia-reperfusion 4 h after administration (Fig. 2B). fLNPs mainly accumulated in the infarcted area just below the region where the left anterior descending artery was occluded. We did not observe any accumulation of LNPs in the heart of sham-operated or control animals.
From: “Delivery of modified mRNA to damaged myocardium by systemic administration of lipid nanoparticles” (2022)
https://www.sciencedirect.com/science/article/pii/S0168365922000414#
We can add those recovering from heart attacks or myocarditis to the list of those who should not be transfected. Along with cancer patients due to the risk of recurrence, and anyone else for that matter.
Cancer risk from chronic and sustained stimulation of the immune system
We know from the PET/CT studies that axillary lymph nodes showed increased metabolic activity for at least six months. Persistent spike protein expression was indicated by histopathologic analyses of various tissues, especially from the excellent work by the late Dr. Arne Burkhardt31.
But to return to our original question - does it matter, does persistent stimulation of the immune system carry with it any long term consequences?
The link between inflammation and cancer is well established, as often the signalling pathways are common to both. We can take interleukin-1 (IL-1), IL-6, IL-17 or tumour necrosis factor (TNF) as examples32.
Activated, proliferating lymphocytes have revealed overlapping metabolic rewiring with neoplastic lymphocytes. Glycolysis is a good example. The difference is that once immune stimulation from antigens and pro-inflammatory cytokines abates the lymphocyte will either undergo apoptosis or return to the prior state as quiescent memory cells.

In contrast a lymphocytic neoplasm, such as leukaemia, lymphoma or myeloma, remains in a permanent proliferative state due to the deregulation of oncogenes and loss of tumour suppressors33.
In 2006, Suarez et al added to these observations by considering the evidence of lymphomas caused by chronic antigenic stimulation by microbial pathogens and/or autoantigens34. Oncogenic viruses such as Epstein-Barr virus (EBV), human herpesvirus 8 (HHV8) and T-lymphotropic virus 1 (HTLV-1) are known to induce lymphoid malignancies. What is less well known is that chronic and sustained stimulation of the immune system also increases the risk of a protracted proliferative state causing lymphoid transformation into lymphoma phenotypes.
This is probably describing the possible long term effects of spike protein stimulation on the axillary lymph nodes.
Illustrated graphically, but with Helicobacter pylori as the source of antigens in A and B. By stage C bacterial antigens are no longer required to sustain the proliferative state. This as a model for a bacterial induced cancer, MALT lymphoma which can be gastric and non-gastric. MALT is derived from mucosa associated lymphoid tissue.
BCR: B-cell receptor
![H pylori and gastric MALT lymphomagenesis paradigm for infection-associated indirect lymphoid transformation. (A) Persisting antigens (Ag's) elicit a polyclonal B-cell response. Costimulation is provided by cytokines and members of the tumor necrosis factor superfamily (CD40-CD40L in T-cell–dependent responses and B-cell activating factor [BAFF]/B-lymphocyte stimulator [BLyS] or a proliferation-inducing ligand [APRIL] produced by dendritic cells in T-cell–independent responses). In the case of H pylori, T cells specific for H pylori epitopes provide help to B cells that recognize cross-reactive autoantigens present in the gastric mucosa such as fucosylated sialyl–Lewis X through CD40-CD40L costimulation. (B) Occurrence of genetic events such as p15 and p16 hypermethylation provide a selective advantage leading to the outgrowth of an antigen-responsive clone. Antigen dependence reflects the requirement for BCR signals such as NF-κB activation (see also Figure 5). (C) Progression toward antigen-independent (therefore antimicrobial-insensitive) MALT lymphoma is associated with the occurrence of additional genetic events. Chromosomal translocations involving MALT1 and Bcl-10 lead to a constitutive activation of NF-κB, bypassing the requirement for BCR-dependent signals (Figure 5). The t(11;18) translocation occurs early during B-cell proliferation and accelerates the transformation process in an antigen-independent fashion. The t(1;14) and t(14;18) translocations also lead to BCR-dependent NF-κB activation, but occur later after an antigen-dependent phase and can be associated with additional cytogenetic abnormalities. The t(3;14) translocation produces an IgH-FoxP1 transcript in 10% of MALT lymphomas that do not harbor other translocations involving the MALT1/Bcl-10 pathway. The precise role of t(3;14) is not known. P53 mutation is associated with transformation to high-grade lymphoma.](https://substackcdn.com/image/fetch/$s_!-YkN!,f_auto,q_auto:good,fl_progressive:steep/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2Fd3631503-57ff-4125-8a18-b2b20e191d2c_1280x848.jpeg "H pylori and gastric MALT lymphomagenesis paradigm for infection-associated indirect lymphoid transformation. (A) Persisting antigens (Ag's) elicit a polyclonal B-cell response. Costimulation is provided by cytokines and members of the tumor necrosis factor superfamily (CD40-CD40L in T-cell–dependent responses and B-cell activating factor [BAFF]/B-lymphocyte stimulator [BLyS] or a proliferation-inducing ligand [APRIL] produced by dendritic cells in T-cell–independent responses). In the case of H pylori, T cells specific for H pylori epitopes provide help to B cells that recognize cross-reactive autoantigens present in the gastric mucosa such as fucosylated sialyl–Lewis X through CD40-CD40L costimulation. (B) Occurrence of genetic events such as p15 and p16 hypermethylation provide a selective advantage leading to the outgrowth of an antigen-responsive clone. Antigen dependence reflects the requirement for BCR signals such as NF-κB activation (see also Figure 5). (C) Progression toward antigen-independent (therefore antimicrobial-insensitive) MALT lymphoma is associated with the occurrence of additional genetic events. Chromosomal translocations involving MALT1 and Bcl-10 lead to a constitutive activation of NF-κB, bypassing the requirement for BCR-dependent signals (Figure 5). The t(11;18) translocation occurs early during B-cell proliferation and accelerates the transformation process in an antigen-independent fashion. The t(1;14) and t(14;18) translocations also lead to BCR-dependent NF-κB activation, but occur later after an antigen-dependent phase and can be associated with additional cytogenetic abnormalities. The t(3;14) translocation produces an IgH-FoxP1 transcript in 10% of MALT lymphomas that do not harbor other translocations involving the MALT1/Bcl-10 pathway. The precise role of t(3;14) is not known. P53 mutation is associated with transformation to high-grade lymphoma.")
We have evidence that MALT lymphoma cases may also start to climb soon. These were previously a rare occurrence. MALT lymphoma in the large intestine usually appears as solitary or multiple elevated or polyploid lesions35.
The median latency period was 5 years according to one study, and it is also associated with an increased risk of new onset metachronous gastric cancer (MGC), relative risk 4.92 (95% CI 2.45-8.79). Gastric adenocarcinoma (GC) is the fourth most common cancer worldwide and the second cause of cancer-related death. It is often diagnosed at an advanced stage and has a low five-year survival rate36.
Hat tip to Dr. Kevin McCairn for featuring this preprint from July ‘23 by Peluso et al: “Multimodal Molecular Imaging Reveals Tissue-Based T Cell Activation and Viral RNA Persistence for Up to 2 Years Following COVID-19”37
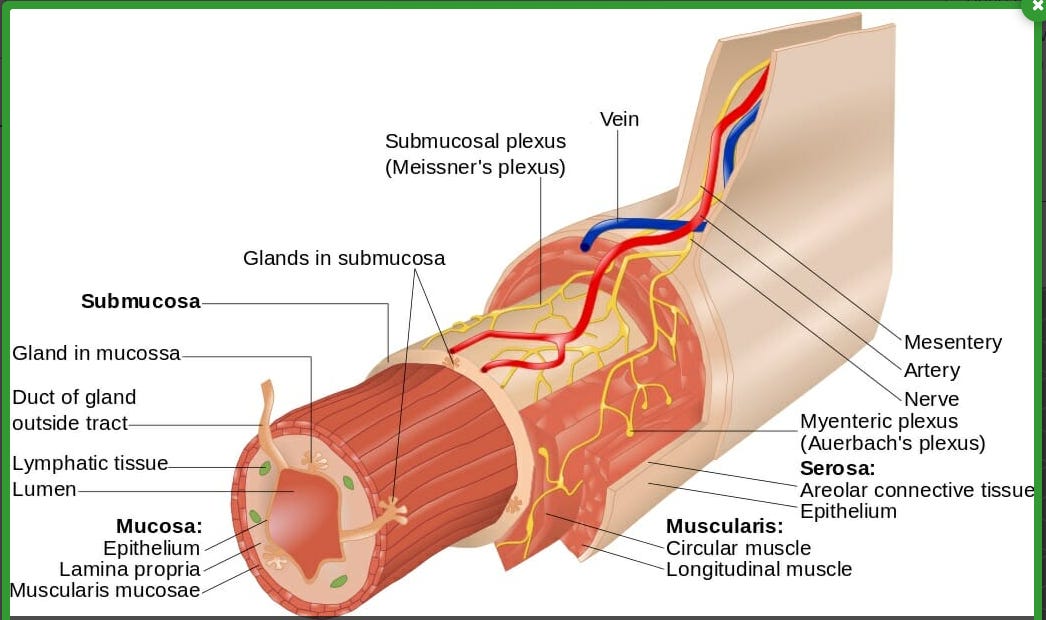
The red flag from this study is where they found the viral mRNA, which included the MALT mucosa associated lymphoid tissues, the rectosigmoid lamina propria.
Rectosigmoid is the lower portion of the sigmoid colon and upper portion of the rectum.
The lamina propria is a large layer of loose connective tissue that fills the spaces between the intestinal glands. It separates the innermost layer of epithelial cells from a layer of smooth muscle, the muscularis mucosa:
The GI tract and intestinal mucosa are also a site of significant HIV replication and CD4+ T-cell destruction38. Indeed there is a MALT lymphoma called “AIDS-Associated MALT Lymphoma” which is a slow growing B-cell non-Hodgkin’s lymphoma (NHL).39
A report from the Italian Cancer Registry covering 1996-2005 gave a 5 year survival rate of 64% of those without HIV vs only 25% for AIDS patients with NHL.40 Immune status has a significant effect on outcomes.
It is important to note that although focused on SARS-CoV-2 viral mRNA they also recorded vax status, including >180 days prior to imaging. Without a non-transfected group this makes studying the impact for potential causative effects challenging.
Key takes from “Multimodal Molecular Imaging Reveals Tissue-Based T Cell Activation and Viral RNA Persistence for Up to 2 Years Following COVID-19”:
We performed whole-body positron emission tomography (PET) imaging in a cohort of 24 participants at time points ranging from 27 to 910 days following acute SARS-CoV-2 infection using a novel radiopharmaceutical agent, [18F]F-AraG, a highly selective tracer that allows for anatomical quantitation of activated T lymphocytes.
Tracer uptake in the post-acute COVID group, which included those with and without Long COVID symptoms, was significantly higher compared to pre-pandemic controls in many anatomical regions, including the brain stem, spinal cord, bone marrow, nasopharyngeal and hilar lymphoid tissue, cardiopulmonary tissues, and gut wall.
Its not AIDS in this case, but HIV is also described as a disease of chronic infection and inflammation41:
Although T cell activation tended to be higher in participants imaged closer to the time of the acute illness, tracer uptake was increased in participants imaged up to 2.5 years following SARS-CoV-2 infection. We observed that T cell activation in spinal cord and gut wall was associated with the presence of Long COVID symptoms.
…tracer uptake in lung tissue was higher in those with persistent pulmonary symptoms.
Even if initially asymptomatic, this is also a marker for chronic infection and inflammation:
Notably, increased T cell activation in these tissues was also observed in many individuals without Long COVID.
Given the high [18F]F-AraG uptake detected in the gut, we obtained colorectal tissue for in situ hybridization SARS-CoV-2 RNA and immunohistochemical studies in a subset of participants with Long COVID symptoms. We identified cellular SARS-CoV-2 RNA in rectosigmoid lamina propria tissue in all these participants, ranging from 158 to 676 days following initial COVID-19 illness, suggesting that tissue viral persistence could be associated with long-term immunological perturbations.
Increased uptake was identified up to 2.5 years following SARS-CoV-2 infection in the absence of known re-infection. Furthermore, [18F]F-AraG uptake in some tissues was associated with a higher number of Long COVID symptoms. Lastly, we identified cellular SARS-CoV-2 RNA in rectosigmoid lamina propria tissue in all participants with Long COVID symptoms who underwent biopsy, ranging from 158 to 676 days following initial COVID-19 symptom onset, suggesting that tissue viral persistence could be associated with these immunologic findings.
Of the 24 participants, all but one were “vaccinated” from 6 to 425 days prior to PET.
The earliest scans were at least 60 days after transfection, apart from 6 days for a participant that hadn’t notified the study team:
Post-hoc investigation of this participant’s PET/CT images revealed similar [18F]F-AraG uptake across all tissue ROIs to other post-acute COVID participants (i.e., was in the middle range of observed SUVmax) and without marked uptake in the deltoid muscle injection site.

From: “Figure 1: [18F]F-AraG PET and PET/CT images from participants following COVID-19 and pre-pandemic control volunteers. Maximum intensity projections (MIP; coronal and sagittal views of 3-dimesional reconstructions) are shown for four representative participants at various times following SARS-CoV-2 infection (a) and male and female uninfected controls (b). Axial PET/CT overlay images are shown in (c) showing increased signal in nasal turbinates, parotid glands, hilar lymph node, lung parenchyma, and lumbar bone marrow in representative post-acute COVID and pre-pandemic control participants (white arrows). MIPs for all participants are shown in Supplemental Figure 1.”, source: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10418298/

Nearly all the RNA was found in cells in the lamina propria. They also found that a small percentage of RNA+ cells expressed CD68+ macrophages.
Case studies
Spike protein induced hyperplasia, aggressive recurrences and turbo-cancer after transfection has been known about almost from the commencement of large scale public campaigns - this case was published in August ‘21.
Hyperplasia is an enlargement of an organ or tissue caused by cell proliferation and an increase in the amount of organic tissue42.
An extension of the lymphatic system the thymus gland is located in the chest behind the sternum. It is most active leading up to puberty and slowly atrophies to be replaced by fatty tissue throughout life.

Its key role is to make and differentiate different T-cells with different roles in the immune system eg CD4+ T helper cells:

We now know from case studies such as this that synthetic spike protein expression is also associated with thymus gland related cancers as well as other blood cancers of the axillary lymph nodes.
The average latency period for second hematologic cancers such as lymphomas and leukaemia was 51 months (~4 years) according to a 2017 study in Argentina43, but the overall range varied from 10 to 110 months. The significance of them being recurrent cancers is that it gives us a definite starting point, which you cannot usually get from a first diagnosis.
If we are going to see transfection and spike protein induced blood cancers in increasing case numbers this should soon start to become apparent. The early signs aren’t good and this report also reminds us of the previous graphs - public health was in rapid decline prior to 2021:
Non-Hodgkin lymphoma European age-standardised (AS) incidence rates for females and males combined increased by 38% in the UK between 1993-1995 and 2016-2018.[1-4] The increase was of a similar size in females and males.
For females, non-Hodgkin lymphoma AS incidence rates in the UK increased by 37% between 1993-1995 and 2016-2018. For males, non-Hodgkin lymphoma AS incidence rates in the UK increased by 35% between 1993-1995 and 2016-2018.
Over the last decade in the UK (between 2006-2008 and 2016-2018), non-Hodgkin lymphoma AS incidence rates for females and males combined increased by 8%. In females AS incidence rates increased by 6%, and in males rates increased by 9%.

From: “Non-Hodgkin lymphoma incidence statistics”. Cancer Research UK. Published May 15, 2015. Accessed October 3, 2023. https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/non-hodgkin-lymphoma/incidence
Physicians were being made aware from as early as April ‘21, after seeing the effects of 2 doses of BNT162b2 on their patients.
An interesting comment about the flu jab too, given the rising trend in lymphoma cases from 1995:
This study shows that avid axillary lymph node uptake at FDG PET/CT can be detected in more than a quarter of our patient population even beyond 6 weeks after the second dose of the mRNA-based COVID-19 vaccination. Compared with a previous study showing normalization of FDG uptake within 40 days of receiving an inactivated H1N1 influenza vaccine (6), we found uptake persistence even at 70 days. Physicians should be aware of this potential pitfall.
From: “Prevalence of Increased FDG PET/CT Axillary Lymph Node Uptake Beyond 6 Weeks after mRNA COVID-19 Vaccination” (2021)
Key takes from “Thymic hyperplasia after mRNA based Covid-19 vaccination” by von Tresckow et al (2021)44:
Reactive lymphadenopathy with increased 18F-Fluordeoxyglucose (FDG) uptake in positron emission tomography (PET)/computed tomography (CT) scans occurs in up to 16% of patients after mRNA vaccination (BNT162B2, mRNA-1273) against severe acute respiratory syndrome coronavirus type 2 (SARS-CoV2). It has not yet been described for the adenoviral vector vaccine JNJ-78436735 [1,2] and only sporadically for AZD1222 [3]. Lymphadenopathy due to vaccination might confound initial disease assessment and restaging thereby hampering optimal therapy in patients with cancer.
Here, we report the case of a 35-year-old female patient who was admitted to our hospital with first diagnosed mantle cell lymphoma (MCL).
No concomitant diseases were known. Patient reported no disease-related complaints and particularly no B symptoms. Physical examination as well as testing of laboratory values showed no pathological findings.
Shortly after diagnosis, the patient was vaccinated with mRNA-1273 in the left upper arm.
10 days after vaccination, an 18F-FDG PET/CT staging displayed moderately increased uptake in the cervical right region, but markedly increased uptake in the axillary left and anterior superior mediastinal regions (Fig. 1). Clinically, the axillary lymphadenopathy disappeared a few days after immunization.

From: “Fig.1 (A) Maximum intensity projection of the patient with only moderate tracer uptake in the detected right cervical mantle cell lymphoma (MCL, dashed arrow, Deauville 3), increased uptake in the thymus (dot-dashed arrow, Deauville 4) and left axillary reactive lymphadenopathy (arrow, Deauville 5), and moderate homogeneous uptake in the reactive bone marrow (asterisk, Deauville 3). (B) Axial CT slice of the same patient with hyperplastic thymus and small left axillary lymph nodes, both regions showing intense tracer uptake in PET/CT fusion (C). (D) Hemalaun and Eosin (HE) stained histological section of thymus showing classic structure of medulla (⋄), cortex (+) and thymic corpuscles (^) and no signs of MCL”, source: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8387216/ Since radiotherapy with curative intent was planned and thymic involvement of MCL would have made localized radiotherapy unfeasible, a diagnostic thymus resection was performed [5]. Histology showed hyperplasia of the thymus without infiltration of the lymphoma (Fig. 1), possibly as an immunologic response to vaccination. Therefore, the patient is referred to local radiotherapy of the affected cervical lymph node region with curative intent.
Our case brought out that markedly increased uptake in 18F-FDG PET/CT scans with temporal association to vaccination with mRNA-based vaccines may occur not only in regional lymph nodes but also in the thymus. In the context of cancer, it is critical to distinguish such immune responses from involvement by malignancy to avoid false positive staging results that may lead to inadequate treatment decisions.

Case reports are coming in daily. This was posted at time of writing and is also a reminder that multiple conditions are going to be encountered more frequently.
This will complicate diagnosis and treatment, in this case of myasthenia gravis (MG) and grade 1 thymus gland cancer. We don’t know her vax status but autoimmune MG is associated with synthetic mRNA gene agents4546.
Woman felt like her 'face was melting' before receiving two life-altering diagnoses
"I was 41 years old, had always been healthy, eaten healthily, never smoked and had no family history of cancer," said Elsa Gavriil, from Hackney, London.
The executive assistant in a tech company first developed an odd cough in January 2022, and then her eyelid drooped.
"I was really struggling after a month to just hold my eyes open," Elsa remembered.
"It was a really weird thing. I was struggling with the sun and lights in the office."
Elsa said the ordeal was "quite difficult" to deal with as she felt as if her face was "melting".
A neurologist diagnosed Elsa with myasthenia gravis, a rare autoimmune condition, but more news was to come.
Following a CT scan, Elsa was also diagnosed with thymus gland cancer - a 4cm tumour had been found between her lungs and behind her sternum.

Somatic mutations: cancer is a continuum
Cancer is a dynamic disease and as it progresses cancers generally become more genetically variable or heterogeneous. This is the fuel for resistance and makes effective treatment all the more challenging47.
There are around 40 trillion cells and 200 different cell types in the human body48 and over 200 different cancer types, each with different features and symptoms being presented49. This doesn’t necessarily equate 1:1 as some tissues have multiple cancer types.
My prior understanding was that all of us, through age, genetic predisposition and lifestyle occasionally generated and acquired aberrant cells with potentially oncogenic mutations. Our cancer immunosurveillance would usually detect these and destroy them, happens every day.
However, some individuals have a familial genetic predisposition that puts them at high risk of breast cancer or lymphoma, for instance, as we saw in an earlier case report. If we didn’t have this risk factor then prolonged stimulation of the lymphatic system shouldn’t be a problem for us, we can cope with it.
Occasionally you come across a paper that turns your understanding on its head and beats you out of your complacency. Perhaps this is just me as I’m not a cancer specialist. But one such paper was published in 2019 by Kennedy et al.
Its called “Cancer-Associated Mutations but No Cancer: Insights into the Early Steps of Carcinogenesis and Implications for Early Cancer Detection”.
Somatic mutations accumulate with age, contribute to cancer and were very difficult to measure within normal, pre-cancerous tissue until the arrival of next-generation sequencing (NGS) and then error-corrected NGS (ecNGS).
The original sequencing of the human genome used Sanger sequencing took over 10 years and cost about a billion dollars50. NGS, on the other hand started with the development of pyrosequencing and was first available commercially by 2005 as the 454/Roche platform. Advantages include being able to sequence large DNA samples in parallel at massive scale and significantly reduced cost and time51.
When they started using NGS to look for somatic mutations they expected to find them in specific cases - the elderly, cancer patients and those with familial cancer genotypes or poor lifestyle choices, i.e. high risk groups. But that’s not what they found.
The gist of it is that there is no shortage of cancer associated mutations in virtually all of us. We even start accumulating them from birth, albeit at a very low level.
Only our immune system and especially the tumour suppressors are holding back the tide - cancer initiation is almost a given if you are deficient in these, sooner or later.
Its as if the removal of a tumour suppressor is equivalent to being exposed to a carcinogen, except that the latent cancer was there all along, via oncogenes.
Which is a BIG problem because of the jab, and the older you are the worse it gets.
See here:
Here we performed bioinformatic analysis to investigate the interaction of S2 subunit protein of SARS-nCoV-2 of novel coronavirus with tumor suppressor proteins p53 and BRCA-1/2. In this short communication we report the interaction between S2 subunit proteins with tumor suppressor proteins for the first time. This preliminary result will open up a new direction to investigate the effect of a novel coronavirus in cancer patients.
From: “S2 Subunit of SARS-nCoV-2 Interacts with Tumor Suppressor Protein p53 and BRCA: an In Silico Study” (2020)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7324311/
https://doorlesscarp953.substack.com/p/s2-subunit-of-sars-ncov-2-interacts
And here:
Results: BRCA1 (Breast Cancer type 1 susceptibility protein) and CXCR4 (a chemokine receptor belonging to the G protein coupled receptor family) were found to exhibit higher binding affinities.-73.82 kcal/mol and -66.45 kcal/mol were the global energies they showed upon binding to S protein respectively.
Conclusion: Therefore, novel SARS-CoV-2 has a higher chance of inducing cancer in non-cancerous individuals and aids in cancer acceleration in cancer patients . This poses a threat to cancer patients and immunocompromised individuals.
From: “SARS-CoV-2 Kerala Isolate Spike Protein Induces Cancer Proliferating Markers for Lung and Breast Cancer: An In Silico Approach” (2022)
https://www.eurekaselect.com/article/123743
https://doorlesscarp953.substack.com/p/sars-cov-2-spike-protein-binding
And especially here, with a prophetic quote calling for mobilisation and mass action due to spike protein molecular mimicry and the generation of autoimmune antibodies to at least 19 different tumour suppressors:
These data are disturbing and invite to immediately intensify clinical surveillance in oncology and to undertake rigid cancer prevention actions, including healthy lifestyle and continuous controls. It will be vital to formulate/implement actions that contemplate fast and safe procedures for clinical trials, development of specific and reliable tumor markers for diagnosis, accurate follow-up of treatments, and, administratively, medical health records, detailed registries, biobanks, health surveys, and coordinated observational studies. Never before do all the recommendations of the European plan for the fight against cancer appear current and necessary. De facto, tumors appear to be the predominant pathologies that will populate the post pandemic long COVID-19.
From: “Anti-Severe Acute Respiratory Syndrome Coronavirus 2 Immune Response to Cancer Onset via Molecular Mimicry and Cross-Reactivity” (2021)
https://doorlesscarp953.substack.com/p/autoantibodies-against-at-least-19

And why we need to be testing for these too:
…anti-tumour suppression gene antigens are detected before the diagnosis of the cancer or in the early stages of the malignant disease, suggesting a potential diagnostic or prognostic role.
From: “Cancer and autoimmunity: autoimmune and rheumatic features in patients with malignancies” (2001)
One hope is that in time, if you limit your exposure to spike protein your tumour suppressors may recover and if you do have any early stage cancers then these could be inhibited.
But hope isn’t a strategy. Viral spike protein or mRNA gene agents aren’t going to disappear any time soon and we need further studies. And spike protein induced BRD4 expression can lead to yet more oncogenic mutations itself:
Key takes from “Cancer-Associated Mutations but No Cancer: Insights into the Early Steps of Carcinogenesis and Implications for Early Cancer Detection52“ (2019), emphasis mine:
Two main features have emerged. First, somatic mutations are highly prevalent, to the extent that it is unlikely for any two somatic cells to have the exact same genome [4].
Second, a large proportion of these mutations occur in cancer genes and harbor signs of positive selection [3], supporting the striking conclusion that ‘clonal evolutionary processes typically thought of as operative only in neoplasia are, in fact, a ubiquitous part of normal aging’ [5].
The first reports of extensive cancer mutations in patients without cancer occurred in 2014 when three groups simultaneously reported mutations in leukemia genes in the blood of ~10% of healthy individuals aged 65 or older [11-13].
Read that twice:
This phenomenon, called clonal hematopoiesis of indeterminate potential (CHIP) [14], was not initially observed in younger individuals. However, the subsequent use of ecNGS revealed the presence of CHIP in 3% of individuals aged 20–29 [15] and 95% of individuals aged 50–60 [16].
Sequencing of induced pluripotent stem cells and single-cell analysis from leukocytes across a wide range of ages (newborn to centenarians) has demonstrated the presence of somatic mutations in cells from all individuals of all ages [17,18]. These mutations often affected genes or loci implicated in cancer, increased near linearly with age, and, in one study [18], were associated with increased risk of leukemia and mortality.
In a groundbreaking report in 2015, Martincorena et al. reported the presence of thousands of clones harboring cancer-associated mutations in normal skin of four individuals aged 55 to 73 [19], demonstrating that the phenomenon is not limited to the hematopoietic compartment.
Mutations in the TP53 gene were found at a very low level (~0.01%) in all the women they tested, aged 32-85, with and without ovarian cancer.
By “positively selected” they mean that throughout life TP53 mutations progressively transition from being evenly distributed throughout the gene to forming clustered cancer-like mutations, through cumulative selection:
…their frequency increased with age. In addition, these mutations were primarily nonsynonymous, clustered in common TP53 mutational hotspots, and were frequently predicted to be inactivating, strongly suggesting that they were positively selected.
We are all sitting on a potential cancer time bomb. It makes me look at my own health in a different light:
Since the publication of these initial reports, several additional studies have documented the presence of cancer-associated mutations in a variety of normal solid tissues and benign conditions, including esophagus [23,24], colon [25], brain [26], endometrium [27-30], several gynecological tissues [29], and a comprehensive set of 29 human tissues [31]. These findings are quickly expanding and reshaping our understanding of human carcinogenesis.

The authors then ask:
Given the high frequency of positively selected clones in normal tissue, why is clinically diagnosed cancer not more common in the human population?
One reason is extremely robust tumour suppressor mechanisms:
A possible explanation relies on the action of tumor suppressor mechanisms, which can be viewed as nature’s solution to prevent cancer formation in multicellular organisms [38]. Malignant transformation requires the bypass of tumor suppressor mechanisms operating in a given tissue at a given time. These include, among others, contact inhibition, senescence, and immune surveillance (Figure 1).
The high prevalence of cancer-associated mutations in the absence of apparent cancer suggests that their occurrence is not rate limiting to tumor formation.
This is why its alarming to have needle-induced population level impairment of tumour suppression mechanisms:
Moreover, the observed presence of cancer-associated mutations in early life indicates that these mutations can exist for long periods of time without ever converting to overt disease, suggesting that tumor suppression mechanisms must be far more effective and multifactorial than generally appreciated.
Of note, while tumor suppressor mechanisms are remarkably successful in preventing cancer in early life, their efficiency might decrease later in life, contributing to the increased incidence of cancer at older age.
Tumor suppressor mechanisms are critical to stop the progression of mutated clones. The weakening of these mechanisms at late age and/or the bypass by additional mutations renders pre-existing clones susceptible to malignant transformation.
“If I were you, I wouldn’t start from here”
Another biological implication they make is that cancer is a continuum - an ongoing process of accumulating and positively selecting somatic mutations which often precede symptomatic disease for far longer and more gradually than was initially thought:
In a seminal paper, Vogelstein and colleagues synthesized years of work involving both histopathological and clinical data to argue that mutations leading to colon cancer accrue during sequential rounds of clonal selection years prior to diagnosis. They further hypothesized that this is a generalized phenomenon for carcinogenesis [49]. The current spate of sequencing data supports these early hypotheses, but indicates that the path to carcinogenesis is far longer, more pervasive, and more gradual than theory initially predicted. Moreover, new insights suggest that a large fraction of cells, and not just a small population, exist along this continuum.
Epigenetic choice of destination?
Don’t just blame your genes, get proactive and do something about it:
Perhaps the most important clinical implication derived from the findings of clonal evolution within normal tissue is that cancer-associated mutations, or at least a subset of them, are not specific for cancer.
And there is clinical evidence to support their hypothesis:
Additional evidence for the prognostic value of clonal expansions comes from recent deep sequencing studies in preleukemic samples. In patients that developed acute myeloid leukemia (AML), blood biopsies collected more than 5 years prior to diagnosis were already enriched for mutations in AML-associated genes and carried large clonal expansions [65,66]. It is possible, however, that blood mutations could inform not only about the risk of hematological malignancies, but solid cancers as well.
There is a caution though. NGS also increases the risk of conducting unnecessary prophylactic surgery53 and complicates treatment options. It could even become a cash cow for the unscrupulous54.
MCED, or multi-cancer early detection is a methylation based variation of this. MCED looks for cell-free DNA (cfDNA) tumour signals for 50+ types of cancer55. Screening appears to be the Next Big Thing:
More immediate concerns arise due to the rapidly expanding field of clinical sequencing. The presence of these mutations complicates the utility of these applications. Premature deployment without proper care will likely lead to unacceptably high false positive rates, with potentially disastrous consequences for patients.

From: “Features of Cancer Mutations in Normal Tissue (A), Identified Challenges (B), and Potential Solutions (C).”, source: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8765002/

BHF & BS - mind your BP!
Given the safety-first precautionary principle you might think that the “British Heart Foundation” would be singing a different tune, or at least taking down their web pages and hiding under a large rock in shame.


But no, the BHF are still trying to drum up new business, as it were:

Nothing is off-limits, apart from the truth:

Even Pfizer are more honest about their product than the heart charity is, and that’s saying something.
From the Comirnaty (BNT162b2) UK patient information leaflet:
There is an increased risk of myocarditis (inflammation of the heart muscle) and pericarditis (inflammation of the lining outside the heart) after vaccination with Comirnaty (see section 4). These conditions can develop within just a few days after vaccination and have primarily occurred within 14 days. They have been observed more often after the second vaccination, and more often in younger males. The risk of myocarditis and pericarditis seems lower in children ages 5 to 11 years compared with ages 12 to 17 years. Most cases of myocarditis and pericarditis recover. Some cases required intensive care support and fatal cases have been seen. Following vaccination, you should be alert to signs of myocarditis and pericarditis, such as breathlessness, palpitations and chest pain, and seek immediate medical attention should these occur.
From: “Package leaflet: Information for the user Comirnaty 30 micrograms/dose concentrate for dispersion for injection Adults and adolescents from 12 years COVID-19 mRNA Vaccine (nucleoside modified) tozinameran”
They are happy to leave you in ignorance about cardiac damage caused by other shots too56:
Is there a risk of cardiac arrest from the Covid vaccine?
No. There is no evidence that people are at an increased risk of cardiac arrest in the days or weeks following the Covid-19 vaccine.
Do other vaccines carry a risk of myocarditis?
Research published in The Lancet medical journal in April 2022 shows that there is no greater risk of developing heart inflammation after a Covid-19 vaccine than after other common vaccines, including the flu jab.
Researchers from Singapore looked at the findings of 22 different studies, covering 405 million doses of different vaccines around the world – including flu, smallpox, polio, measles, mumps and rubella. Overall the rates of myocarditis and pericarditis following Covid vaccines weren’t significantly different to other vaccines, including flu, although rates of myocarditis or pericarditis in young men were higher following mRNA-based Covid vaccines such as Moderna or Pfizer.
The researchers, writing in The Lancet medical journal, suggested that the rare cases of post-vaccine myocarditis and pericarditis might be connected to the overall immune response to vaccination, not specifically because of the Covid-19 vaccination or the spike protein it is based on. They suggested that the reports of myocarditis and pericarditis might be because of the large scale of Covid-19 vaccination and the close scrutiny it has had.
Based on these findings, the researchers said that the benefits of Covid-19 vaccines (including a reduced risk of severe illness or death) far outweigh the very small risk of myocarditis or pericarditis, which is also seen for other vaccines.
Are children at higher risk of heart inflammation from the vaccine?
Cases of heart inflammation (myocarditis or pericarditis) after the vaccine in children and young people are rare. Overall the rate is lower in children than in adults aged 18-39.
The independent Medicines and Healthcare products Regulatory Agency (MHRA) has reviewed all the evidence and confirmed the Pfizer vaccine is safe and effective for children aged 5 and over.
From: “Myocarditis and Covid-19 vaccines: should you be worried?” (June ‘23)

But it all becomes clear, - if as alleged you have signed NDAs to keep your paymasters happy, then you become their bitches. Shame on you, BHF.
A charity has hit back at claims by a Leicestershire MP that it covered up data on the harm caused by Covid-19 vaccines. The British Heart Foundation (BHF) dismissed the allegations made by Andrew Bridgen where he insisted a senior figure in the charity was part of the cover-up.
The North West Leicestershire MP made the claims during a debate in the House of Commons. The MP, who is double-vaccinated himself, said the leading charity had hidden figures which showed the vaccine led to an inflammation of the heart arteries over fears it could lose funding from the pharmaceutical industry.
* * *
The MP's allegations against the BHF were among his strongest comments yet, insisting leading figures were hiding the truth. He said: “It is covering this up for fear that it may lose funding from the pharmaceutical industry. The lead of that cardiology research department has a prominent leadership role with the British Heart Foundation, and I am disappointed to say that he has sent out non-disclosure agreements to his research team to ensure that this important data never sees the light of day. That is an absolute disgrace.”
From: “British Heart Foundation dismisses Covid-19 'cover up' claims made by Leicestershire MP” (Dec ‘22).
https://www.leicestermercury.co.uk/news/health/british-heart-foundation-dismisses-covid-7980462

The BHF is emblematic of many broken institutions. Until we clean house, progress is going to be slow and many doctors, patients and associates will continue to be baffled as case counts continue to climb.
Conclusion
We now have overwhelming evidence of iatrocide from research, case studies, VAERS reports, daily news reports and even warnings from the pharma companies too. The lab modified viruses aren’t off the hook either, by any means.
Experimental mRNA gene agents are associated with more frequent breakthrough infections, antagonism of tumour suppressors and long term persistent expression in the gastrointestinal tract and axillary lymph nodes in particular. This is marked clinically by chronic inflammation and a patho book full of other conditions, especially cardiovascular disease and cancer. PET/CT is a useful diagnostic tool.

References
Buergin N, Lopez-Ayala P, Hirsiger JR, et al. Sex-specific differences in myocardial injury incidence after COVID-19 mRNA-1273 booster vaccination. European Journal of Heart Failure. n/a(n/a). doi:10.1002/ejhf.2978
Xu RY, Zhu XF, Yang Y, Ye P. High-sensitive cardiac troponin T. J Geriatr Cardiol. 2013;10(1):102-109. doi:10.3969/j.issn.1671-5411.2013.01.015
Al-Akchar M, Shams P, Kiel J. Acute Myocarditis. In: StatPearls. StatPearls Publishing; 2023. Accessed October 6, 2023. http://www.ncbi.nlm.nih.gov/books/NBK441847/
Dr. Janci [@JanciToxDoc]. In a study of 700 COVID vaxxed compared to 300 unvaxxed even asymptomatic COVID vaxxed showed indications of myocarditis by FDG uptake on PET CT https://t.co/AUgXocYh2C. Twitter. Published September 24, 2023. Accessed September 25, 2023.
Treglia G, Cuzzocrea M, Muoio B, Elzi L. PET findings after COVID-19 vaccination: “Keep Calm and Carry On.” Clin Transl Imaging. 2021;9(3):209-214. doi:10.1007/s40336-021-00430-3
Goldman S, Bron D, Tousseyn T, et al. Rapid Progression of Angioimmunoblastic T Cell Lymphoma Following BNT162b2 mRNA Vaccine Booster Shot: A Case Report. Frontiers in Medicine. 2021;8. Accessed September 27, 2023. https://www.frontiersin.org/articles/10.3389/fmed.2021.798095
Nakahara T, Iwabuchi Y, Miyazawa R, et al. Assessment of Myocardial 18F-FDG Uptake at PET/CT in Asymptomatic SARS-CoV-2-vaccinated and Nonvaccinated Patients. Radiology. 2023;308(3):e230743. doi:10.1148/radiol.230743
Fluorine-18 - Wikipedia
Positron - Wikipedia
Ardito F, Giuliani M, Perrone D, Troiano G, Lo Muzio L. The crucial role of protein phosphorylation in cell signaling and its use as targeted therapy (Review). International Journal of Molecular Medicine. 2017;40(2):271-280. doi:10.3892/ijmm.2017.3036
Rajas F, Gautier-Stein A, Mithieux G. Glucose-6 Phosphate, a Central Hub for Liver Carbohydrate Metabolism. Metabolites. 2019;9(12):282. doi:10.3390/metabo9120282
ZHENG J. Energy metabolism of cancer: Glycolysis versus oxidative phosphorylation (Review). Oncol Lett. 2012;4(6):1151-1157. doi:10.3892/ol.2012.928
Liberti MV, Locasale JW. The Warburg Effect: How Does it Benefit Cancer Cells? Trends Biochem Sci. 2016;41(3):211-218. doi:10.1016/j.tibs.2015.12.001
Substack. Moriarty | Substack. Accessed September 27, 2023. https://substack.com/@hiddencomplexity
Substack. Jennifer Depew, R.D. | Substack. Accessed September 27, 2023. https://substack.com/@denutrients
Suhail S, Zajac J, Fossum C, et al. Role of Oxidative Stress on SARS-CoV (SARS) and SARS-CoV-2 (COVID-19) Infection: A Review. Protein J. 2020;39(6):644-656. doi:10.1007/s10930-020-09935-8
Chaaban N, Kshatriya S, ya. Myocarditis on 18FDG-PET imaging. Radiol Case Rep. 2022;17(6):2120-2122. doi:10.1016/j.radcr.2022.03.074
Ashraf MA, Goyal A. Fludeoxyglucose (18F). In: StatPearls. StatPearls Publishing; 2023. Accessed September 26, 2023. http://www.ncbi.nlm.nih.gov/books/NBK557653/
Gambhir SS. Molecular imaging of cancer with positron emission tomography. Nat Rev Cancer. 2002;2(9):683-693. doi:10.1038/nrc882
FERES M, FERES MFN. Absence of evidence is not evidence of absence. J Appl Oral Sci. 31:ed001. doi:10.1590/1678-7757-2023-ed001
Koksal D, Demirag F, Bayiz H, et al. The correlation of SUVmax with pathological characteristics of primary tumor and the value of Tumor/ Lymph node SUVmax ratio for predicting metastasis to lymph nodes in resected NSCLC patients. J Cardiothorac Surg. 2013;8:63. doi:10.1186/1749-8090-8-63
Patone M, Mei XW, Handunnetthi L, et al. Risk of Myocarditis After Sequential Doses of COVID-19 Vaccine and SARS-CoV-2 Infection by Age and Sex. Circulation. 2022;146(10):743-754. doi:10.1161/CIRCULATIONAHA.122.059970
Calvo F, Karras BT, Phillips R, Kimball AM, Wolf F. Diagnoses, Syndromes, and Diseases: A Knowledge Representation Problem. AMIA Annu Symp Proc. 2003;2003:802.
Giannitsi S, Bougiakli M, Bechlioulis A, Naka K. Endothelial dysfunction and heart failure: A review of the existing bibliography with emphasis on flow mediated dilation. JRSM Cardiovasc Dis. 2019;8:2048004019843047. doi:10.1177/2048004019843047
Yin X, Wang Z, Wu T, et al. The combination of CXCL9, CXCL10 and CXCL11 levels during primary HIV infection predicts HIV disease progression. J Transl Med. 2019;17:417. doi:10.1186/s12967-019-02172-3
Asensio VC, Maier J, Milner R, et al. Interferon-Independent, Human Immunodeficiency Virus Type 1 gp120-Mediated Induction of CXCL10/IP-10 Gene Expression by Astrocytes In Vivo and In Vitro. J Virol. 2001;75(15):7067-7077. doi:10.1128/JVI.75.15.7067-7077.2001
Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;140(11). doi:10.1161/CIR.0000000000000678
Krauson AJ, Casimero FVC, Siddiquee Z, Stone JR. Duration of SARS-CoV-2 mRNA vaccine persistence and factors associated with cardiac involvement in recently vaccinated patients. npj Vaccines. 2023;8(1):1-8. doi:10.1038/s41541-023-00742-7
Fertig TE, Chitoiu L, Marta DS, et al. Vaccine mRNA Can Be Detected in Blood at 15 Days Post-Vaccination. Biomedicines. 2022;10(7):1538. doi:10.3390/biomedicines10071538
Hald Albertsen C, Kulkarni JA, Witzigmann D, Lind M, Petersson K, Simonsen JB. The role of lipid components in lipid nanoparticles for vaccines and gene therapy. Adv Drug Deliv Rev. 2022;188:114416. doi:10.1016/j.addr.2022.114416
Bhakdi S, Burkhardt A. On COVID vaccines: why they cannot work, and irrefutable evidence of their causative role in deaths after vaccination. https://doctors4covidethics.org/wp-content/uploads/2021/12/end-covax.pdf
Singh N, Baby D, Rajguru JP, Patil PB, Thakkannavar SS, Pujari VB. Inflammation and Cancer. Ann Afr Med. 2019;18(3):121-126. doi:10.4103/aam.aam_56_18
Altman BJ, Dang CV. Normal and cancer cell metabolism: lymphocytes and lymphoma. The FEBS Journal. 2012;279(15):2598-2609. doi:10.1111/j.1742-4658.2012.08651.x
Suarez F, Lortholary O, Hermine O, Lecuit M. Infection-associated lymphomas derived from marginal zone B cells: a model of antigen-driven lymphoproliferation. Blood. 2006;107(8):3034-3044. doi:10.1182/blood-2005-09-3679
Akasaka R, Chiba T, Dutta AK, et al. Colonic Mucosa-Associated Lymphoid Tissue Lymphoma. Case Rep Gastroenterol. 2012;6(2):569-575. doi:10.1159/000342726
Palmela C, Fonseca C, Faria R, Baptista RB, Ribeiro S, Ferreira AO. Increased risk for metachronous gastric adenocarcinoma following gastric MALT lymphoma-A US population-based study. United European Gastroenterol J. 2017;5(4):473-478. doi:10.1177/2050640616671643
Peluso MJ, Ryder D, Flavell R, et al. Multimodal Molecular Imaging Reveals Tissue-Based T Cell Activation and Viral RNA Persistence for Up to 2 Years Following COVID-19. medRxiv. Published online July 31, 2023:2023.07.27.23293177. doi:10.1101/2023.07.27.23293177
Clayton F, Reka S, Cronin WJ, Torlakovic E, Sigal SH, Kotler DP. Rectal mucosal pathology varies with human immunodeficiency virus antigen content and disease stage. Gastroenterology. 1992;103(3):919-933. doi:10.1016/0016-5085(92)90026-u
AIDS-Associated MALT Lymphoma. DoveMed. Accessed October 4, 2023. http://www.dovemed.com/diseases-conditions/aids-associated-malt-lymphoma/
Re A, Cattaneo C, Rossi G. Hiv and Lymphoma: from Epidemiology to Clinical Management. Mediterr J Hematol Infect Dis. 2019;11(1):e2019004. doi:10.4084/MJHID.2019.004
HIV and Inflammation. International Association of Providers of AIDS Care. Accessed October 4, 2023. https://www.iapac.org/fact-sheet/hiv-and-inflammation/
Hyperplasia - Wikipedia
Felice MS, Rossi JG, Alonso CN, et al. Second Neoplasms in Children Following a Treatment for Acute Leukemia and/or Lymphoma: 29 Years of Experience in a Single Institution in Argentina. J Pediatr Hematol Oncol. 2017;39(8):e406-e412. doi:10.1097/MPH.0000000000000971
von Tresckow J, von Tresckow B, Reinhardt HC, Herrmann K, Berliner C. Thymic hyperplasia after mRNA based Covid-19 vaccination. Radiol Case Rep. 2021;16(12):3744-3745. doi:10.1016/j.radcr.2021.08.050
Papadopoulou M, Stefanou MI, Palaiodimou L, Tsivgoulis G. Myasthenia Gravis Exacerbation Following Immunization With the BNT162b2 mRNA COVID-19 Vaccine: Report of a Case and Review of the Literature. Neurohospitalist. 2023;13(3):303-307. doi:10.1177/19418744231158161
Ishizuchi K, Takizawa T, Sekiguchi K, et al. Flare of myasthenia gravis induced by COVID-19 vaccines. Journal of the Neurological Sciences. 2022;436:120225. doi:10.1016/j.jns.2022.120225
Dagogo-Jack I, Shaw AT. Tumour heterogeneity and resistance to cancer therapies. Nat Rev Clin Oncol. 2018;15(2):81-94. doi:10.1038/nrclinonc.2017.166
Weeden CE, Hill W, Lim EL, Grönroos E, Swanton C. Impact of risk factors on early cancer evolution. Cell. 2023;186(8):1541-1563. doi:10.1016/j.cell.2023.03.013
National Collaborating Centre for Cancer (UK). Suspected Cancer: Recognition and Referral. National Institute for Health and Care Excellence (NICE); 2015. Accessed October 3, 2023. http://www.ncbi.nlm.nih.gov/books/NBK304993/
Reuter JA, Spacek D, Snyder MP. High-Throughput Sequencing Technologies. Mol Cell. 2015;58(4):586-597. doi:10.1016/j.molcel.2015.05.004
Akintunde O, Tucker T, Carabetta VJ. The evolution of next-generation sequencing technologies. ArXiv. Published online May 15, 2023:arXiv:2305.08724v1.
Kennedy SR, Zhang Y, Risques RA. Cancer-Associated Mutations but No Cancer: Insights into the Early Steps of Carcinogenesis and Implications for Early Cancer Detection. Trends Cancer. 2019;5(9):531-540. doi:10.1016/j.trecan.2019.07.007
Alaofi RK, Nassif MO, Al-Hajeili MR. Prophylactic mastectomy for the prevention of breast cancer: Review of the literature. Avicenna J Med. 2018;8(3):67-77. doi:10.4103/ajm.AJM_21_18
Christensen KD, Dukhovny D, Siebert U, Green RC. Assessing the Costs and Cost-Effectiveness of Genomic Sequencing. J Pers Med. 2015;5(4):470-486. doi:10.3390/jpm5040470
Klein EA, Richards D, Cohn A, et al. Clinical validation of a targeted methylation-based multi-cancer early detection test using an independent validation set. Annals of Oncology. 2021;32(9):1167-1177. doi:10.1016/j.annonc.2021.05.806
Engler RJM, Nelson MR, Collins LC, et al. A prospective study of the incidence of myocarditis/pericarditis and new onset cardiac symptoms following smallpox and influenza vaccination. PLoS One. 2015;10(3):e0118283. doi:10.1371/journal.pone.0118283

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Prof Angus Dalgleish discusses case reports of aggressive melanomas, B-cell lymphoma, myeloma, aggressive colorectal cancer; igG4 class switching, suppression of autopsies, vaccinal spike mRNA & spike protein in a biopsy of an aggressive colon cancer.
***
Jikkyleaks 🐭
@Jikkyleaks
This is an absolutely incredible interview between
@Johnincarlisle
and Prof Angus Dalgleish, an oncologist with more than 500 papers.
One of the rare doctors with molecular biology experience.
He explains how the UK government has silenced him.
https://youtu.be/PnJ5T1Enwq4
Thanks DC...it will take me all weekend to wade through this.
Also, +1 for "poorly bits."